Article Text

Abstract
Objective To assess the extent and the characteristics of hospital admissions in registered adult patients with congenital heart disease.
Design Observational cohort study.
Setting The Netherlands.
Patients 5798 adult patients with congenital heart disease from the Dutch CONCOR national registry linked to the Dutch National Medical Registration (Prismant).
Main outcome measures All hospital admissions from the years 2001 up until 2006.
Results During 28 990 patient-years, 2908 patients (50%) were admitted to hospital. Median age at admission was 39 years (range 18–86 years); 46% were male. Admission rate in CONCOR patients was high among all ages (range 11–68%) and exceeded that of the general Dutch population two to three times; this difference was most pronounced in the older age groups. Altogether there were 8916 admissions, 5411 (61%) of which were for cardiovascular indications. Among cardiovascular admissions, referrals for arrhythmias were most common (31%). Of 4926 interventions, 2459 (50%) were cardiovascular, most often reparative interventions or cardioversion (53%). Most non-cardiovascular admissions were obstetric. Among defects, univentricular heart and tricuspid atresia had the highest incidence and duration of admission.
Conclusions Healthcare utilisation in registered and medically supervised adult patients with congenital heart disease is high and increases with age. Admission rates are at least two times higher than in the general population, and most marked in the older age groups. With the ageing of this population, a major increase in healthcare utilisation is imminent in the near future. Timely preparation of healthcare resources is crucial to sustain optimal care.
- Marfans
- fallots tetralogy
- transposition of the great arteries
- epidemiology
Statistics from Altmetric.com
Introduction
Adult congenital heart disease has become a major health issue, comprising a population that is currently estimated at one million in the USA alone,1 and at least 1.2 million in Europe.2 These numbers will continue to rise in the future owing to the ongoing advances in cardiothoracic surgery and cardiac care. The distinct cardiac problems faced by this relatively novel patient population have well been recognised.3 The aim to improve and investigate survival in these patients has yielded ample literature on short-term outcome. In contrast, evidence on long-term prognosis is scarce yet suggests that, in the majority of cases, congenital heart surgery leaves patients with residual lesions for which lifelong medical surveillance is required.4
Mortality in adult patients with congenital heart disease has been shown to be increased.5 Moreover, morbidity in these patients appears to be substantial.6–8 Evidence of the impact of adult congenital heart disease on health care is scarce, yet shows an increased healthcare utilisation among these patients.9–11 With the ageing of this population, adequate evaluation of healthcare utilisation of adults with congenital heart disease regarding hospital admissions is critical to prepare for adequate healthcare resources in general and specifically for the various congenital heart defects. In addition, this will assist in informing patients more precisely on their future health perspectives.
We used the Dutch CONCOR national registry for adults with congenital heart disease to assess healthcare utilisation in terms of hospital admissions in registered and medically supervised adult patients with congenital heart disease.
Methods
CONCOR registry
The CONCOR (CONgenital CORvitia) Dutch national registry database has previously been described in detail.12 Briefly, CONCOR aims to facilitate research into the aetiology of congenital heart disease and on its outcome. From November 2001, patients with congenital heart disease aged 18 years or older have been recruited through the treating cardiologist or via response to advertisements in local media, and included by three independent, permanently employed research nurses. Clinical data such as diagnosis, clinical events and procedures—classified using the European Paediatric Cardiac Code Short List coding scheme13—as well as patient and family history were obtained from medical records. In case of multiple diagnoses in one patient, a pre-specified hierarchical scheme based on consensus-based classification of severity of diagnoses3 was used, by means of which the diagnosis with the worst prognosis was established as the main diagnosis. After entry, data on major cardiac events prior to entry and during follow-up were systematically recorded from medical letters on the patients' condition written by their cardiologist. Quality control of the data is routinely performed by randomly verifying around 10% of data each year. Currently, 102 hospitals are participating, including all eight tertiary referral centres from which approximately 70% of patients originate.
From CONCOR, date of birth, inclusion date, gender and main congenital heart diagnosis were derived. The severity of the main diagnosis was categorised as mild, moderate or severe, using a consensus-based classification scheme.3
Hospital admission data
Hospital admission data were obtained by linkage of the CONCOR database (n=7277 on date of linkage, 15 March 2007) to the Dutch National Medical Registration. Hospital admission was defined as a planned or unplanned admission of at least 24 hours including an overnight stay; visits to the outpatient clinic and emergency room were not included. Using a combination of zip code, gender and date of birth, the status of 95% of patients was assessed; 344 patients (5%) could not be linked owing to missing or erroneously registered zip codes. Of 6933 remaining patients, 1135 were excluded since they were younger than 18 years at the start of follow-up on 1 January 2001. National ancestry was provided as an approximation of ethnicity, and distinguished between native Dutch, non-native Western (originating from a European country (except Turkey)), North America, Oceania, Indonesia or Japan), and non-Western (Africa, South America, Asia (excluding Indonesia and Japan) or Turkey).
The number of hospital admissions in the linked CONCOR population was assessed from 1 January 2001 to 1 January 2006, thus yielding a follow-up duration of 5 years. No patients were lost during follow-up. For each hospital admission, a principal admission diagnosis was determined at discharge by the treating physician and coded by local hospital staff according to the International Classification of Diseases, ninth revision, clinical modification (ICD-9-CM).14 Admission diagnoses and procedures during admission were categorised as either cardiovascular (if the treating physician during admission was a cardiologist or a cardiothoracic surgeon, or in whom a cardiovascular diagnosis was certain) or non-cardiovascular. Cardiovascular admission diagnoses were occasionally not described further than symptomatic (eg, chest pain); for reasons of clarity and importance, these admissions were described separately. Non-cardiovascular admission diagnoses were further categorised according to the classification of the Dutch National Institute for Public Health and Environment (RIVM).15 In addition, the main procedure during admission was recorded and classified as either cardiovascular or non-cardiovascular. Cardiovascular procedures comprised surgical and percutaneous interventions aimed to correct or palliate congenital heart disease (such as valvar surgery and septal closure), cardioversion, diagnostic procedures (mainly consisting of catheterisation), pacemaker procedures (comprising new implantations, replacement and complications), ablation, ICD (implantable cardioverter defibrillator) procedures and other cardiovascular procedures or vascular interventions outside the coronary arteries, pulmonary artery or aorta, such as phlebotomy. Furthermore, all admissions were allocated to a tertiary and a non-tertiary medical centre. If a patient was transferred to another centre during hospital stay, the hospital admission was still considered as from the original medical centre in data analysis.
Figures on hospital admissions in the general Dutch population were obtained online from the Central Bureau of Statistics of The Netherlands (http://statline.cbs.nl).
Data analysis
Ages at the start of follow-up and at hospital admission were summarised using medians (range). Patient-years of follow-up were calculated by multiplying number of registrees by follow-up years. For distribution of congenital heart defects, defects comprising at least 65 patients were included in order to give an overview. For all other analyses, defects of patients comprising a group of at least 40 subjects were used in order to provide sufficient detail. Hospital admissions and procedures were counted in total and by defect. Hospital durations were summarised using means for the whole population and by defect. Trend was assessed using Spearman's rank correlation test.
To compare admission rates in CONCOR to the general Dutch population, the admission rate in CONCOR was calculated by dividing the number of CONCOR patients at least once admitted in 2005 (n=1146) by number of CONCOR patients within 10-year age groups. Similarly, the admission rate in the general population was assessed by dividing the number of all individuals admitted to hospital in The Netherlands in 2005 by the number of Dutch inhabitants on 1 January 2005 within 10-year age groups. We used SPSS 14.0 for data analysis.
Results
Of 5798 patients available for analyses, 2862 were male (49%). During a total follow-up duration of 28 990 patient-years, 2905 patients (50%) were admitted to hospital. Median age at admission was 39 years (range 18–86 years); 46% of admitted patients were male. In total, 57 patients (2.0% of admitted patients) died during admission in hospital.
Table 1 shows the baseline characteristics of the study population. Median age at the start of follow-up was 32 years (range 18–85 years); 83% of patients were below 50 years of age. Of all patients, 20% were admitted to hospital three or more times during 5 years of follow-up.
Baseline characteristics of CONCOR patients (n=5798)
Table 2 shows the proportional distribution of underlying congenital heart defects in the study population. Six of the most common congenital heart defects (atrial septal defect, ventricular septal defect, tetralogy of Fallot, aortic coarctation, aortic stenosis and pulmonary stenosis) covered 70% of diagnoses. Patients with patent arterial duct, atrial septal defect and Ebstein's anomaly were oldest (40–45 years), whereas those with pulmonary atresia, transposition of the great arteries and atrioventricular septal defect were youngest (24–27 years). Among patients with transposition of the great arteries, 3% had undergone an arterial switch procedure before enrolment.
Proportional distribution of main congenital heart defects and age by defect (n=5798)
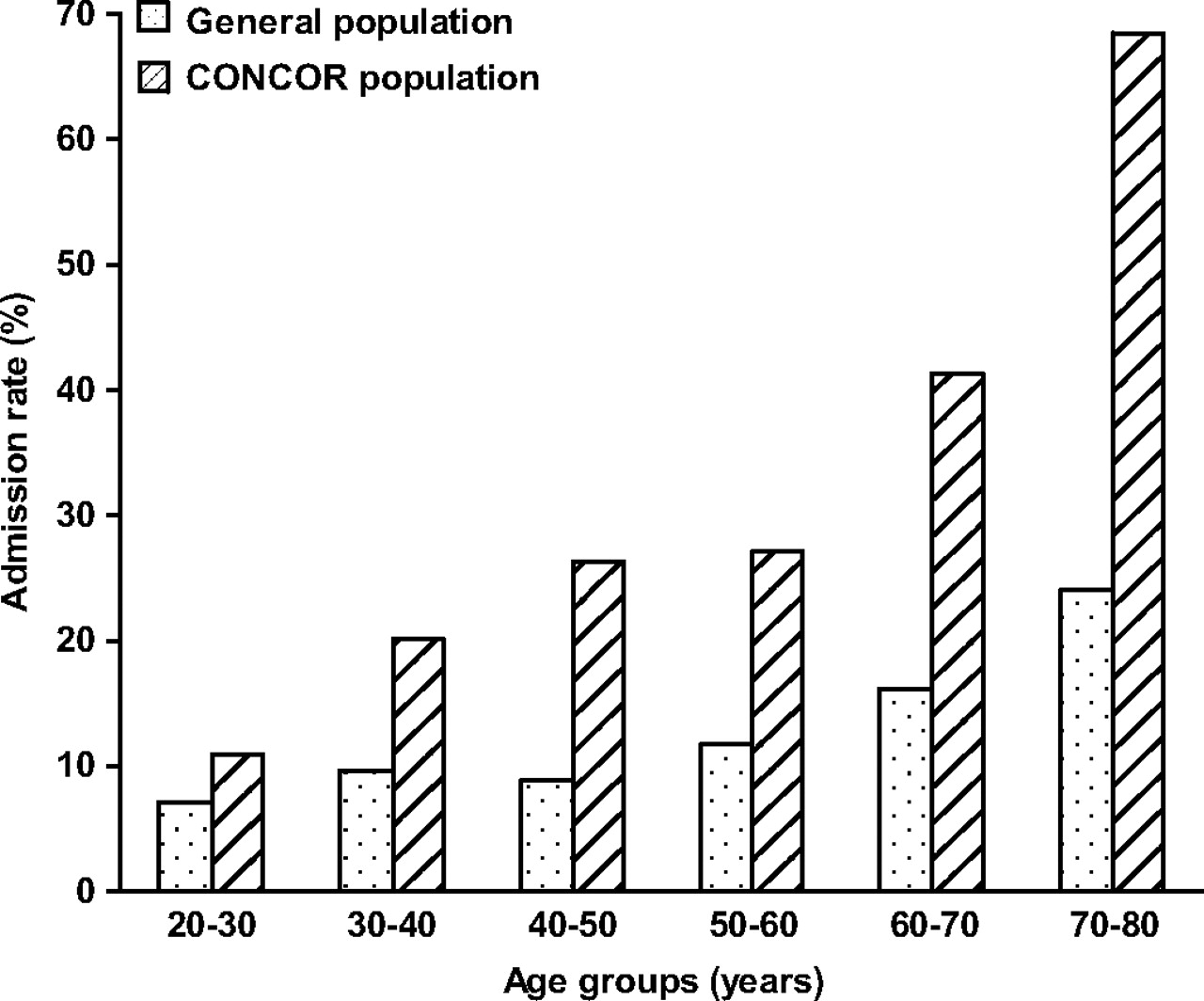
Figure 1 compares admission rate among CONCOR patients with the admission rate of the general Dutch population in the year 2005. The admission rate was high among all age groups, varying from 11% in the youngest age group to 68% in the highest group. Above 40 years, one in four patients was admitted to hospital at least once during the 5-year follow-up period; this frequency increased with age. In all age groups above age 30, the admission rate of CONCOR patients was two to three times higher than that of the general Dutch population. This difference in admission rate was most marked in the age groups above 40 years.
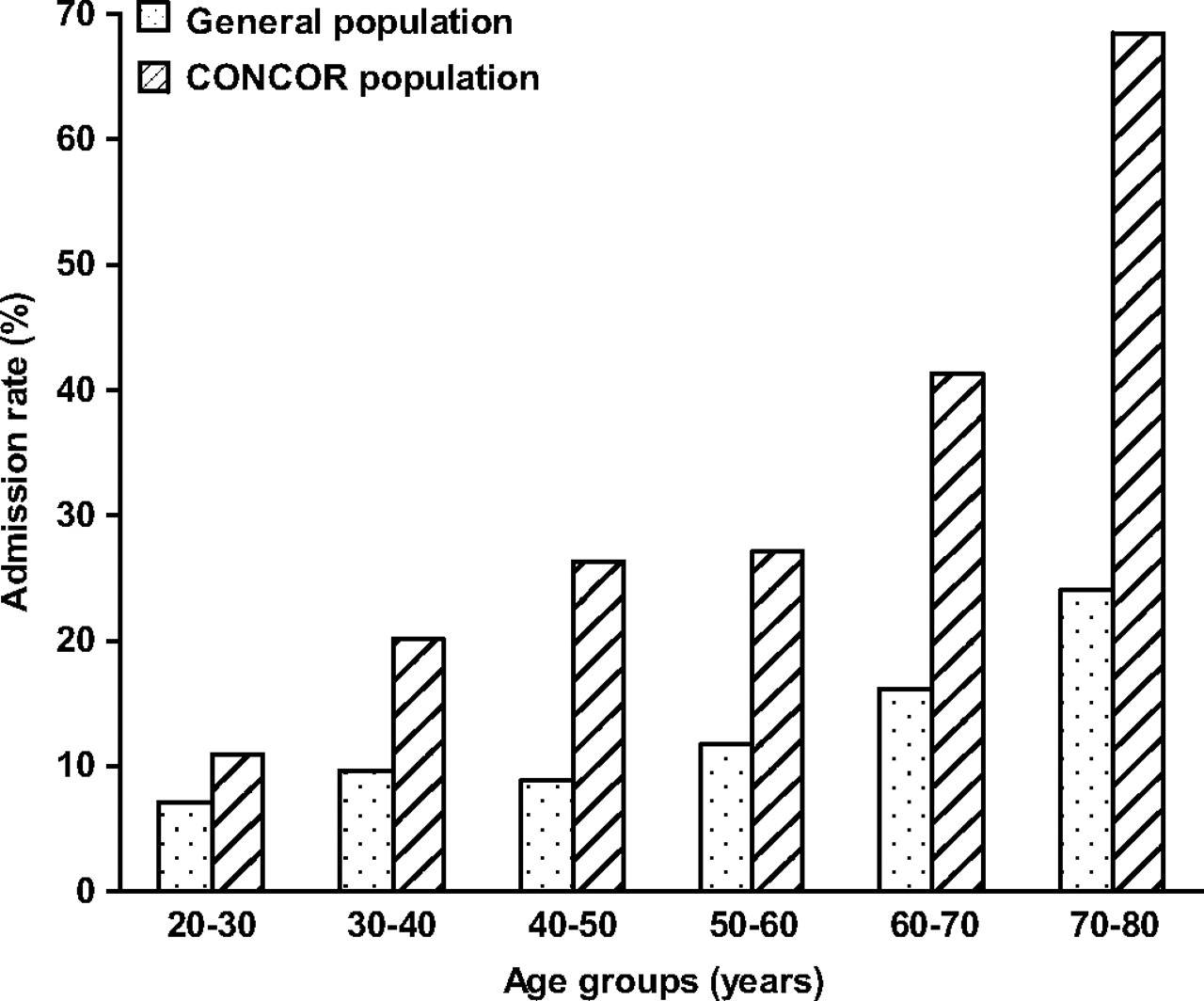
Admission rate in CONCOR patients and in the general Dutch population by decade in 2005.
During 5 years, there were 8916 hospital admissions; the hospitalisation rate was 308 hospitalisations/1000 patient-years. The number of admissions increased significantly each year (p for trend <0.001). In 5411 hospital admissions (61%) the reasons for admission were cardiovascular. The most frequent cardiovascular admission diagnoses are shown in figure 2. Arrhythmias accounted for 31% of cardiovascular admissions. Patients admitted for chest pain most often had an atrial septal defect or an aortic coarctation at a median age of 41 years; 16% underwent a catheterisation at a median age of 53 years. Among the patients with pacemaker admissions, 45% was admitted for new implantation of a pacemaker. Patients admitted for coronary artery disease were on average 52 years old and most often had an atrial or ventricular septal defect; median age of the catheterised patients (27%) was 59 years. Endocarditis was the main admission diagnosis in 88 hospital admissions (1.6%).

Most frequent cardiovascular admission diagnoses/symptoms in the CONCOR population (n=5798) 2001–2005. All cardiovascular admissions with n≥100 are displayed. nos=not otherwise specified.
Figure 3 shows the most frequent non-cardiovascular admission diagnoses. Patients were most often admitted for obstetric reasons, 45% of which included delivery. The most frequent obstetric admissions not including delivery were sterilisation (8%), imminent preterm birth (6%) and missed abortion (4%). Patients were admitted equally often for obstetrics compared to the Dutch population (both 2–3% between 20 and 40 years of age). The frequency of admissions for neoplasms was also similar to that of the general Dutch population.

Most frequent non-cardiovascular admission diagnoses in the CONCOR population (n=5798) in the years 2001–2005. All non-cardiovascular admissions with n≥100 are displayed. The hospital admissions for blood (forming) organs concern admission diagnoses such as anaemia.
In 4926 admissions (53% of all admissions), patients underwent a procedure. Of these procedures, 2459 (50%) were cardiovascular, of which the most important are shown in table 3. Interventions for congenital heart disease and cardioversion together accounted for 53% all of cardiovascular procedures.
Cardiovascular procedures during hospital admission (n=2459)
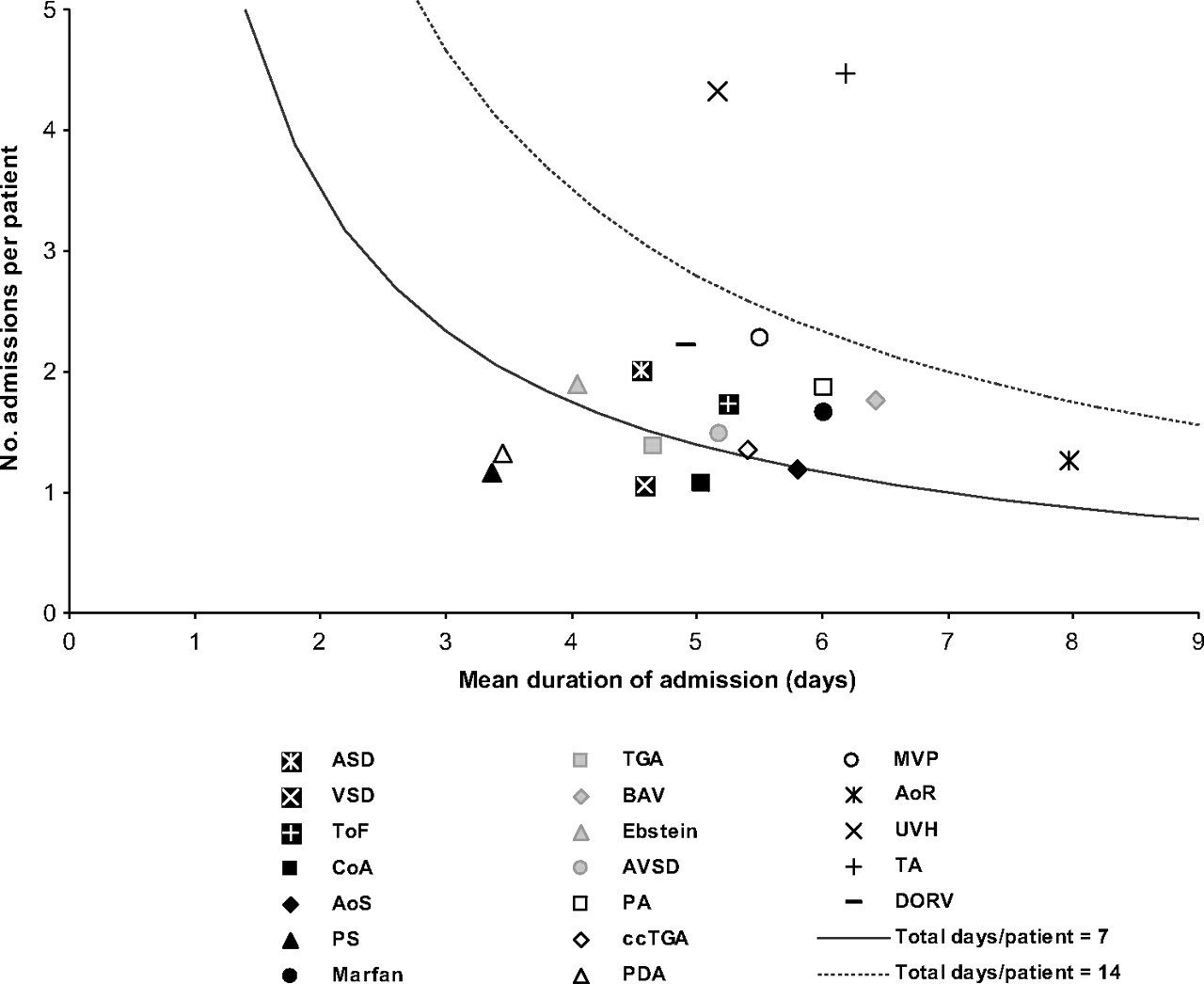
Figure 4 shows the number of admissions per patient and the mean duration of hospital admission by defect. Multiplication of these numbers renders the total duration of admission per patient by defect; the curves represent 1 and 2 weeks of total duration of hospital admission, respectively. Below the curve of 1 week of total duration of hospital admission were patent arterial duct, pulmonary stenosis, ventricular septal defect, aortic coarctation, transposition of the great arteries and aortic stenosis. Above the curve of 2 weeks of total duration of hospital admission were univentricular heart and tricuspid atresia. Restriction of the analyses to cardiovascular admissions revealed a similar pattern.

Number of all hospital admissions per patient and mean duration of hospital admission by defect. Admissions in the years 2001–2005. Included are all defects with n>40, displayed in descending order of frequency. AoR, aortic regurgitation; AoS, aortic stenosis; ASD, atrial septal defect; AVSD, atrioventricular septal defect; BAV, bicuspid aortic valve; ccTGA, congenitally corrected transposition of the great arteries; CoA, aortic coarctation; DORV, double outlet right ventricle; Ebstein, Ebstein's malformation; Marfan, Marfan syndrome; MVP, mitral valvar prolapse; PA, pulmonary atresia; PDA, patent arterial duct; PS, pulmonary stenosis; TA, tricuspid atresia; TGA, transposition of the great arteries; ToF, tetralogy of Fallot; UVH, univentricular heart; VSD, ventricular septal defect. The curves represent the total number of days (7 and 14, respectively) for which a patient is admitted to hospital by defect.
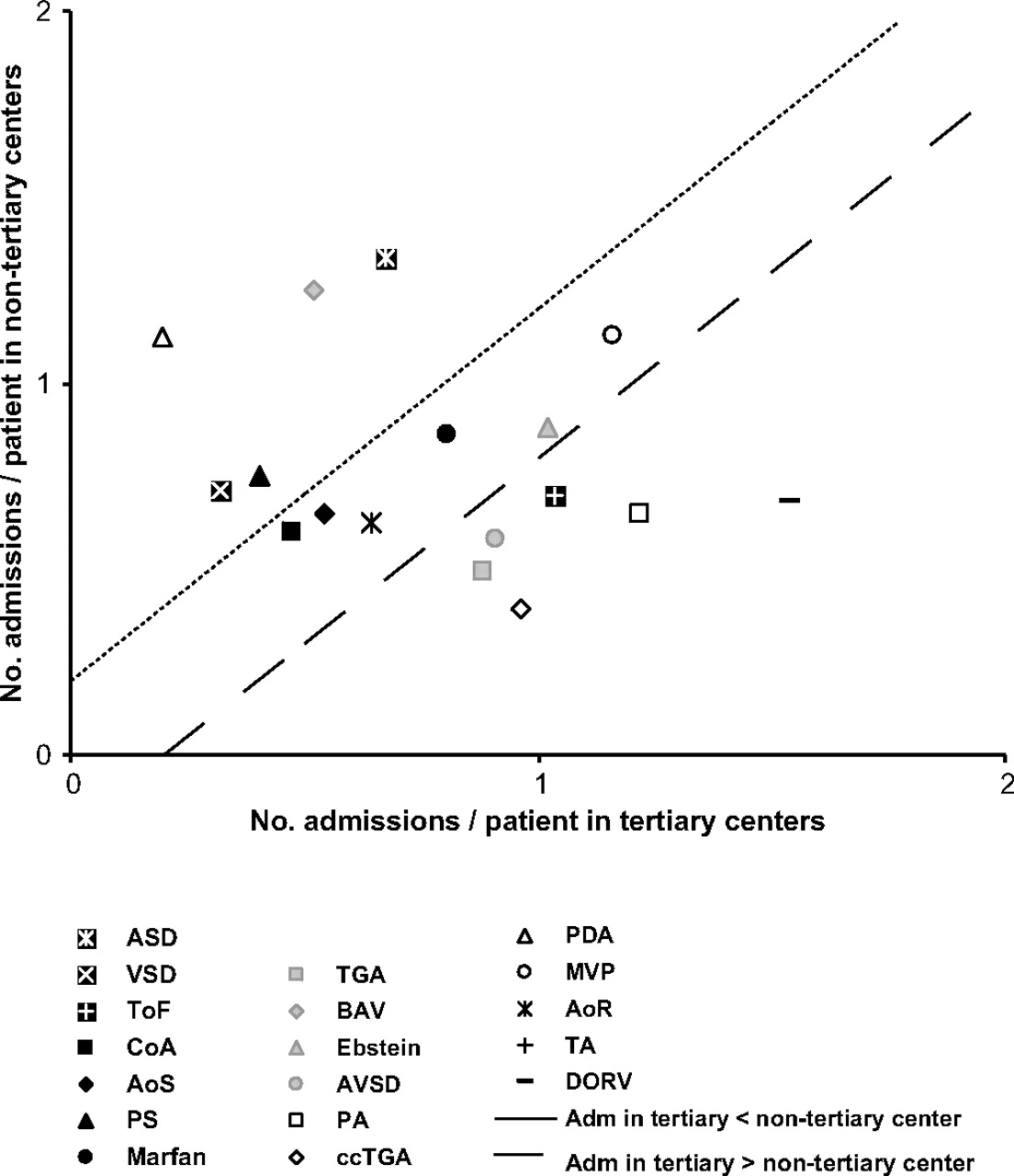
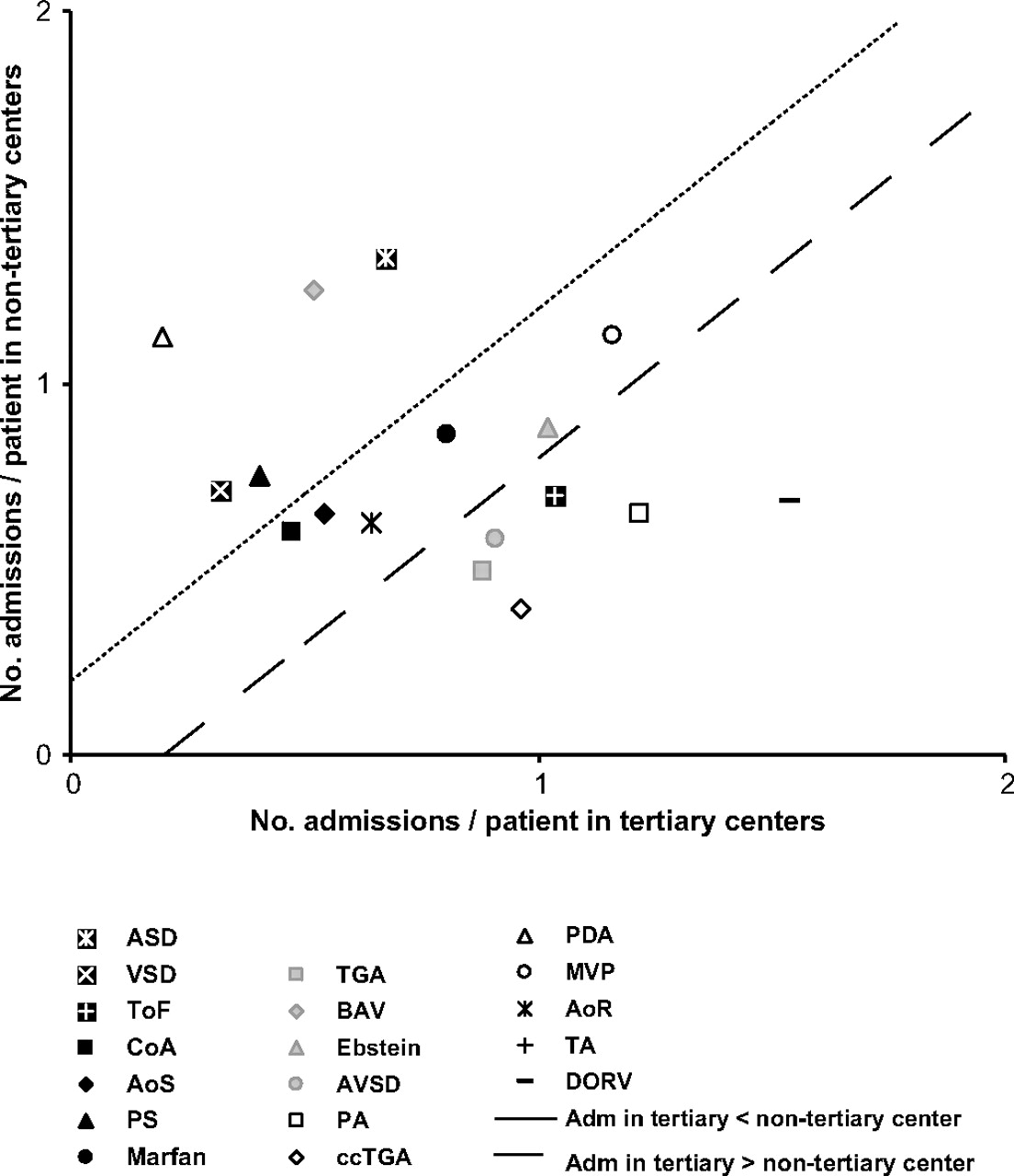
Figure 5 shows the number of admissions per patient in tertiary (45%) and non-tertiary centres (55%) separately by defect. Patients with defects left of the left-hand line were more frequently admitted to non-tertiary centres than to tertiary referral centres: atrial septal defect, patent arterial duct and bicuspid aortic valve. Patients with defects right of the right-hand line were more often admitted to tertiary referral centres; this was most pronounced in tricuspid atresia and double-outlet right ventricle. The defects between the lines were distributed more or less equally over tertiary and non-tertiary centres.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Number of admissions per patient in tertiary and in non-tertiary centres by defect. Admissions in the years 2001–2005. Included are all defects with n>50 except univentricular heart, displayed in descending order of frequency. See legend of figure 4 for abbreviations. Adm, admissions.
Discussion
The present study is the first to evaluate the characteristics and the extent of the emerging burden of disease in terms of hospital admissions in registered adult patients with congenital disease using in a large nationwide population. Adult patients with congenital heart disease have high admission rates at all ages, which further increase with ageing. Compared to the general Dutch population, hospital admission rate was two to three times higher. Two-thirds of admissions were cardiovascular. Among defects, patients with tricuspid atresia or univentricular heart had a particularly high utilisation of health care.
Strengths and limitations
The particular strengths of our study are the large number of patients, the rigorous and uniform methods of recording data and the robust database linking process. Moreover, CONCOR is the first large scale and nationwide registry of adults with congenital heart disease, thus adding substantially to evidence applicable to these patients. The limitations are that CONCOR neither comprises very mild congenital heart disease in patients lost to medical surveillance nor critical congenital heart disease that led to death prior to enrolment. Complex congenital heart disease may be over-represented as most patients were registered by tertiary referral centres. Furthermore, we had no information on the number of hospital admissions in which transfers between tertiary and non-tertiary centres took place; this number will be small as only few indications require such a transfer. Finally, we could only address part of the healthcare utilisation of these patients as visits to the outpatient clinic, the emergency room or the general practitioner were not included. However, our data clearly describe actual hospital admission, since an admission was defined as a hospital stay of at least 24 hours.
Relation to current literature
At present, the vast majority of adults with congenital heart disease are still under the age of 50 years, a finding described previously,16 and corresponding with the notion that open heart surgery became widely available only a few decades ago. But adults with congenital heart disease grow older.16 Therefore, a rise in the number of adults with congenital heart disease above 50 years is to be expected in the near future.
We found half of our patients admitted during 5 years of follow-up, which is in concordance with previous numbers.10 Furthermore, our findings showed high admission rates among adult patients with congenital heart disease that increased with age, and markedly exceeded that of the general population, as reported earlier.10 The occurrence of major cardiac complications at all ages with a clear tendency to increase with age has well been recognised.4 In terms of disability adjusted life years (DALY), congenital heart disease has a ranking similar to prominent non-infectious diseases such as asthma, rheumatoid arthritis and breast cancer.17 Moreover, the population of adults with congenital heart disease has been shown to grow in number at an estimated 5% per year,1 18 as well as in severity.16 Thus, the population of adults with congenital heart disease is not only expanding, but also growing older, and more often has complex underlying cardiac defects. This will further impact on the level of healthcare utilisation, especially among older adults.
We found our patients to be admitted most frequently for arrhythmias as well as for chest pain, in agreement with previous reports.9 19 The number of catheterisations in patients admitted for chest pain was low, suggesting that the chest pain was most often atypical. Moreover, patients admitted for chest pain as well as coronary artery disease were relatively old, which suggests that age was a more important argument to admit patients to hospital than their underlying congenital heart defect.
Our findings indicate that frequency and duration of hospital admission, as an approximation for healthcare utilisation, varied considerably by defect. As expected, this variation largely corresponds with the consensus-based classification of severity of defects, as previously reported.3 10 However, transposition of the great arteries was associated with less healthcare utilisation, in terms of hospitalisations as defined, than we expected. This may be explained by the combination of the type of reparative surgery and healthcare allocation. The patients with transposition of the great arteries included in this study have almost invariably undergone an atrial switch operation, and are generally under the medical surveillance of a tertiary referral centre; such centres are equipped with a special emergency unit for heart patients where they go for cardioversion of the arrhythmias to which they are prone. Thus, technically they are not admitted to hospital but treated in the specialised outpatient emergency room, leading to an underestimation of hospital admissions among these patients. Finally, healthcare utilisation of atrial septal defects was higher than we expected. This may be due to their older age, leading to more hospital admissions for both cardiovascular and non-cardiovascular problems.
As expected, we found the milder defects to be most often admitted in non-tertiary centres, and severe defects primarily in tertiary referral centres. Currently, the expertise on adult congenital heart disease is concentrated in tertiary referral centres. Notwithstanding the importance of these centres regarding experience, research and education, the impending increase in healthcare utilisation for both cardiovascular and non-cardiovascular health problems in adults with congenital heart disease warrants expansion of the expertise to non-tertiary centres.
Future research and implications
Each year the population of adults with congenital heart disease grows both in number and in age, thus representing a larger proportion of the whole population. With the high and yearly increasing hospital admissions rate, especially among older adults, the expected rise of healthcare utilisation of these patients in the near future is alarming. Therefore, the re-allocation of both quantitative and qualitative healthcare resources needs to be considered. Tertiary centres may expand their facilities for adult patients with congenital heart disease and enhance multidisciplinary long-term care for complex defects; the electrophysiological burden could be prevented or diminished by reducing the number of heart incisions and early operations. Non-tertiary centres have to be prepared for the needs of these vulnerable yet relatively unfamiliar patients, such as emergency treatment of arrhythmias, ablations and heart failure. More cardiologists need to be trained in the provision of optimal care tailored to patients with congenital heart disease in both tertiary and non-tertiary medical centres.20 This importance is also stressed by the fact that not only the number of cardioversions but also the number of ablations will greatly increase. Furthermore, more in-depth research is warranted regarding the characteristics of hospital admissions, such as the differentiation between emergency versus planned admissions. Moreover, to guide policymaking, additional information is needed such as estimating their healthcare burden in terms of costs. In Europe there are currently some 728 million inhabitants with an estimated 1.2–2.7 million adults with congenital heart disease; this number is currently believed to be at least one million in the USA, making a population of 306 million. In the present study, we have found that the Dutch population of adult patients with congenital heart disease generates some 308 hospital admissions per 1000 patients per year. Extrapolating our findings, we would expect at least 308 000 hospital admissions in the USA and 370 000–832 000 hospital admissions in the European Union for, for example, the year 2010. This would be a conservative estimate given that the population of adults with congenital heart disease will further increase.
In conclusion, healthcare utilisation of registered and medically supervised adult patients with congenital heart disease is high and increases with age. Admission rates are two to three times higher compared to the general population, and most marked among the older age groups. With ageing of this expanding population, a major increase in healthcare utilisation is imminent in the near future. Timely recruitment of healthcare resources is crucial to sustain optimal care.
Acknowledgments
We thank Agnes de Bruin, Janneke Ploemacher and Fred Gast of the Central Bureau of Statistics of The Netherlands and Prismant for linking the hospital admission data and facilitating this study. We also thank the Dutch medical institutions and their study coordinators for participating in the CONCOR project (appendix). Finally, we thank Lia Engelfriet, Irene Harms and Sylvia van den Busken of the Academic Medical Centre for their dedicated support of the CONCOR project.
Appendix
The following Dutch medical institutions and study coordinators participate in the CONCOR project. Academisch Medisch Centrum, Amsterdam: BJM Mulder; Academisch Ziekenhuis Maastricht, Maastricht: JLM Stappers; Albert Schweitzer Ziekenhuis, locatie Amstelwijck / Dordwijk, Dordrecht; Alysis Zorggroep, locatie Rijnstate, Arnhem: HA Bosker; Alysis Zorggroep, locatie Zevenaar, Zevenaar: P van den Bergh; Amphia Ziekenhuis, Breda: HPJ de Haan; Antonius Ziekenhuis, Sneek: A Oomen; Atrium Medisch Centrum, locatie Heerlen, Heerlen: L Baur; Bethesda Ziekenhuis, Hoogeveen: SHK The; BovenIJZiekenhuis, Amsterdam: ALM Bakx; Bronovo Ziekenhuis, 's-Gravenhage: PRM Dijkman; Canisius Wilhelmina Ziekenhuis, Nijmegen: JJ Remmen; Cardiologie Centrum Amsterdam Zuid, Amsterdam; Catharina Ziekenhuis, Eindhoven: JJ Koolen; Centraal Militair Hospitaal, Utrecht: R Rienks; Delfzicht Ziekenhuis, Delfzijl: JHZ Banki, JN Spanjaard; DeventerZiekenhuizen, Deventer: DJA Lok; Diaconessenhuis, Leiden; Diaconessenhuis, Meppel: K Thomas; Diakonessenhuis, Utrecht / Zeist; Elkerliek Ziekenhuis, Helmond; Erasmus Medisch Centrum, Rotterdam: JW Roos-Hesselink; Flevoziekenhuis, Almere: ASJM Sadee; Franciscus Ziekenhuis, Roosendaal: RJ Bos; Gelre Ziekenhuizen, locatie Juliana, Apeldoorn: L Cozijnsen; Gelre Ziekenhuizen, locatie het Spitaal, Zutphen: NYY Al-Windy; Gemini Ziekenhuis, Den Helder: JGM Tans; Groene Hart Ziekenhuis, Gouda; Haga Ziekenhuis, locatie Leyweg, 's-Gravenhage: BJM Delamarre; Haga Ziekenhuis, locatie Sportlaan, 's-Gravenhage; Havenziekenhuis, Rotterdam: CM Leenders; Hofpoort Ziekenhuis, Woerden; IJsselland Ziekenhuis, Capelle aan den IJssel; IJsselmeer Ziekenhuizen, Lelystad / Emmeloord: JM Ansink; Ikazia Ziekenhuis, Rotterdam: JP Kerker; Isala Klinieken Weezenlanden / Sophia, Zwolle: JCA Hoorntje; Jeroen Bosch ziekenhuis, locatie Carolus, 's-Hertogenbosch: ECM Schavemaker; Jeroen Bosch Ziekenhuis, locatie Groot Ziekengasthuis, 's-Hertogenbosch: E Krivka; Kennemer Gasthuis, locatie Zuid, Haarlem: R Tukkie; `t Lange Land Ziekenhuis, Zoetermeer; Laurentius Ziekenhuis, Roermond: CJPJ Werter; Leids Universitair Medisch Centrum, Leiden: HW Vliegen; Maasziekenhuis Pantein, Boxmeer; Maasland Ziekenhuis, Sittard: LGH Brunnikhuis; Maasstadziekenhuis, locatie Clara / Zuider, Rotterdam; Martini Ziekenhuis, Groningen: L Bartels; Máxima Medisch Centrum, Veldhoven / Eindhoven: RF Visser; Meander Medisch Centrum, Amersfoort: SM Roeffel; Medisch Centrum Alkmaar, Alkmaar: CLA Reichert; Medisch Centrum Haaglanden, locatie Antoniushove, Leidschendam; Medisch Centrum Haaglanden, locatie Westeinde, 's-Gravenhage; Medisch Centrum Leeuwarden, Leeuwarden: CJ de Vries; Medisch Spectrum Twente, Enschede: EMCJ Wajon; Onze Lieve Vrouwe Gasthuis, Amsterdam: R Riezebos; Oosterschelde Ziekenhuizen, Goes: HWO Roeters van Lennep; Refaja Ziekenhuis, Stadskanaal: AG Vijn; Reinier de Graaf Ziekenhuis, Delft; Rijnland Ziekenhuis, Leiderdorp / Alphen aan den Rijn; Rivas Zorggroep, Gorinchem; Rode Kruis Ziekenhuis, Beverwijk: JHM Spekhorst; Röpcke-Zweers Ziekenhuis, Hardenberg / Coevorden: AJ Schaap; Ruwaard van Putten Ziekenhuis, Spijkenisse; Scheper Ziekenhuis, Emmen: L van de Merkhof; Sint Anna Ziekenhuis, Geldrop: PE Polak; Sint Antonius Ziekenhuis, Nieuwegein: HWM Plokker; Sint Elisabeth Ziekenhuis, Tilburg; Sint Franciscus Ziekenhuis, Rotterdam: MJ Veerhoek; Sint Jans Gasthuis, Weert: HC Klomps; Sint Lucas Andreas Ziekenhuis, Amsterdam: RGEJ Groutars; Sint Lucas Ziekenhuis, Winschoten: NM de Groot-van Popele; Slingeland Ziekenhuis, Doetinchem: JMC van Hal; Slotervaart Ziekenhuis, Amsterdam: AG Veerbeek; Spaarne Ziekenhuis, Hoofddorp: AFM Kuijper; Streekziekenhuis Koningin Beatrix, Winterswijk: C van der Lee; Talma Sionsberg, Dokkum: AW Hagoort-Kok; Tergooiziekenhuizen, locatie Blaricum, Blaricum: G Hoedemaker; Tergooiziekenhuizen, locatie Hilversum, Hilversum: J Plomp; Tweesteden Ziekenhuis, Tilburg: MS Hulsbergen-Zwarts; Universitair Medisch Centrum Groningen, Groningen: PG Pieper; Universitair Medisch Centrum Sint Radboud, Nijmegen: APJ van Dijk; Universitair Medisch Centrum Utrecht, Utrecht: BJM Mulder, GTj Sieswerda; Universitair Ziekenhuis Gent, Gent; VieCuri Medisch Centrum, Venlo / Venray: BM Rahel; Vlietland Ziekenhuis, Vlaardingen / Schiedam; VU Medisch Centrum, Amsterdam: G Veen, TC Konings; Waterland Ziekenhuis, Purmerend: M Mihciokur; Westfriesgasthuis, Hoorn: PFMM van Bergen; Wilhelmina Ziekenhuis, Assen: IJ van Eede; Ziekenhuis Amstelland, Amstelveen; Ziekenhuis Bernhoven, Oss / Veghel; Ziekenhuis Bethesda, Dirksland; Ziekenhuis de Gelderse Vallei, Ede: TT van Loenhout; Ziekenhuis de Heel, Zaandam; Ziekenhuis Lievensberg, Bergen op Zoom; Ziekenhuis Nij Smellinge, Drachten: RPLM van der Aa; Ziekenhuis Rivierenland, Tiel; Ziekenhuis Sint Jansdal, Harderwijk: R Dijkgraaf; Ziekenhuis de Tjongerschans, Heerenveen: SK Oei; Ziekenhuis Walcheren, Vlissingen: WH Pasteuning; Ziekenhuisgroep Twente, Streekziekenhuis Midden-Twente, Hengelo: L Pos; Ziekenhuisgroep Twente, Twenteborg Ziekenhuis, Almelo: GCM Linssen; ZorgSaam Zeeuws-Vlaanderen, Terneuzen: CAW Janssens.
References
Footnotes
Funding Interuniversity Cardiology Institute of the Netherlands, and the Netherlands Society of Cardiology.
Competing interests None.
Ethics approval This study was conducted with the approval of the Academic Medical Centre, The Netherlands.
Provenance and peer review Not commissioned; externally peer reviewed.