Article Text

Abstract
Background: Atrial fibrillation (AF) and heart failure (HF) often coexist. The aim was to investigate whether restoring sinus rhythm (SR) could improve cardiac function, symptoms, exercise capacity and quality of life (QoL) in patients with chronic heart failure.
Methods: Patients with HF and persistent AF receiving guideline-recommended treatments, including anticoagulants, were eligible for the study. Patients were randomised to either rhythm (treated with amiodarone for at least 3 months prior to attempting biphasic external cardioversion and continued amiodarone long-term if SR was restored) or rate control. Anticoagulants were continued throughout the study regardless of rhythm, unless contraindications developed. Both groups were treated with beta blockers and/or digoxin to reduce the heart rate to <80 bpm at rest and <110 bpm after walking. Symptoms, walk distance (6-minute corridor walk test, 6MWT), QoL and cardiac function were assessed at baseline and 1 year.
Results: 61 patients with HF and persistent AF (median duration 14 months (IQR 5 to 32)) were randomly assigned to a rate or rhythm control strategy. Of patients assigned to rhythm control (n = 30), 66% were in SR at 1 year, and 90% of those assigned to rate control (n = 31) achieved the heart rate target. At 1 year, NYHA class (p = 0.424) and 6MWT distance (p = 0.342) were similar between groups but patients assigned to rhythm control had improved LV function (p = 0.014), NT-proBNP concentration (p = 0.046) and QoL (p = 0.019) compared with those assigned to rate control. Greatest improvement was seen in patients in whom SR was maintained.
Conclusion: Restoring SR in patients with AF and heart failure may improve QoL and LV function when compared with a strategy of rate control.
Statistics from Altmetric.com
Atrial fibrillation (AF) and heart failure are both common and often coexist. Patients with AF who develop heart failure have more symptoms, a worse quality of life and a poorer prognosis, and the same is true for patients with heart failure who develop AF.1–3
The best way to manage AF in the presence of heart failure is uncertain. Several large trials comparing rate with rhythm control for the management of AF have been reported, (AFFIRM, PIAF, STAF, RACE, HOT-CAFÉ),4–8 providing little evidence of the superiority of one strategy over another. However, these studies were largely conducted on patients without heart failure and included those with paroxysmal AF. Theoretically, patients with heart failure may benefit more from restoration of SR than their non-heart-failure counterparts. Several observational and non-randomised studies have reported that restoring and maintaining sinus rhythm in patients with heart failure improved LV function, exercise performance and QoL, and reduced mortality.9–14 Retrospective subgroup analysis of (1) the AFFIRM study, suggested survival benefit for those with impaired LV function who maintained SR,15 and (2) the RACE study reported that rhythm control improved LV function and reduced atrial size, hospitalisation and mortality.16 17 However, the recent prospective randomised Atrial Fibrillation in Congestive Heart Failure (AF-CHF) study18 failed to show an effect on mortality in patients assigned to rhythm control compared with rate control. Nonetheless, a management strategy that improves symptoms and/or QoL for patients with heart failure without harming them would be highly desirable.
Concurrent with the latter trial, we conducted a randomised controlled study to determine whether restoration and maintenance of sinus rhythm were of benefit to patients with heart failure and persistent AF.
METHODS
Study population
An overview of the study design is shown in fig 1. Potential study patients were identified among referrals to the hospital’s heart failure clinic. Patients aged ⩾18 years of age with persistent AF and chronic symptomatic heart failure (ie, NYHA ⩾ Class II symptoms) with evidence of systolic dysfunction on echocardiography were eligible for enrolment. Patients in whom oral anticoagulants were contraindicated were excluded. Persistent AF was defined according to joint European Society of Cardiology (ESC), American Heart Association (AHA) and American College of Cardiology (ACC) guidelines.19 Heart failure therapy was optimised (including dose titration) in all patients during follow-up.

Overview of rate versus rhythm control study. At 1 year, adequate rate control was achieved in 90% of patients and sinus rhythm maintained in 66% patients in rate control and rhythm control groups respectively. AF, atrial fibrillation; HF, heart failure.
The study was approved by the Hull & East Yorkshire Ethics Committee, and all patients gave written informed consent. Patients were randomly allocated (block randomisation with variable block-size) to either a rate control or rhythm control strategy.
A standard medical history, including current therapy, was taken. Patients were examined and had a 12-lead electrocardiogram, two-dimensional echocardiography and blood taken for standard haematology, biochemistry profiles and NT-pro-BNP (Elecsys, Roche, Indianapolis, Indiana). A 6-minute walk test (6-MWT) was performed and quality of life (QoL) assessed.
Patients were reviewed at 4-monthly intervals following randomisation. At each visit, cardiovascular events were recorded, a 12-lead electrocardiogram was obtained, and rate control at rest and during a corridor walk test performed. At 1 year, blood was taken for NT-proBNP, haematological and biochemical analysis, and patients had a repeat transthoracic echocardiogram. Patients were encouraged to report new or worsening symptoms between visits. Ambulatory recording was used where symptoms suggested intermittent AF recurrence but was not used routinely.
Quality of life
Quality of Life (QoL) was assessed by asking patients to complete a generic and a disease specific questionnaire, the Medical Outcomes Study Short Form-36 (SF-36) version II questionnaire and the Minnesota Living with Heart failure (MLWHF) questionnaire respectively.
The Medical Outcomes Study Short Form-36 version II (SF-36vII) questionnaire is a widely used and validated measure of health status. Using specified algorithms, scores on these subscales were transformed to create the Physical and Mental Component Summary scores, which could range from 0 to 100, with higher scores indicating better perceived health status. The MLWHF is specifically designed to measure the effects of heart failure and its treatment on an individual’s QoL. Overall scores range from 0 to 105, with higher scores representing a poorer quality of life (unlike SF36vII).
The reliability estimates using the Cronbach α for the study population were 0.81, 0.77 and 0.83 for SF36vII Physical functioning, SF36vII Mental functioning and MLWHF respectively.
Study patients and investigators were unaware of QoL questionnaire scores throughout follow-up.
Echocardiography
Echocardiography was performed in all patients at baseline and at 1 year. Measurements were taken in accordance with American Echocardiography Society/European Association of Echocardiography guidelines. Due to the inherent difficulties of accurately measuring LV ejection fraction in AF, LV systolic function was assessed in all subjects by estimation on a six-point scale of normal, mild, mild to moderate, moderate, moderate to severe and severe impairment.
Rate control strategy
Digoxin and β-blockers were used to achieve rate control.20 Adequate rate control was defined as a resting ventricular rate of <80 bpm and a rate of <110 bpm at the end of the 6-MWT.
Rhythm control strategy
Patients assigned to the rhythm control group started oral amiodarone therapy (200 mg three times a day for 1 month, followed by 200 mg twice a day for 1 month and 200 mg daily thereafter). If AF persisted, despite at least 2 months of treatment, “day-case” external biphasic electrical cardioversion under general anaesthesia was performed using an energy regime of 150 J, followed by 150 J if initially unsuccessful, then 200 J if necessary. Thereafter, patients continued to receive amiodarone therapy in addition to their usual medication. If cardioversion was unsuccessful or AF recurred, further attempts at electrical cardioversion were offered. If attempts at restoring sinus rhythm were abandoned, then amiodarone was stopped, and a rate-control strategy was followed.
Regardless of study arm allocation or cardiac rhythm, all patients were anticoagulated using warfarin, aiming for an International Normalised Ratio (INR) of 2.0 to 3.0 throughout the study.
Statistical analysis
The primary outcome was QoL using SF-36vII at 1 year. Secondary outcomes were proportion in SR, MLWHF, NT-proBNP, 6-minute corridor walk test (6MWT) and severity of LV systolic dysfunction in hierarchical order.
Discrete variables are expressed as frequency counts and percentages; continuous variables are expressed as mean (SD) if normally distributed, otherwise median (interquartile range, IQR). Variable distribution was assessed using the one-sample Kolmogorov–Smirnov test. Comparisons of NT-proBNP were made using log-transformed values to reduce the effects of skewness within the distribution.
All analyses were based on the intention-to-treat principle. Differences between groups at baseline were not examined in line with good statistical practice for randomised controlled trials.21 Differences at 1 year compared with baseline were established by the paired samples t test or χ2 test where appropriate. A nominal level of 5% significance was assumed (two-tailed). The differences between rate and rhythm control groups with respect to change in variable from baseline to 1 year were compared using ANOVA or the Kruskal–Wallis test according to variable distribution. The numbers of patients completing the study at 1 year were 30 and 29 in the rate and rhythm control groups respectively. This allowed us to detect a medium to large effect size (ie, 0.6 to 1.0 SDs of the primary outcome measure) with 80% power and 5% significance (two-tailed).
Analysis was performed using SPSS (Chicago) for Windows, version 14.0.2 statistical software.
RESULTS
Patient characteristics
Sixty-one patients were recruited, with 31 randomly assigned to a strategy of rate control and 30 to rhythm control. Baseline characteristics are shown in table 1. Most patients were already receiving beta-blockers (80%), ACE inhibitors (89%) and loop diuretics (90%) at the baseline assessment. The median duration of AF was 14 months (IQR 6 to 32), and 20% of patients had undergone a previous external cardioversion. Patients were well matched with respect to symptom severity, QoL, 6MWT, severity of LV dysfunction and NT-proBNP.
No patient was lost to follow-up. There were two deaths during the first year’s follow-up, one in the rate control group (of cardiovascular cause) and one in the rhythm control group (non-cardiovascular cause). Warfarin was discontinued in one patient (rate control group) due to recurrent epistaxis. One patient in the rate control group underwent elective pacemaker insertion because of bradycardia.
Rate control
Of patients assigned to rate control, 61% already fulfilled target ventricular rate control at rest and following exercise at baseline assessment. The mean ventricular rate was 73 (SD 15) bpm at rest and 100 (22) bpm following exercise. Digoxin and beta-blocker use at baseline was 65% and 84% respectively. At 1 year, target ventricular rate control was achieved in 90% of patients. Digoxin and beta-blocker use at 1 year was 84% and 90% respectively. The mean ventricular rate was lower at rest and following exercise; 70 (9) bpm at rest (p = 0.002 versus baseline) and 87 (12) bpm (p = 0.015 versus baseline) after exercise. All patients in the rate control group were in AF at each and every follow-up visit.
Rhythm control
Amiodarone was started in all rhythm control patients at baseline, and 24 (80%) patients were still taking it at 1 year. Beta blocker use at baseline and 1 year was 83% and 93% respectively. Sinus rhythm was restored in six (20%) patients using amiodarone alone. One patient declined electrical cardioversion and remained in AF throughout the study. Cardioversion restored SR in 18 of the 23 (78%) patients in whom it was attempted. The mean energy levels were 170 (25) J. A second cardioversion was performed in four patients for AF recurrence following an initially successful cardioversion. Overall, 26 (87%) patients were converted from AF to SR at some time during the study. The median time to first electrical cardioversion was 4 months (IQR 3 to 6 months).
The prevalence of AF in the rhythm control group was 53% at 4 months, 30% at 8 months and 34% at 1 year (see fig 2). At 1 year, a rate control strategy had been adopted in six patients (20%) as a result of accepting permanent AF and discontinuing amiodarone.

Percentage of patients in sinus rhythm during follow-up within the rhythm control group.
Quality of life (QoL) and symptoms
Patients assigned to rhythm control had a greater improvement in QoL over 1 year compared with rate control when assessed using SF36vII (p = 0.020 for SF36vII as a whole; p = 0.050 for mental functioning and p = 0.029 for physical functioning subgroups). The difference in QoL using the MLWHF questionnaire was not statistically significant (p = 0.140; see fig 3). In a post hoc exploratory analysis, we compared only those patients in sinus rhythm at 1 year (within the rhythm group) with those with adequately rate controlled AF (in the rate control group), and found an improvement in QoL using both MLWHF (p = 0.040) and SF36vII (p = 0.022; see fig 4).

Comparison of change in quality of life (QoL) scores over 1 year between rate and rhythm control groups. The p values denote the comparison between groups. Bars represent mean QoL score and whiskers represent the standard error of the mean. *Inverse Minnesota Living with Heart failure (MLWHF) score; unlike SF-36 vII, a lower MLWHF score indicates a better QoL.
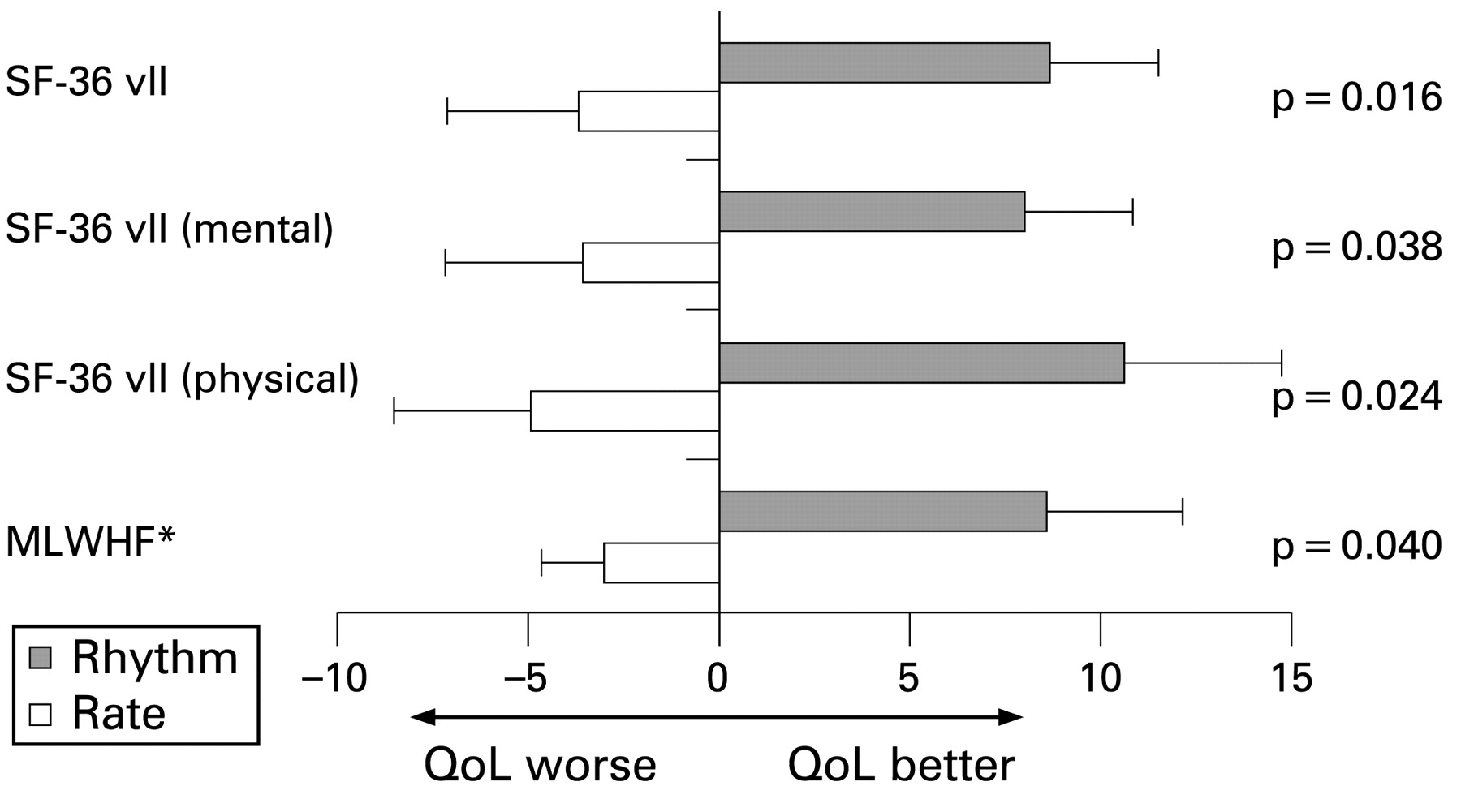
Comparison of change in quality of life (QoL) scores over 1 year between rate and rhythm control groups (comparing only those who maintained SR in the rhythm control group with those achieving adequate rate control in rate control group). Bars represent mean QoL score, and whiskers represent the standard error of the mean. *Inverse Minnesota Living with Heart failure (MLWHF) score; unlike SF-36 vII, a lower MLWHF score indicates a better QoL.
NYHA class was similar at baseline and 1 year in each group with no differences observed between strategies (p = 0.424). Similarly, no difference in NYHA class was seen when comparing only those who were in SR at 1 year (within rhythm control group, p = 0.582) or only those with adequate rate control (within rate control group, p = 0.492).
Exercise performance (6MWT)
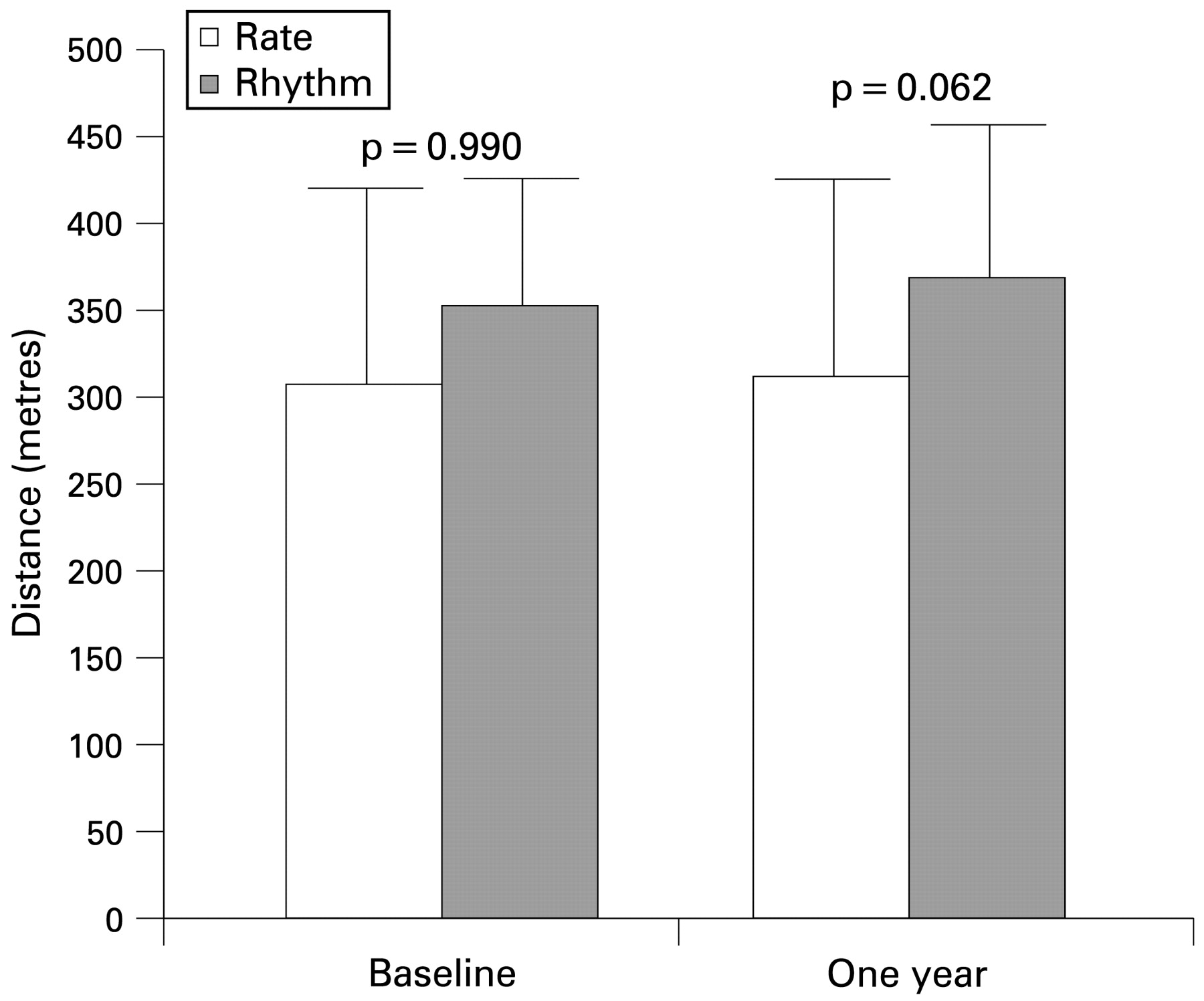
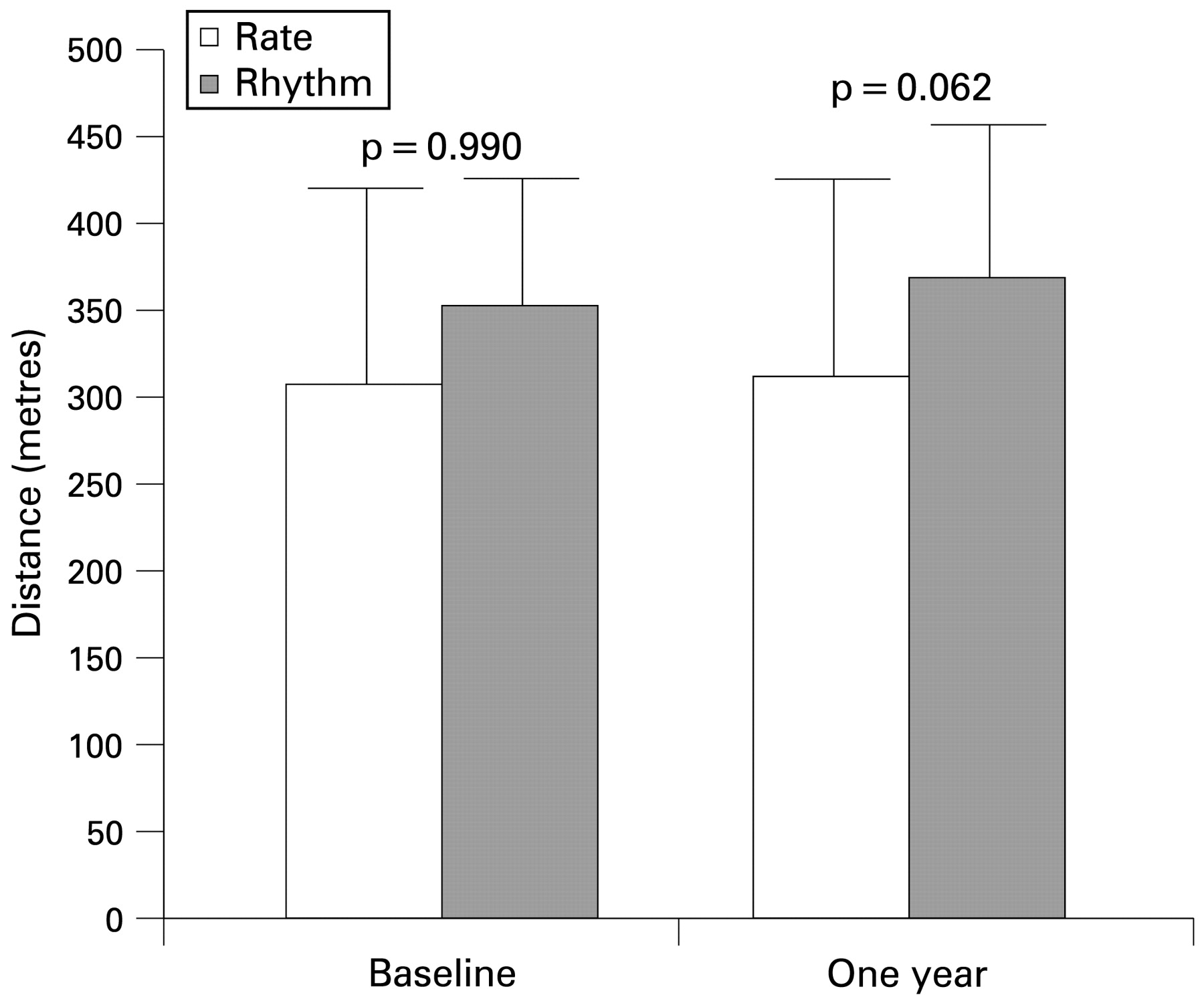
Distance walked at baseline was 307 (118) m and 352 (80) m for rate and rhythm control groups respectively (p = 0.108), compared with 311 (122) m and 368 (76) m at 1 year. The mean change at 1 year was −7 (41) m and +5 (58) m for rate and rhythm control respectively (p = 0.342; see fig 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Six-minute walk test distance at baseline and 1 year. There was no difference between groups at baseline or 1 year.
When comparing only those patients with adequate rate control at 1 year with those in sinus rhythm, the mean change in 6MWT distance was −10 (42) m and +21 (51) m for rate and rhythm control respectively (p = 0.048).
Left ventricular function
LV function was assessed qualitatively and analysed as such. Baseline median left ventricular function was “moderately” impaired for both groups (p = 0.755). Patients assigned to rhythm control had a greater improvement in LV function over 1 year compared with patients assigned to rate control (p = 0.014). The median severity of LV systolic dysfunction at 1 year in those assigned to rhythm control was “mild” but remained “moderate” in those assigned to rate control.
Natriuretic peptides
NT-proBNP concentrations were similar at baseline (1835 (947 to 2546) pg/ml and 1285 (913 to 1624) pg/ml for rate and rhythm groups respectively, p = 0.102). The median NT-proBNP concentrations at 1 year were 1480 (1074 to 2681) pg/ml and 685 (347 to 1176) pg/ml for rate and rhythm groups respectively. Comparing the change in NT-proBNP concentrations over 1 year, a greater reduction was seen for those in the rhythm control group compared with rate control (−0.03 vs −0.23 log(NT-proBNP) for rate and rhythm control, respectively, p = 0.047). The greatest reduction in NT-proBNP concentration (from 1472 (797 to 1848) pg/ml to 458 (296 to 975) pg/ml) over 1 year was seen in those patients maintaining SR at 1 year, p = 0.005 compared with rate control).
Biochemical and haematological data
Haemoglobin fell by 1.0 (1.1) g/dl in the rhythm control group from 14.2 (1.4) g/dl at baseline to 13.4 (1.3) g/dl at 1 year (p = 0.036 compared with rate control). Creatinine rose in the rhythm control group by 18.5 (26.5) μmol/l from 105 (21) μmol/l at baseline to 121 (38) μmol/l at 1 year (p = 0.046 compared with rate control). By contrast, there was no change in haemoglobin (13.5 (1.4) g/dl at baseline; 13.2 (1.6) g/dl at 1 year) or creatinine (118.8 (37.8) μmol/l at baseline; 118.0 (34.7) μmol/l at 1 year) in the rate control group.
There was no difference between baseline and 1 year thyroid stimulating hormone concentrations (1.8 (1.1) mIU/l vs 1.9 (1.4) mIU/l, p = 0.970; 2.2 (1.6) vs 2.9 (3.0), p = 0.156 for rate and rhythm control groups respectively).
DISCUSSION
This randomised controlled trial conducted exclusively in patients with chronic HF and persistent AF suggests that a strategy of rhythm control can improve quality of life and left ventricular function compared with optimal rate control alone. The improvement in quality of life was due largely to an improvement in the physical functioning domain. The greatest improvement was seen in patients in whom SR was restored and maintained at 1 year follow-up.
The “Achilles heel” of a rhythm control strategy for AF is arrhythmia recurrence. Recurrence rates at 1 year for patients in published randomised studies range from 17% in the AFFIRM study to 43% and 44% in the STAF and PIAF studies respectively.4–6 Patients with heart failure may be prone to a higher rate of recurrence because they have structural heart disease and dilated atria, both of which are stimuli for AF recurrence.22 Accordingly, it may be futile to attempt cardioversion in patients with heart failure without additional steps to reduce recurrence. However, several antiarrhythmic drugs (particularly Class I) are associated with increased mortality in patients with ventricular dysfunction.23 24 Amiodarone is considered by many to be the antiarrhythmic drug of choice for patients with heart failure and AF, since it increases the efficacy of cardioversion and reduces the rate of AF recurrence.25 26 We were able to restore and maintain SR at 1 year (80% and 66% respectively) in our patients with cardioversion plus adjuvant amiodarone or with amiodarone alone. In our study, amiodarone was well tolerated by patients in the rhythm control group for at least 1 year. However, recent reports suggest that amiodarone might have an adverse long-term effect on mortality in patients with moderate or severe heart failure and LV systolic dysfunction,27 28 predominantly by worsening heart failure. The neutral outcome observed in the AF-CHF study may reflect the negation of the long-term benefits of sinus rhythm by the long-term adverse consequences of amiodarone.
Alternative methods of restoring and maintaining sinus rhythm in heart failure such as pulmonary vein isolation (PVI) (including PABA-CHF study),13 29 30 have shown encouraging short-term results and may have the advantage of avoiding the need for amiodarone therapy. However, the majority of patients in the PABA-CHF study had paroxysmal (65%) rather than persistent AF. Long-term maintenance of sinus rhythm with PVI may be less successful in persistent AF.
Treatments that are safe and improve symptoms have an important role in the management of heart failure. Retrospective analyses of patients with heart failure in the RACE study and the Canadian Trial of Atrial Fibrillation (CTAF) showed improvements in QoL only for those patients who could be maintained in SR.17 31 Our study population differs substantially from these, as did our routine use of amiodarone and relatively high rate of maintenance of sinus rhythm at 1 year. Our patients are more similar to those enrolled in AF-CHF. However, patients in AF-CHF were younger, and many had paroxysmal rather than persistent AF, which may account for their relatively high maintenance of sinus rhythm (79%) during long-term (37 months) follow-up.18
This study confirms that restoring SR in patients with left ventricular impairment can improve cardiac function as reported by others.14 16 32 There are several possible mechanisms for this, including (1) restoring the atrial contribution to ventricular filling, (2) regulating the cardiac cycle and (3) improvement in resting heart rate and chronotropic response to exercise. We believe that our study is the first randomised trial of cardioversion to show that restoring SR in patients with heart failure leads to a fall in natriuretic peptides.
Exercise performance and NYHA class were similar between groups at 1 year, but there was a suggestion that patients who maintained SR at 1 year might have improved, in keeping with other previous reports.33 The physical functioning component of the SF36vII improved, as did LV function, and so an improvement in exercise capacity might have been expected. However, exercise performance and QoL correlate poorly in patients with AF.34
Our study was analysed using the “intention to treat” rather than “per-protocol” principle to reduce bias in the assessment of each strategy. However, this approach may underestimate the true magnitude of the effect of restoring sinus rhythm, as benefit may be diluted by the inclusion of patients in whom the intended strategy failed. A per-protocol analysis identified greater improvements in QoL and walking distance at 1 year in patients who remained in SR. However, this could be biased in favour of cardioversion, since patients destined to do well might be more likely to remain in SR. Because of these uncertainties, intention to treat is the more rigorous and conservative estimate.
LIMITATIONS
The present study, in common with all other studies of rate versus rhythm control for patients with AF, was unblinded. Patient and observer bias could have influenced all of the results apart, perhaps, from NT-proBNP. Accordingly, our results should be interpreted with caution and viewed in the context of other studies. Our study was too small to evaluate effects on mortality. Although AF-CHF was a large multicentre study, it was designed primarily to assess the effects of intervention on major cardiovascular morbidity and mortality rather than symptoms and physical functioning. Our study provides complementary information. Our study suggests that cardioversion improves symptoms, and AF-CHF suggests that the strategy is safe.
Paroxysms of AF in between patient visits will have been missed if asymptomatic and could have had detrimental effects on cardiac function and heart-failure symptoms in patients assigned to rhythm control.
The improvement in LV function and QoL seen with rhythm control were not associated with a benefit in exercise capacity. Our study may have lacked adequate power to show an effect on 6MWT. NYHA may be too crude a measure adequately to detect a difference in symptom severity (unlike QoL tools). In addition to the 6MWT, formal cardiopulmonary exercise testing might have been a more robust method of evaluating the effect of rhythm restoration on exercise capacity in this setting.
CONCLUSIONS
Restoring sinus rhythm is feasible in a large proportion of patients with heart failure and persistent AF and, within the limits of this study, appears to lead to improved quality of life and left ventricular function. The AF-CHF study suggests that this strategy is also safe but does not improve long-term morbidity or mortality. These results combined may help to decide upon the “best treatment” strategy for an individual patient. However, given the modest benefits observed, cardioversion in this clinical setting may be appropriate only in selected cases.
REFERENCES
Footnotes
-
Competing interests: None.
-
Ethics approval: Ethics approval was provided by the Hull & East Yorkshire Ethics Committee.
-
Patient consent: Obtained.