Article Text

Abstract
Objectives: To examine trends in the prevalence of diagnosed atrial fibrillation (AF), its treatment with oral anticoagulants between 1994 and 2003, and predictors of anticoagulant treatment in 2003.
Methods: Analysis of electronic data from 131 general practices (about one million registered patients annually) contributing to the DIN-LINK database.
Results: From 1994 to 2003 the prevalence of “active” AF rose from 0.78% to 1.31% in men and from 0.79% to 1.15% in women. The proportion of patients with AF taking anticoagulants rose from 25% to 53% in men and from 21% to 40% in women. Most others received antiplatelets. The likelihood of receiving anticoagulants was greater for men and with increasing stroke risk. It decreased sharply with age after 75 years. Socioeconomic status, urbanisation and region had no influence. Non-steroidal anti-inflammatory drugs, antiplatelet drugs and ulcer healing drugs were associated with reduced likelihood of receiving anticoagulants, as were peptic ulcers, chronic gut disorders, anaemias, psychoses and poor compliance. Anticoagulant treatment was associated with several cardiovascular co-morbidities and drugs, possibly due to secondary care treatment. Nevertheless, only 56.5% of patients at very high risk of stroke were taking anticoagulants in 2003, whereas 38.2% of patients at low risk of stroke received anticoagulants.
Conclusions: This study confirms previously observed trends of increasing AF prevalence and warfarin treatment. Many patients who may benefit from anticoagulation still do not receive it, whereas others at lower risk of stroke do. The lower likelihood of women receiving anticoagulants is of particular concern.
- ACORN, A Classification of Residential Neighbourhoods
- AF, atrial fibrillation
- NSAIDs, non-steroidal anti-inflammatory drugs
- OR, odds ratio
- atrial fibrillation
- anticoagulation
- co-morbidities
- prevalence
- stroke risk
Statistics from Altmetric.com
- ACORN, A Classification of Residential Neighbourhoods
- AF, atrial fibrillation
- NSAIDs, non-steroidal anti-inflammatory drugs
- OR, odds ratio
The use of oral anticoagulants (mainly warfarin) to reduce the risk of thrombotic stroke by patients with atrial fibrillation (AF) is generally acknowledged to be a major advance in preventing this devastating complication.1–3 Despite this, many patients who may benefit from its use do not receive it.4 Research into why this should be has been limited. Warfarin has intensive monitoring requirements, and many drug and disease interactions, cautions and contraindications. The risk of causing dangerous bleeding episodes and other issues mean that decisions regarding its use are complex. Guidelines to assist treatment decisions by stratifying patients with AF by stroke risk have been published and may be an important influence on clinicians, although this has not been fully evaluated.5,6 Antiplatelet drugs are an alternative to warfarin, although less effective.
A literature review of factors associated with the non-prescription of warfarin found that the most common reason for warfarin underuse is the clinical perception that patients will not comply with treatment.7 Other studies have suggested that advanced age, rural location, walking ability, susceptibility to falls, and both cognitive and functional impairments are common reasons for patients not receiving warfarin.8,9 Patient preference is an important factor, with less than 50% of eligible patients in one study agreeing to warfarin when the risks and benefits had been fully explained to them.10 In a qualitative study, UK general practitioners disagreed over the evidence for anticoagulation, expressed concerns over the influence of secondary care doctors in starting such treatment, and regarded shared decision making with patients as being more important than adherence to prescriptive guidelines.11
The prevalence of diagnosed AF appears to be increasing.4 It is most important to understand the issues influencing treatment decisions in stroke prevention. This study examined trends in the prevalence of diagnosed AF and of treatment to prevent stroke between 1994 and 2003. It examined the influence of a range of factors, including stroke risk, on the likelihood of anticoagulant prescription in UK general practice in 2003.
METHODS
DIN-LINK
DIN-LINK (formerly DIN) is an ongoing anonymised computerised UK primary care database from practices that use iSOFT (formerly Torex) software (iSOFT Group plc, Manchester, UK) from 1989 onwards. This report is based on 131 practices that run an updated version of the software used in an earlier version of the database, previously described.12,13 We have outlined methods for identifying good-quality data in DIN-LINK,12 and this approach was repeated with the updated database. The final practices selected had to provide at least five years of continuous high-quality data.
The completeness and accuracy of DIN-LINK data for coronary heart disease have been validated by comparisons with other national data sources, including the Health Survey for England and the General Practice Research Database.14 DIN-LINK has also been shown to provide similar prevalence to other general practitioner databases for a wide range of conditions.12,13 Morbidity and drug data are coded by Read codes. An important aspect of the database is the availability of a postcode-level sociodemographic indicator, the ACORN index,15 which uses data from the 2001 census to classify postcodes. Multiple levels of aggregation of the index are available but commonly the most aggregated level, a five-level classification from “wealthy achievers” through to “hard pressed”, is used. ACORN scores were available for most patients in 125 of the 131 practices. The UK region and urban/rural status of each practice is also known.
Patients
Patients were included in a given year if they remained registered on 31 December of that year and for six months previously. Patients with diagnosed AF were identified by searching for the presence of appropriate Read codes in the records. Prescriptions were identified for oral anticoagulants, antiplatelet drugs and drugs listed in the British National Formulary (number 48–2004) as having known significant interactions with warfarin. Read coded co-morbidities, absolute and relative disease contraindications to warfarin and risk factors for stroke were also extracted (see web table 1 on the Heart website for all Read codes used—http://www.heartjnl.com/supplemental).
Predictive factors for oral anticoagulant (OA) use by 12267 patients ⩾35 years old with active atrial fibrillation in 2003
Presence of AF in a given year
AF differs from some other chronic conditions in that it may be intermittent and may be treated by drug or electrical cardioversion or radiofrequency ablation to restore sinus rhythm, at least temporarily. Patients so treated have not generally been thought to require further treatment with warfarin while in sinus rhythm, although this is now debated.16
Whereas it is straightforward to identify patients who have ever been in AF from DIN-LINK and similar databases, it is less easy to identify patients who have returned to sinus rhythm, but may go back into AF again. Other studies have not addressed this issue. We have done so by developing a computer algorithm (details available on request from the authors) through an iterative process of comparison and validation with the DIN-LINK patient records. Each year this took patients who had previously had an AF diagnosis and looked for the latest occurrence in the year of a code from each of two groups of drug and clinical codes. One group suggested cardioversion treatment or presence of sinus rhythm and the other suggested return to AF, either by the presence of an appropriate clinical code or by digoxin or anticoagulant drug use. The time interval between the appearance of a code from each of the groups was also used to refine the decision about whether a patient had ended the year in “active” AF. A patient can be inactive one year and become active in a following year and so on. In this paper, prevalence trends are presented for patients with AF ever and patients with active AF, but other analyses are presented for patients with active AF only, although both analyses were carried out.
Stroke risk
The stroke risk stratification scheme used here is that contained in the PRODIGY guidance. PRODIGY is clinical decision support software available nationally to general practitioners through their clinical computer systems.17 The PRODIGY guidance on anticoagulation in AF stratifies patients from low to very high risk of stroke according to clinical criteria very similar to other schemes such as CHADS2 (congestive heart failure, hypertension, age > 75, diabetes mellitus, and prior stroke or transient ischemic attack).6 The clinical criteria are age; history of stroke or transient ischaemia; and the presence of hypertension, diabetes, heart failure or left ventricular dysfunction. This scheme was used to allocate all patients identified to have AF to a stroke risk.
Statistical methods
Factors predicting the prescribing of oral anticoagulants in 2003 for patients with active AF were analysed by logistic regression with the individual patient as the unit of analysis and adjusted for practice by fitting a dummy variable for each included practice. This has the effect of adjusting for region and urban/rural differences too, as these factors are confounded with practice. Factors that were investigated were sex, age, ACORN score (including a missing category) and PRODIGY risk score. All logistic regressions were analysed by PROC LOGISTIC in SAS V.8.1 for Solaris (SAS Institute, Cary, North Carolina, USA).
Further logistic regressions were analysed by examining the influence of the presence of the following: a total of 25 co-morbid conditions (ever), 9 contraindicating conditions (ever) and 12 drug cautions (prescribed at any time in 2003). (These are listed in web table 1 on the Heart website—http://www.heartjnl.com/supplemental.) A final model incorporating all of these factors was chosen by using a stepwise procedure in PROC LOGISTIC, with cut offs for entry and exit of variables set at p = 0.01.
Regional and urban/rural differences were analysed by fitting a hierarchical model with PROC MIXED in SAS, with practices being at level 2 and individual patients at level 1. Explanatory variables from the previous logistic model (sex, age group, ACORN and PRODIGY risk score) were fitted as fixed effects at the patient level, and the practice urban/rural status and its region were fitted as a fixed effect at practice level. A random effect for practice was fitted to model the variation across practices.
RESULTS
The 131 DIN-LINK practices in this report average in total one million registered patients per year between 1994 and 2003. ACORN data were available for 98.5% of patients in 2003.
Not all of the 131 practices had data available for every year between 1994 and 2003, due to some entering and leaving DIN-LINK and to data quality issues in earlier years. Restricting the analysis to the same pool of practices over time had no notable effect on the results.
Prevalence of diagnosed AF
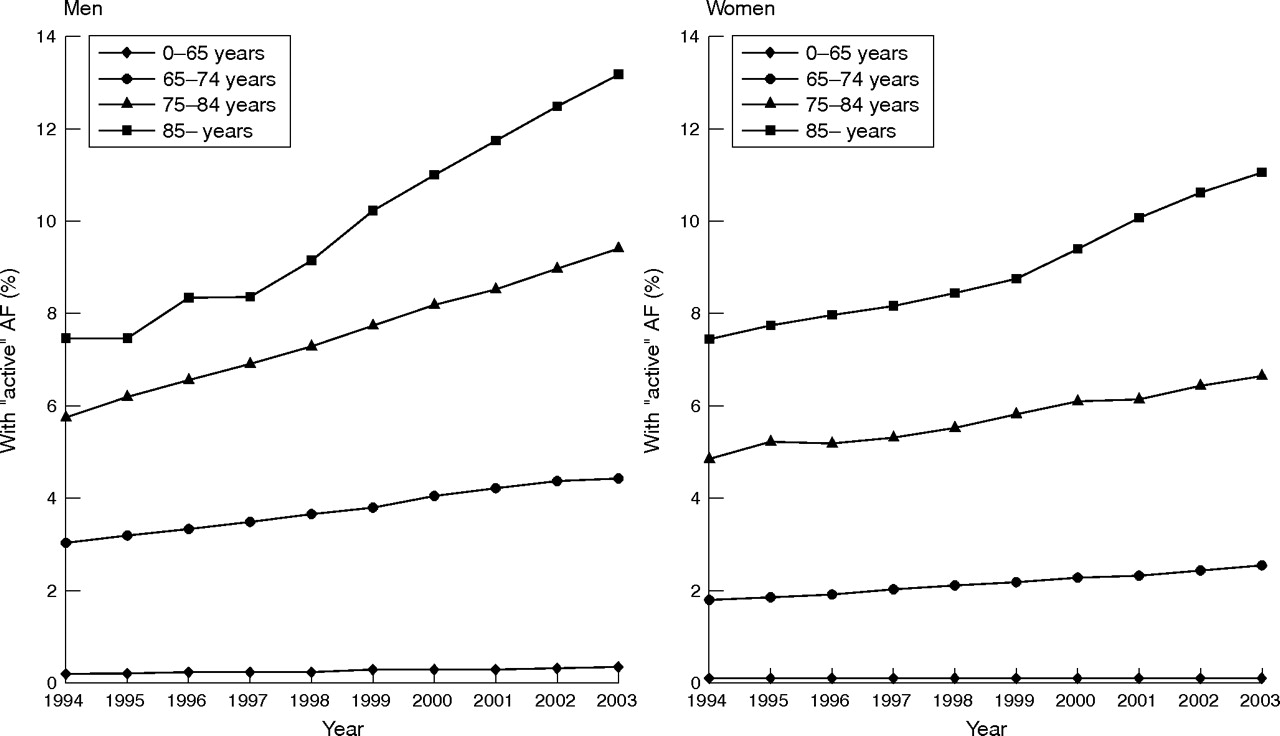
All-ages prevalence of diagnosed AF has risen steadily over time (0.84% in men in 1994 compared with 1.49% in 2003, compared with 0.83% and 1.29%, respectively, in women). The prevalence of active AF rose in a similar fashion (0.78% in men in 1994 compared with 1.31% in 2003, compared with 0.79% and 1.15%, respectively, in women), although the gradually increasing numbers of patients with long term inactive AF means that plots for ever and active AF gradually diverge over time (see web fig 1 on the Heart website—http://www.heartjnl.com/supplemental). The prevalence rose steadily with increasing age. In 2003 the prevalence of active AF in people aged ⩾ 85 was 13.2% in men and 11.0% in women. Figure 1 shows a steady rise in the trend in prevalence of active AF over time in all age groups, most notably in the ⩾ 85 group. Although all trends presented here are not adjusted for age and sex, such adjustment did not have any substantive effect (data not shown).

Trends in active atrial fibrillation (AF) 1994–2003.
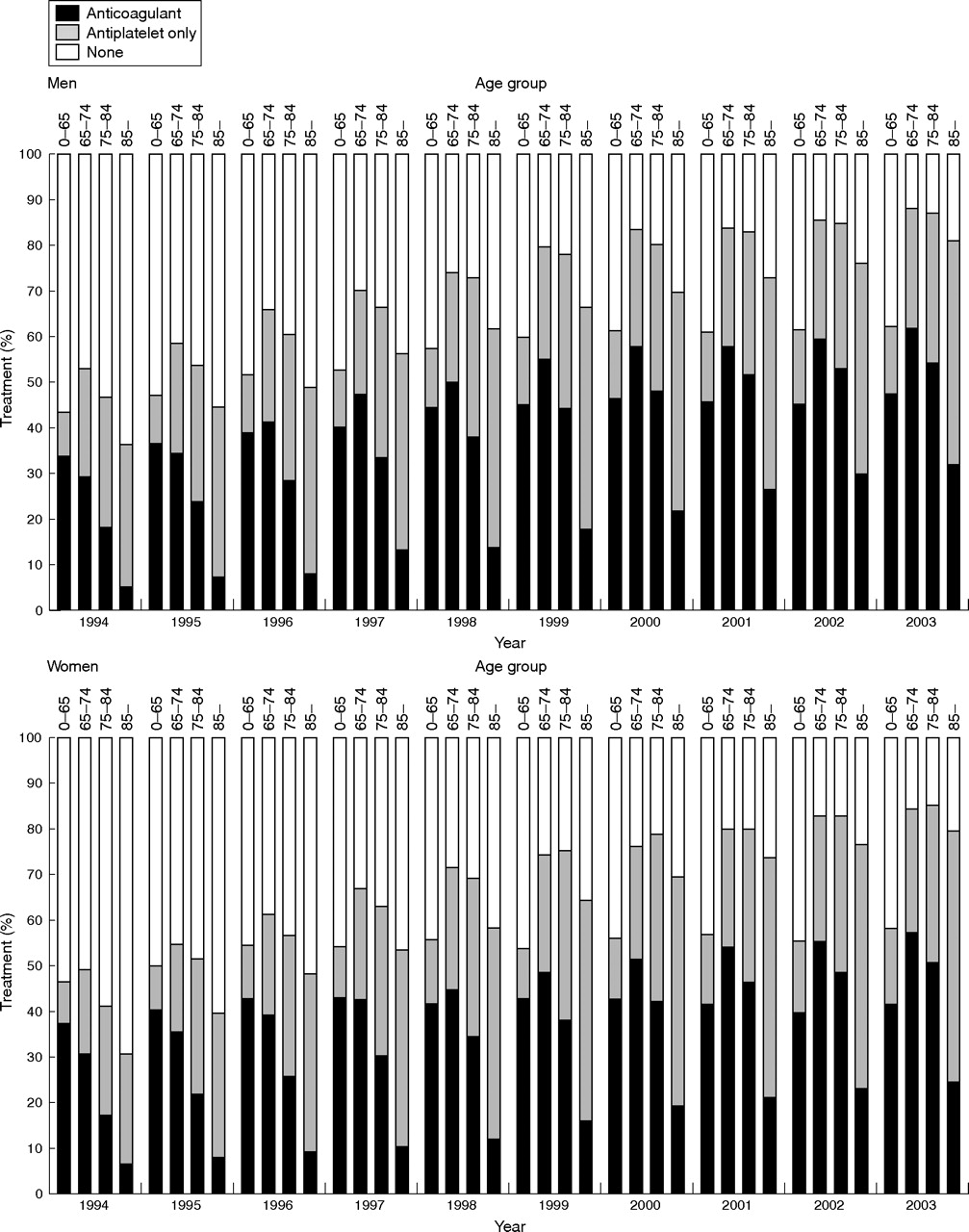
Trends in treatment of active AF
Figure 2 shows trends in treatment to prevent stroke for male and female patients with active AF (for the numbers on which the figure is based see web table 2 on the Heart website—http://www.heartjnl.com/supplemental). Treatment of all types has increased greatly over the study period, with under half of all patients having any treatment in 1994 but around 80% of patients receiving some form of stroke prevention treatment in 2003.
Oral anticoagulant (OA) and antiplatelet treatment by PRODIGY risk score for stroke in patients ⩾35 years old with active atrial fibrillation in 2003
{kind=link}
{kind=link}
Trends in treatment of active atrial fibrillation 1994–2003.
Treatment of AF with oral anticoagulants more than doubled from 1994 to 2003 in men (25% to 53%) and rose similarly but to a smaller extent in women over this time (21% to 40%). The increase is most apparent in older age groups in both sexes, but the ⩾ 85 age group remains by far the least likely to receive warfarin.
Treatment of AF with antiplatelet drugs also increased between 1994 and 2003, although not as rapidly as for oral anticoagulants: treatment with only antiplatelet drugs during any year rose from 23% to 29% in men and 22% to 33% in women.
Factors predicting anticoagulant treatment in patients with AF in 2003
Table 1 summarises the final model predicting anticoagulant treatment in patients who were 35 years or older in 2003. The hierarchical model for region and urban/rural status showed no influence of these factors on the likelihood of anticoagulant prescription (data not shown) The final model, with significant factors from the previous logistic regressions entered in a stepwise fashion, shows major influences of age, sex and PRODIGY risk and smaller, or no, effects for most other factors.
Men were more likely to be prescribed warfarin (odds ratio (OR) 1.26), and extremes of age were associated with a substantially decreased likelihood (OR 0.78 for age 75–84 v 55–64, OR 0.28 for age ⩾ 85 v 55–64). Increasing stroke risk was strongly associated with treatment: patients at very high risk were five times more likely to be treated than those at low risk (OR 5.05, 95% confidence interval 3.97 to 6.42). ACORN score was not significantly associated with treatment likelihood.
Of the potential interacting and contraindicated drugs and conditions that were assessed, 14 remained in the final model. Non-steroidal anti-inflammatory drugs (NSAIDs), antiplatelet drugs and ulcer healing drugs were associated with a reduced likelihood of treatment as were peptic ulcers, chronic gut disorders, anaemias, poor compliance and non-organic psychoses. A range of cardiovascular co-morbidities (ischaemic heart disease, heart failure, arterial disease and other cardiovascular system disorders) and drugs (lipid lowering and antiarrhythmics) were independently associated with an increased likelihood of anticoagulation.
Stroke prophylaxis by PRODIGY risk
Table 2 shows proportions of patients taking no treatment, antiplatelet treatment only, and anticoagulant treatment, by PRODIGY stroke risk in 2003. To investigate whether the patterns of treatment were influenced by the presence of co-morbidities or advanced age, we initially excluded patients with selected co-morbidities (middle section of table 2), and then excluded patients with selected co-morbidities and all who were age ⩾ 85 years (bottom section of table 2).
Of patients at very high risk (having had a previous ischaemic stroke), 7.2% were taking no treatment. Conversely, 38.2% of patients at low risk were taking warfarin. Only 56.5% of patients at very high risk were taking warfarin, although most of the rest were taking antiplatelet drugs. Excluding patients by age or co-morbidities did not greatly alter this pattern, although warfarin was generally used more by patients younger than 85.
All analyses were repeated for patients with AF ever and gave very similar results (data not shown).
DISCUSSION
The prevalence of diagnosed AF in this study is comparable with rates found in other UK primary care studies4,18,19 and emphasises that the previously observed steady rise in the prevalence of diagnosed AF is continuing.4 Our findings do not confirm the Copenhagen heart study findings of a male sex-specific rise in prevalence. Diagnoses were ECG confirmed in the Copenhagen study, however, whereas diagnoses in DIN-LINK were not necessarily ECG confirmed.20 The observed increase may be due to a true increase in prevalence, for which there is some evidence21; to increased ascertainment; or to improved recording of diagnoses. The most probable contributor is an increase in ascertainment due to an increased awareness of the importance of AF. Although increased recording may have contributed, this is unlikely to be the most important explanation, as levels of diagnostic coding were already high in DIN-LINK practices in the earlier years
Trends in stroke prophylaxis in AF
The very pronounced increase in the use of oral anticoagulants by patients with AF confirms and is comparable with the findings of other studies,4 but it also confirms the observation that many patients still do not receive this treatment.19 The increase in treatment of older age groups is as would be predicted from the use of risk-factor scoring systems such as that included in PRODIGY to guide clinicians, as all of these systems include an age element in producing a risk score.
Factors predicting anticoagulant treatment of AF
This study examined predictors of anticoagulant treatment in AF in greater detail than has been previously undertaken.
Sex
A sex difference in prescribing in cardiovascular disease has been observed elsewhere22 and, although some of this difference may be related to differences in age at onset and severity of disease between the sexes,14 in this case a difference persists even after adjustment for age. Given that women with AF appear to lose their protection against sudden death including stroke,23 and may even have a higher mortality than men,24 lower anticoagulant rates are a cause for concern.
Stroke risk score
That high cerebrovascular accident risk is a predictor of warfarin use is unremarkable, but it is noteworthy that 38% of patients categorised as having a low risk were still prescribed anticoagulants, perhaps unnecessarily, whereas only 57% of patients categorised as being at very high risk of a stroke were prescribed these drugs. Confounding by age or co-morbidities does not explain this finding. In the light of this finding, it is unclear whether clinicians actually use decision support tools such as PRODIGY to help manage AF or whether such tools need refining.
Extreme age
The finding that patients older than 85 years were five times less likely to be prescribed warfarin than patients in the 55–64 age group is of note. While ageism appears to be a real problem in some areas of prescribing,14 co-morbidities tend to increase with age, as does the prescribing of drugs that may relatively contraindicate anticoagulant prescription. Some conditions regarded as absolute or relative contraindications to anticoagulants may also develop with age. Before ageism is assumed, the influence of these and other factors, including patient choice, needs to be considered. For example, it is plausible that patients with AF are less likely to agree to anticoagulation treatment with increasing age because of the need for repeated blood tests.
Co-morbidities
Relatively few conditions appeared to be associated with a reduction in the likelihood of anticoagulant prescription. Most were conditions associated with gastrointestinal bleeding, pronounced debility or difficulties with consent or compliance. This is unsurprising.
That a wide range of cardiovascular disorders are associated with an increased likelihood of anticoagulant prescription is likely to be due to the increased contact that these patients have with secondary care doctors, especially cardiologists, who may be more inclined to start anticoagulation than their general practitioner colleagues.
Conditions contraindicating anticoagulants
The numbers of patients with many of the conditions contraindicating anticoagulant drugs were rather small, and few significant effects were noted. Contraindications associated with bleeding or poor compliance were associated with less treatment. The lack of association with mobility problems suggests that independent walking ability is not a major factor in deciding whether to prescribe anticoagulants, contrary to what has been suggested for Italian patients.9
Drug cautions and contraindications to anticoagulants
That NSAIDs and drugs for treatment of peptic ulcers are associated with a reduced chance of anticoagulant prescription is congruent with the other findings of this study. The positive association of antiarrhythmics with anticoagulant prescribing is probably because most of these drugs are started by cardiologists, who may also be more willing to start warfarin. This may also explain the association with lipid lowering drugs. The reason for the influence of uricosuric drugs on prescription of warfarin is not clear.
ACORN score, practice location and degree of urbanisation
This study found no influence of ACORN score or the geographical location or degree of urbanisation of the practice on the likelihood of warfarin prescription. This may reflect a strength of the National Health Service (NHS) in providing care for all parts and groups of the population with a similar condition. Social inequities do not have a major influence on the use of anticoagulants despite their cost and complexity. This is in keeping with previous studies of treatment of hypertension and use of statins in the secondary prevention of coronary heart disease within the NHS.14,25,26
Limitations
Like all studies of this type, it is not possible be certain that all coded cases actually are AF. The validity of diagnoses of many conditions in this and other similar databases, however, has been confirmed by a range of means.12,27 Completeness of coding is more difficult to ascertain, but our findings are comparable with the AF prevalence found in a case-finding study.18 The diagnosis may not be ECG confirmed in all cases, but ECG machines have been widely available in general practice for many years28 and it does not seem unreasonable to assume that the diagnosis is confirmed in most cases. It should also be noted that the algorithm used in this study cannot reliably differentiate between a single episode of self-limiting AF and other forms of AF restored to sinus rhythm by treatment. This may be relevant to other studies of AF treatment but does not substantially affect the validity of our conclusions.
We have examined the influence on likelihood of anticoagulant prescribing of a broader range of factors than previous studies have, but not all factors will be coded in the records. For example, patient preference, which is not coded, can be an important factor for a treatment requiring regular monitoring and dietary restrictions.
Conclusions
This study confirms previously observed rising trends in the prevalence of diagnosed AF and of stroke prophylaxis. Despite such an increase, many patients who possibly would benefit from warfarin treatment do not appear to receive it, whereas many patients at low stroke risk who were taking warfarin may be more safely treated with antiplatelet drugs or nothing. Reasons for this are not clear. Wider use of decision support tools may help, although the degree to which these are actually used is not known. We identified several other factors affecting the decision to initiate warfarin treatment. Reduced likelihood of warfarin prescribing is related to drugs or conditions that predispose to bleeding. Conversely, cardiovascular conditions or treatments were associated with a greater likelihood of warfarin prescription, suggesting that being seen in secondary care may have an important influence. The lower likelihood of women receiving anticoagulants is of particular concern.
Given the considerable variations in treatment of seemingly similar patients and the potentially serious consequences of over-treatment or under-treatment, further studies surveying doctors’ reasons for prescribing or not prescribing warfarin in specific cases may be of value in understanding what other factors are important here. The factors that influence whether patients are willing to be treated with warfarin also need to be considered.
Acknowledgments
We acknowledge the technical assistance of Mr Steve Caine of CompuFile Ltd in handling the data and the general practitioners who provided the data.
REFERENCES
Supplementary materials
Footnotes
-
Published Online First 30 December 2005
-
This study was funded by a grant from AstraZeneca. IC was also funded by a grant from the Wellcome Trust. SDeW was funded by the BUPA foundation.
-
Competing interests: AstraZeneca funded this study and have interests in stroke prophylaxis. NR is a director of a company providing DIN-LINK data for commercial purposes.