Article Text

Abstract
Objectives: To investigate whether the ratio of early transmitral flow velocity (E) to early diastolic mitral annular velocity (E′) predict prognosis in patients with non-valvular atrial fibrillation.
Methods: 230 patients with non-valvular atrial fibrillation were enrolled and studied. According to E/E′ value, patients were divided into groups with lower (group A with E/E′ ⩽ 15) and higher (group B with E/E′ > 15) E/E′.
Results: During follow up (average 245 days), 21 (9.1%) deaths were documented. All cause death (15/90 (16.7%) v 6/140 (4.3%)), cardiac death (10 (11.1%) v 2 (1.4%)) and congestive heart failure (16 (17.8%) v 8 (5.7%)) were more common in group B than in group A (all p < 0.01). A Kaplan–Meier survival curve showed that the cumulative survival rate was significantly lower in group B than in group A (log rank p = 0.0013). By multivariate logistic regression analysis, E/E′ (χ2 = 4.47, odds ratio (OR) 1.05, 95% confidence interval (CI) 1.01 to 1.11, p = 0.03) and age (χ2 = 6.45, OR 1.06, 95% CI 1.01 to 1.11, p = 0.02) were independent predictors of mortality.
Conclusion: The Doppler-derived index of left ventricular filling pressure, E/E′, is a powerful predictor of the clinical outcome of patients with non-valvular atrial fibrillation.
- E, early transmitral filling velocity
- E′, early diastolic mitral annular velocity
- EF, ejection fraction
- LV-DT, deceleration time of early transmitral flow velocity
- PV-DT, deceleration time of diastolic peak pulmonary venous flow velocity
Statistics from Altmetric.com
- E, early transmitral filling velocity
- E′, early diastolic mitral annular velocity
- EF, ejection fraction
- LV-DT, deceleration time of early transmitral flow velocity
- PV-DT, deceleration time of diastolic peak pulmonary venous flow velocity
Congestive heart failure with or without left ventricular systolic dysfunction is a common cause of death and morbidity in patients with heart diseases. About a third of patients with congestive heart failure have normal left ventricular systolic function.1 Abnormal left ventricular diastolic function has been recognised as a possible cause of congestive heart failure in patients with normal ejection fraction (EF).2 Pulsed Doppler-derived transmitral flow velocity and pulmonary flow have been used as non-invasive measures in assessing left ventricular diastolic function, providing haemodynamic as well as prognostic information about patients with sinus rhythm.3–6
Atrial fibrillation is commonly associated with congestive heart failure, especially in the elderly population.7,8 In addition, the presence of atrial fibrillation is a poor prognostic indicator in patients with congestive heart failure. Doppler echocardiographic methods including measurement of transmitral flow velocity and pulmonary flow velocity have been proposed to evaluate pulmonary capillary wedge pressure and left ventricular diastolic function.9–12
Recently, the ratio of the early transmitral filling velocity (E) to early diastolic mitral annular velocity (E′) has been proposed as a novel index to assess left ventricular filling pressure.13–18 Although E′ and E/E′ have been shown to predict the prognosis of patients with various heart diseases,19–21 its prognostic significance for patients with atrial fibrillation is unknown.
Accordingly, we hypothesised that E/E′ would predict survival of patients with non-valvular atrial fibrillation. We therefore conducted this study to evaluate the usefulness of the tissue Doppler imaging-derived index E/E′ to predict the clinical outcome of patients with non-valvular atrial fibrillation.
METHODS
Study population
Between January 2000 and December 2004, the Bell Land General Hospital echocardiography database was searched to find patients with non-valvular atrial fibrillation who were referred for echocardiographic examination and had both transmitral flow velocity analysis and tissue Doppler imaging of the mitral annulus. A total of 230 consecutive patients with non-valvular atrial fibrillation were identified. Non-valvular atrial fibrillation was defined as atrial fibrillation without rheumatic valvular heart disease or significant (greater than moderate) aortic or mitral valve disease (stenosis or regurgitation) other than of rheumatic origin. We identified 128 men and 102 women with a mean age of 72 (SD 11) years.
Conventional echocardiographic examination
With patients in the left lateral decubitus position, conventional transthoracic two-dimensional and Doppler echocardiography was performed with a commercially available echocardiographic machine (Vivid 7; GE Healthcare Technologies, Waukesha, Wisconsin, USA) with a broadband (1.5–4 MHz) phased array transducer. From the parasternal long axis view, left atrial dimension was measured as reported previously. Left ventricular end diastolic volume, end systolic volume and EF were measured and calculated on the basis of the modified Simpson’s rule from the apical two- and four-chamber views.22 Left ventricular mass was calculated as reported previously.23 Transmitral flow velocity signals were recorded from the apical four-chamber view and E was measured. Deceleration time of early transmitral flow velocity (LV-DT) was also measured. Similarly, pulmonary venous flow velocity signals were recorded from the apical four-chamber view. Systolic and diastolic peak velocities were measured. The ratio of systolic to diastolic peak velocity was calculated. Deceleration time of the diastolic peak pulmonary venous flow velocity (PV-DT) was also measured.
Tissue Doppler imaging measurements
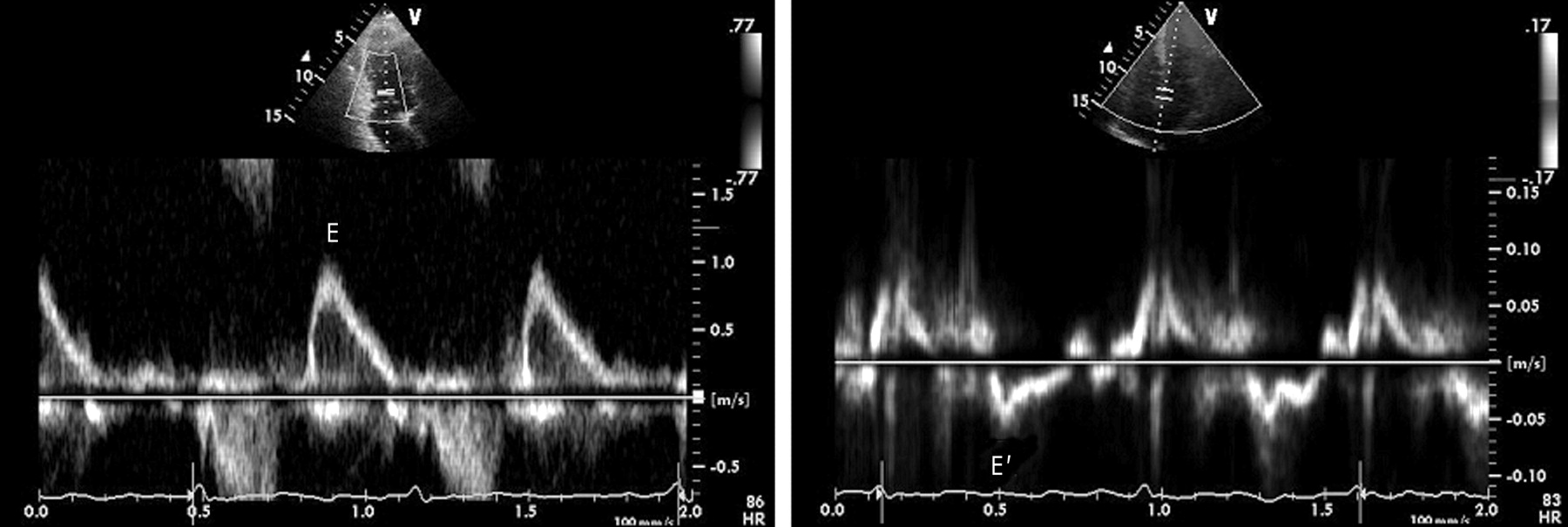
The apical four-chamber view was used to obtain tissue Doppler imaging of the mitral annulus. A sample volume of the pulsed wave Doppler was positioned at the septal side of the mitral annulus and then the spectral signal of the mitral annular velocity was recorded. Peak E′ was measured.16,20 As an index of left ventricular filling pressure, E/E′ was calculated (fig 1). The average of five consecutive Doppler signals was used.24 Mean intraobserver and interobserver variabilities were 4.6 (SD 3.9)% and 9.2 (10.0)% for E, 4.2 (3.3)% and 7.2 (6.2)% for E′, and 5.0 (3.3)% and 11.4 (14.8)% for E/E′, respectively.

Tissue Doppler imaging and transmitral flow velocity signals. E, early transmitral flow velocity; E′, early diastolic mitral annular velocity.
Patients were divided into two groups based on the E/E′ value, group A (E/E′ ⩽ 15, n = 140) and group B (E/E′ > 15, n = 90).
Clinical outcome
Patients’ death and cause of death were identified by a medical record review or telephone contact. Cardiac death was defined as either a death directly related to cardiac disease, mainly congestive heart failure, or sudden death. Similarly, a history of congestive heart failure during follow up was identified by a medical record review or telephone contact.
Statistical analysis
Continuous data are expressed as mean (SD). Differences in parametrical data between the two groups were tested by the unpaired t test. Categorical variables between the groups were compared by χ2 test or Fisher’s exact test. Independent predictors of death were calculated by logistic regression. The following parameters were evaluated first in a univariate model: age, sex, hypertension, hyperlipidaemia, diabetes mellitus, history of myocardial infarction, history of stroke, history of congestive heart failure, left atrial dimension, end diastolic volume, end systolic volume, EF, E, E′, E/E′, LV-DT, peak systolic velocity, diastolic peak velocity of the pulmonary venous flow velocity, the systolic to diastolic ratio, and PV-DT. Variables with a probability value of < 0.15 were then entered into a multivariate logistic regression analysis. Cumulative survival curves during follow up of patients with lower versus higher E/E′ were obtained by the Kaplan–Meier method with a log rank test. A value of p < 0.05 was considered significant. Data were statistically analysed with commercially available software (StatView, SAS Institute, Cary, North Carolina, USA).
RESULTS
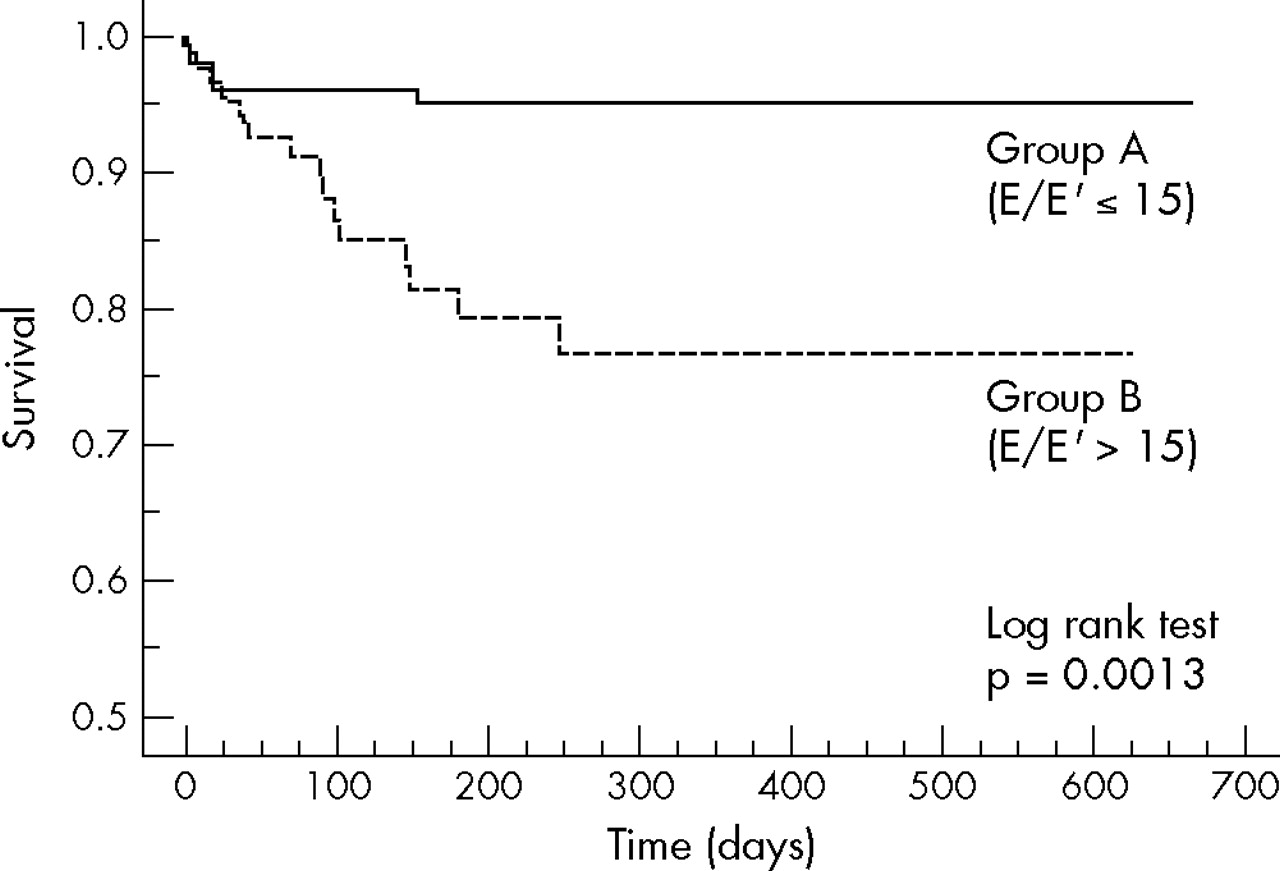
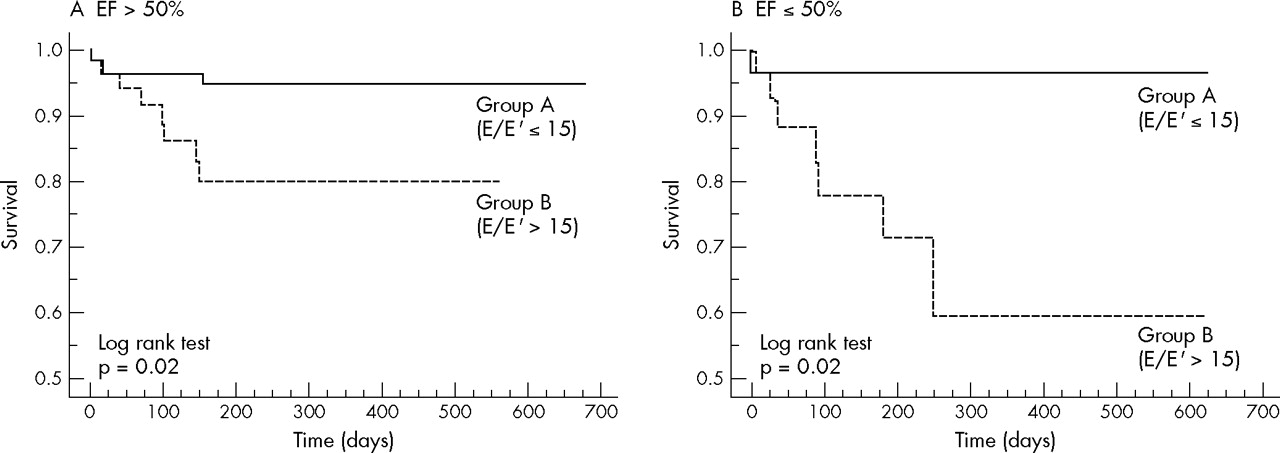
During the follow-up period (average 245 (200) days), 21 deaths (9.1%) were documented: 12 cardiac deaths and 9 non-cardiac deaths. Table 1 shows baseline clinical characteristics of each group. Group B consisted of significantly older patients and more men than in group A. In addition, the incidence of prior myocardial infarction was higher in group B. Table 2 shows two-dimensional and Doppler echocardiographic indices. Compared with group A, group B had larger left atrial dimension, end diastolic volume, end systolic volume and left ventricular mass; higher peak diastolic velocity of the pulmonary venous flow velocity and a higher incidence of mitral regurgitation (less than moderate); and lower EF. Although Doppler-derived E was significantly higher and E′ was lower in group B than in group A, LV-DT and PV-DT did not differ between the groups. Table 3 summarises clinical event rates in each group. Congestive heart failure was more common in group B than in group A. All cause mortality and cardiac death were significantly higher in group B than in group A. On the other hand, non-cardiac death was not different between the two groups. The composite of death and congestive heart failure was significantly higher in group B than in group A. Kaplan–Meier analysis showed that the survival rate during follow up was significantly higher in group A than in group B (log rank p = 0.0013) (fig 2). To investigate the possible impact of left ventricular systolic function, patients were divided into two groups: with preserved left ventricular systolic function (EF > 50%) and with depressed left ventricular systolic function (EF ⩽ 50%). In both groups, the survival rate was significantly higher in patients from group A than in group B patients, as shown by a Kaplan–Meier plot (fig 3).
Baseline clinical characteristics
Two-dimensional and Doppler echocardiographic indices
Clinical events during follow up

Kaplan–Meier plot of survival rate during follow up in group A (ratio of early transmitral flow velocity (E) to early diastolic mitral annular velocity (E′) ⩽15) and group B (E/E′ >15).

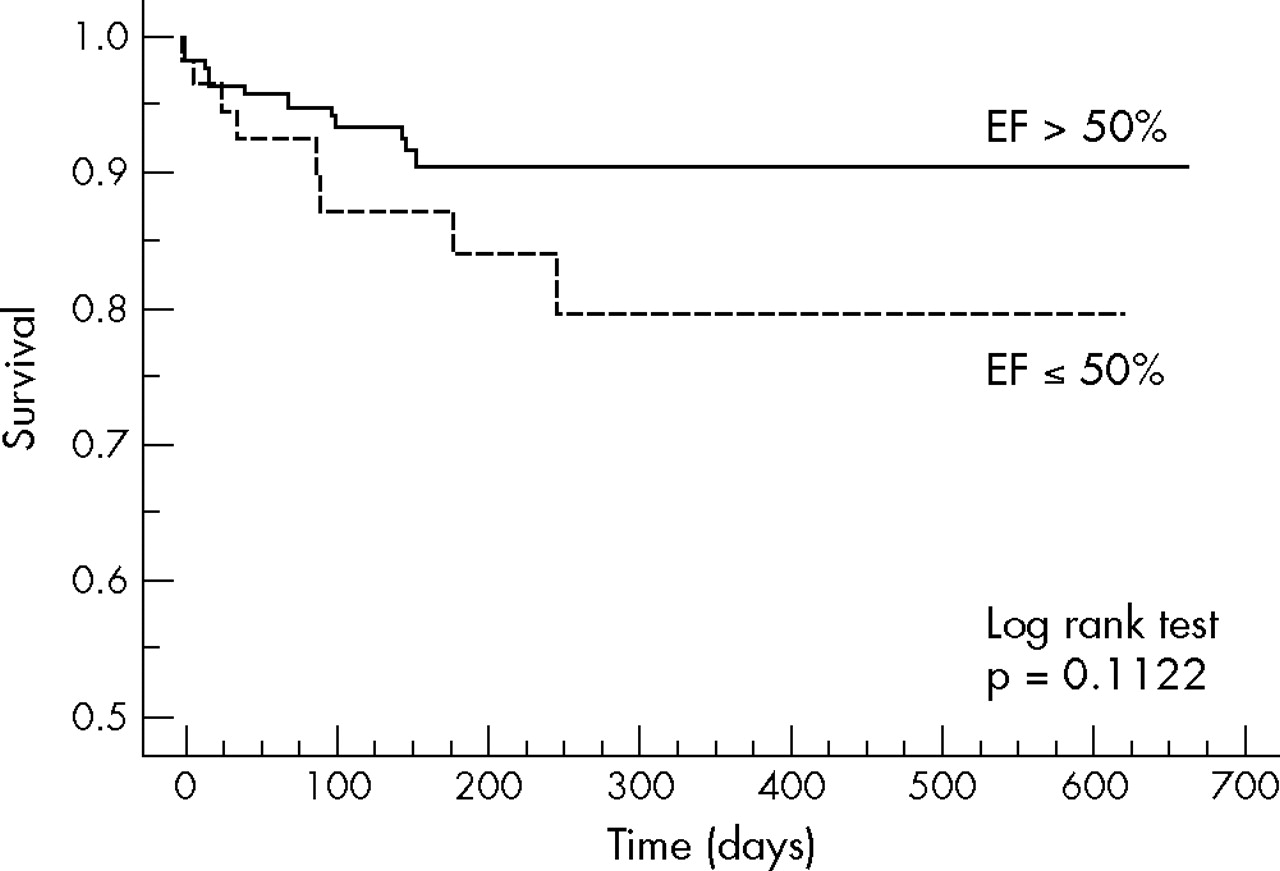
Kaplan–Meier plot of survival rate during follow up in patients with (A) ejection fraction (EF) > 50% and (B) EF ⩽50%. Group A had a significantly higher survival rate during follow up.
Univariate predictors (p < 0.1) of death during follow up were E/E′ (p = 0.004), age (p = 0.005) and hyperlipidaemia (p = 0.03) (table 4). By multivariate logistic regression analysis, independent predictors of death were higher age (χ2 = 6.45, odds ratio (OR) 1.06, 95% confidence interval (CI) 1.01 to 1.11, p = 0.02) and higher E/E′ (χ2 = 4.47, OR 1.05, 95% CI 1.01 to 1.11, p = 0.03). Figures 4 and 5 show Kaplan–Meier analysis according to LV-DT or EF. The cumulative survival rate was similar for patients with LV-DT > 140 ms and ⩽ 140 ms (fig 4). On the other hand, cumulative survival rate tended to be higher in patients with EF > 50% than in patients with EF ⩽ 50%, although it did not reach significance (fig 5).
Clinical and echocardiographic predictors of death during follow up

Kaplan–Meier plot of survival rate by deceleration time of early transmitral flow velocity (LV-DT).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier plot of survival rate by ejection fraction (EF).
DISCUSSION
Our study shows that the tissue Doppler imaging-derived index E/E′ is useful to predict the prognosis of patients with non-valvular atrial fibrillation.
Non-invasive evaluation of diastolic function by Doppler echocardiographic technique has been widely used in daily clinical settings.3–5,25,26 Previous Doppler echocardiographic studies have shown that a restrictive diastolic filling pattern or short deceleration time is a poor prognostic indicator in patients with systolic dysfunction.3–5 Deceleration time is also measured to estimate pulmonary artery wedge pressure in patients with atrial fibrillation.9,11
Recently, an alternative Doppler method to assess left ventricular filling pressure, namely tissue Doppler imaging, has been proposed and tested.13–16 The tissue Doppler imaging-derived index of left ventricular filling, E/E′, has been shown to be useful to assess the left ventricular filling pressure.13–15 Nagueh et al14 showed that E/Ew (equivalent to E/E′) correlated well with pulmonary capillary wedge pressure. Similarly, Ommen et al16 compared E/E′ with the directly measured left ventricular filling pressure and reported that E/E′ > 15 indicates a raised left ventricular filling pressure. In addition, E/E′ was shown to correlate with left ventricular filling pressure in patients with non-rheumatic atrial fibrillation.17
Recent studies have addressed the prognostic implication of E′ or E/E′ in patients with various cardiac diseases.18–21,27 Hillis et al20 reported that E/E′ is a strong predictor of mortality in patients after acute myocardial infarction. They showed that E/E′ > 15 predict poor outcome in patients with acute myocardial infarction. Wang et al19,27 reported that E′ was a strong predictor of cardiac mortality in patients with various cardiac diseases. More recently, McMahon and colleagues21 showed that E/E′ predicts adverse clinical outcome in children with hypertrophic cardiomyopathy. Our present study showed, for the first time, that E/E′ is the strongest independent echocardiographic prognostic predictor in patients with non-valvular atrial fibrillation. Interestingly, LV-DT, which has been known as a strong predictor of mortality in patients with systolic dysfunction, did not predict mortality in patients with non-valvular atrial fibrillation in our present study. Previous echocardiographic Doppler studies have shown that LV-DT predicted mortality in patients with sinus rhythm3–5 as well as with atrial fibrillation.10 Hurrell et al10 reported that in 74 patients with atrial fibrillation and poor left ventricular function (mean EF 39%), restrictive physiology (short LV-DT) predicted poor prognosis. The difference between their series and our present study may in part be explained by the difference in our study populations. In our study, > 70% of the patients had normal systolic function (EF > 50%) and mean EF was 56%. Indeed, when we restricted the analysis to patients with decreased left ventricular systolic function (EF < 50%), the Kaplan–Meier cumulative survival curve showed a higher survival rate among patients with LV-DT > 140 ms than among those with LV-DT ⩽ 140 ms.
The incidence of atrial fibrillation increases with age. Among the population aged > 65 years, about 10% have atrial fibrillation. Non-valvular atrial fibrillation is an important clinical condition not only because of its strong relationship with ischaemic stroke but also as a cause of congestive heart failure and subsequent cardiac mortality and morbidity. Our results may have implications for the risk stratification of this patient population.
Study limitations
There are several limitations in this study. Firstly, we did not measure E and E′ simultaneously. Beat-to-beat variation of the Doppler-derived indices may affect the calculation of E/E′ of patients with atrial fibrillation. Also, the Doppler value may change as left ventricular filling pressure changes. The relationship between serial changes in the E/E′ value and prognosis needs further investigation. Secondly, this was a relatively small, single-centre, retrospective study. These results therefore need to be confirmed by a larger, prospective, multicentre study. Indeed, the lack of an association between LV-DT or PV-DT and prognosis may result from a possible selection bias towards patients with relatively better left ventricular systolic function; thus, our results may need further investigation in a large series including patients with poor left ventricular systolic function. Lastly, the effect of drugs or haemodynamic alteration on E/E′ and, as a result, prognosis has not been investigated.
In conclusion, the Doppler echocardiography and tissue Doppler imaging-derived index of left ventricular filling, E/E′, is a strong predictor of cardiac mortality in patients with non-valvular atrial fibrillation.
REFERENCES
Footnotes
-
Published Online First 31 January 2006