Article Text

Abstract
Objective To accurately compare the radiation dose between prospectively gated cardiac multidetector CT (with and without iterative reconstruction) and diagnostic invasive coronary angiography using the latest International Commission on Radiological Protection 103 (ICRP) tissue weightings.
Design, setting and patients A retrospective analysis of consecutive patients presenting to a university teaching hospital for investigation of coronary artery disease. Radiation doses for each technique were calculated using computational Monte Carlo modelling of a standard Cristy phantom rather than the application of previously published conversion factors. While these have frequently been used in other studies, they are based on out-dated ICRP tissue weightings (ICRP 60) and are for the whole chest rather than for structures irradiated in cardiac imaging. In order to allow a comparison, doses were calculated and expressed in terms of effective dose in millisieverts (mSv).
Results From a population presenting for angiography within a clinical service, the median radiation dose from cardiac CT with standard filtered back-projection (84 patients, 5.4 mSv) was comparable with the dose from invasive diagnostic coronary angiography (94 patients, 6.3 mSv). The dose for cardiac CT using iterative reconstruction was significantly lower (39 patients, 2.5 mSv).
Conclusion The median effective dose from cardiac CT with standard filtered back-projection was comparable with the effective dose from invasive coronary angiography, even with application of the most contemporary ICRP tissue weightings and use of cardiac specific volumes. Cardiac CT scanning incorporating iterative reconstruction resulted in a significant reduction in the effective dose.
- Effective dose
- CT angiography
- prospective ECG gating
- invasive angiography
- CT scanning
- coronary artery disease (CAD)
Statistics from Altmetric.com
- Effective dose
- CT angiography
- prospective ECG gating
- invasive angiography
- CT scanning
- coronary artery disease (CAD)
Since its advent, the use of multidetector CT (MDCT) for the diagnosis of coronary artery disease has been increasing in frequency. It now has an established role in the diagnosis of patients with an intermediate pretest likelihood of coronary artery disease1 because of the accuracy of the investigation, particularly when compared with other noninvasive modalities. MDCT is becoming more available, and in centres with an established programme, the rates of invasive coronary angiography have fallen.2
The radiation dose from MDCT is a common subject in the literature,3–5 and comparisons have been made with conventional invasive coronary angiography.6 7 Recently, because of the concerns regarding the radiation exposure in a relative well and young population, radiation reduction strategies have been a major area of research.8 9
One method of comparing the radiation dose from two differing imaging modalities is the calculation of effective dose. This quantity takes into account the differing type and energy of the radiation source and also the biological harm from exposure to a particular organ (tissue weighting). Its primary use is to define the risk of a health detriment due to the stochastic effects of ionising radiation to a population, rather than the calculation of risk for a specific individual.10 The commonest method of estimating the effective dose from a cardiac CT scan is the use of a conversion factor applied to the dose length product (DLP) of the examination.11 The DLP is the helical pitch-corrected radiation dose from each slice of the CT scan (volume weighted Computed Tomography Dose Index (CTDIv), mGy) multiplied by the length (cm) of the scan in the z-axis (head to foot plane) and is available from the individual scan dose report.
Conversion factors previously used in the literature have varied4 8 12 13 between 0.014 and 0.019 mSv/mGy.cm and are based on helical chest CT using the tissue weightings derived from the International Commission on Radiological Protection (ICRP 60; 1991) document of radiation risk for the whole chest.
There has been a recent change in the ICRP tissue weightings (2007) following the latest available scientific information of the biology and physics of radiation exposure; particularly, the tissue weighting for breast tissue has increased from 0.05 to 0.12 (ICRP 103).14 Additionally, the scan area of cardiac CT is not reflected well by a conversion factor for the whole chest because the scan volume, in cardiac CT, covers the mid chest to the upper abdomen.
Earlier cardiac CT was performed using a helical scan and retrospective gating algorithms (figure 1), and the radiation dose remained relatively high up to 21 mSv.15

Retrospective ECG gating utilises a helical scanning technique. The tube current (mA, grey area) is on for the entire length of the scan but fluctuates because of programmed dose modulation.
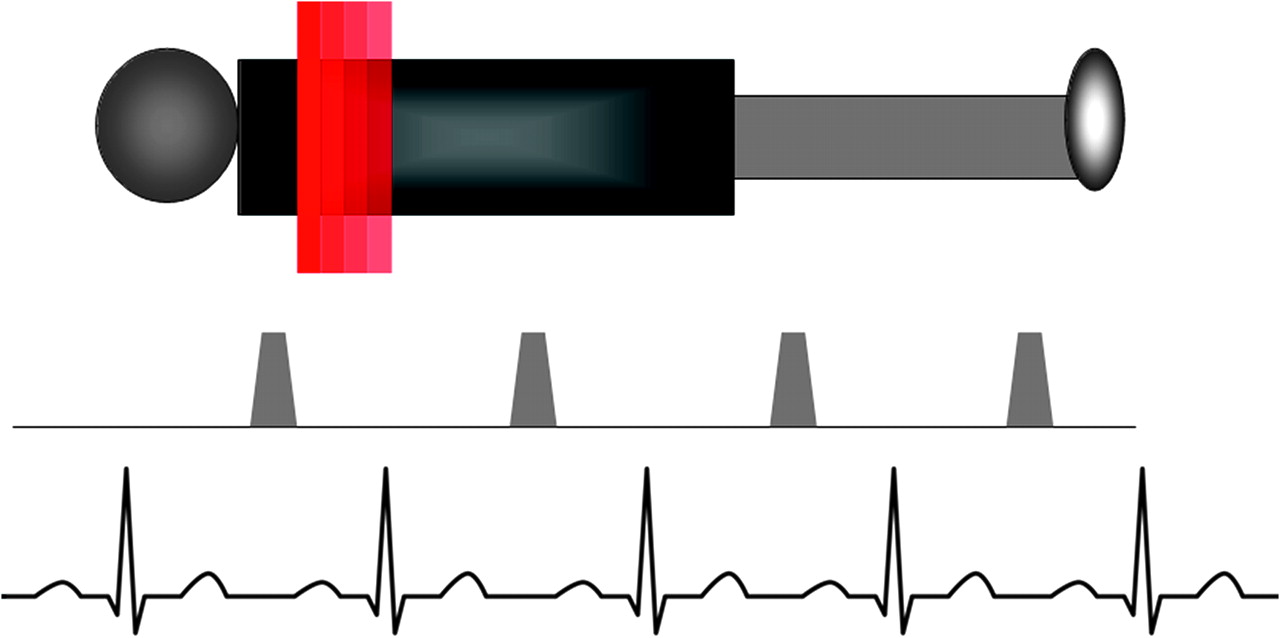
Cardiac CT utilising prospective gating is performed axially (step-and-shoot), and the x-ray current is only turned on for a fraction of a second during diastole (figure 2).16 This development has significantly reduced the examination radiation dose and has become the default technique for the majority of patients.

The step-and-shoot technique with prospective ECG gating uses an axial imaging conformation. The tube current (shaded area) is only on for a short period of time during diastole and relative cardiac stasis.
A new reconstruction technique, iterative reconstruction, is used in this study. This uses more complex mathematical modelling for image reconstruction, which in turn reduces image noise and enables a reduction in the scan mA and therefore examination radiation dose. Iterative reconstruction is compared with cardiac CT with standard filtered back-projection (FBP).
A conversion factor (based on ICRP 60), initially conceived to provide a relatively easy estimation of effective dose for a helical chest CT scan, does not provide an accurate calculation for the effective dose from a cardiac CT scan because of the changes in the ICRP tissue weightings and the significant difference in the scan volume between a cardiac and chest CT.
Conversion factors for conventional invasive coronary angiography have also recently been used.6 17–19 These are also based on older ICRP 60 tissue weightings. Published conversion factors vary widely from 0.12–0.26 mSv/Gy cm2.
This is the first study to take into account the latest ICRP 103 tissue weightings and apply them to prospectively gated cardiac CT. It is also the first to compare doses between a standard scanner with FBP and one utilising iterative reconstruction.
The objective of this study was therefore to provide the most contemporary comparison of the effective radiation dose between standard (FBP) and state-of-the-art cardiac CT using iterative reconstruction and invasive coronary angiography.
Method
Invasive coronary angiography
As part of the ongoing radiation audit at a Plymouth Hospital NHS Trust, we undertook detailed examinations of 110 consecutive patients attending for invasive coronary angiography in one of two catheter laboratories. Sixteen of these patients were used to calculate our own hospital-specific conversion factor for invasive coronary angiography, and this was then applied to 94 patients attending for day-case angiography. Exclusion criteria included non-coronary indication such as valve disease and pre-electrophysiological studies, extreme variance in weight (body mass index (BMI) <20 to >35), previous coronary bypass graft and acute coronary syndrome. Therefore, our patient cohort consisted of outpatients undergoing day-case catheter procedures for the diagnosis of coronary disease.
A retrospective analysis of each examination was undertaken to avoid alteration of the technique because of the audit. The operators were unaware of the audit at the time of the angiography, and there were no restrictions placed on the operators to use a particular angiographic projection or technique. Access within the centre is predominantly radial, and all examinations were undertaken using the transradial approach. The operators included consultant cardiologists and registrars all with >5 years' experience of invasive diagnostic coronary angiography.
Effective dose from invasive coronary angiography
Flat plate Phillips Allura XPER FD10 (Phillips, Eindhoven, Holland) catheterisation equipment was used. A retrospective analysis of the patients was performed, and 8–10 views were acquired as standard.
Previous studies have used a conversion factor (0.22 mSv/Gy cm2) to calculate an effective dose from the total dose area product (DAP) for the examination.6 The DAP is a radiation dose quantity measuring the charge collected from an ionisation chamber (in air) multiplied by the area of the x-ray field. The total examination DAP data are available from the dose report compiled by the system.
We calculated the estimated dose using a PC-based x-ray Monte Carlo model programme—PCXMC vs2.20 The PCXMC simulator is based on the Cristy and Eckerman model and incorporates the new ICRP 103 tissue weightings.20 PCXMC allows a free adjustment of the x-ray beam projection and other examination conditions within projection radiography and fluoroscopy.
The DAP, the projection angle, the kV, the field size, the duration of exposure and the frames per second were recorded for each exposure acquisition along with the patients' height and weight; these data were programmed into the PCXMC simulator to calculate the exposure effective dose.
The study dose report produced by the Philips Allura FD10 equipment does not provide a specific record for screening during invasive angiography. While the total DAP for radiation dose associated with screening is recorded, assumptions had to be made for individual screening projections. As in previously published dosimetry7 calculations, the fluoroscopic field sizes, positions and angles used were assumed to be identical to the acquisition data. The percentage fluoroscopic DAP for each field was divided by the same proportions as the exposure. A quality assurance assessment of the kV for fluoroscopy demonstrated that this was approximately 12 above that for acquisition runs; therefore, fluoroscopic kV was assumed to be acquisition kV+12. Acquired runs and screening projections were modelled with the specific filtration employed by the system (screening had a higher level of beam hardening filtration than acquired runs).
These data were used with PCXMC to model the procedure and calculate the total effective dose for each of the 16 patients and derive our own hospital-specific conversion factor of 0.24 mSv/Gy cm2.
We then applied this conversion factor to a larger population of patients with the same BMI distribution, access route and indication for coronary angiography to calculate the effective dose for coronary angiography.
MDCT protocol
We studied consecutive patients presenting for cardiac CT as part of their usual clinical care; the same exclusion criteria used for the invasive coronary angiography cohort were employed, and only patients scanned with a prospective protocol with the smallest x-ray window were included.
All standard scans, with FBP, were performed on a Light Speed VCT scanner (GE Healthcare, Milwaukee, Wisconsin, USA) deploying commercially available techniques (snapshot pulse, GE Healthcare). If the baseline heart rate was >65 bpm, intravenous β-blockers were administered.
Patients were scanned with a prospective protocol, using the smallest x-ray window (padding over-ride set to 0). For CT coronary angiography (CTCA), 90 ml of Optiray 350 (Covidien,Dublin, Ireland) was administered via a cannula in the antecubital fossa at a rate of 6.5 ml/s reducing to 5.5 ml/s followed by 50 ml of N-saline. The scan area was set to start at the tracheal carina down to the inferior border of the heart using three to four 40 mm overlapping blocks depending on the patient's size.
The scan was triggered by the attending radiologist/cardiologist at the moment of maximal contrast opacification in the left side of the heart.
The scanner parameters 64×0.625 mm, the smallest x-ray window at 75% of the R-R interval, the z-coverage of 40 mm with an increment of 35 mm, gantry rotation time of 350 ms, and tube current and kV were adapted to the BMI.
Scans utilising iterative reconstruction were performed on an HD750 (GE Healthcare) using commercially available software; the first patients scanned as part of the clinical service were included in the study. The BMI distribution was greater than that for the GE VCT scanner (table 1). Exclusion criteria included a non-coronary indication for scanning, previous bypass grafting and a suspected acute coronary syndrome.
Patient demographics and scan parameters
The scanning parameters were similar to those used on the GE VCT scanner, but because of the use of iterative reconstruction, the mA was reduced.
CTCA radiation dose
For each individual patient, the effective dose for the CTCA was calculated using the imaging performance assessment of CT scanners (ImPACT) calculator. This is a computer-based anthropomorphic geometric phantom using the Monte Carlo-derived National Radiation Protection Board (NRPB), now part of the Health Protection Agency) data sets21 and is a well-validated method of calculating CT radiation dose.12 For an effective dose calculation, the ImPACT model requires the CTDIair (for the particular CT scanner), kV, mA and scanner filter. The CTDIair was measured with a 100-mm pencil ionisation chamber (Accupro; RadCal, Monrovia, California, USA), placed in the scanner bore across the range of filter/kV combinations typically used in clinical scanning. These results were applied to each patient's data set to calculate an individual's effective dose. The ImPACT calculator uses the latest ICRP 103 tissue weightings. No CT conversion factors were used to calculate the effective dose in this study.
Statistics
Quantitative variables were expressed as mean (SD), median with interquartile ranges (IQRs), and percentages. Mann–Whitney U tests were performed for the comparison of effective dose between the two groups. All analysis was performed on commercially available software (SPSS 17.0).
Results
Over a 6 month period, 94 invasive angiograms were available for review. The median effective dose was 6.3 mSv (IQR 4.2–8.2). The mean BMI was 27 (3.6), and the mean age was 66 (10) years; 67% were men.
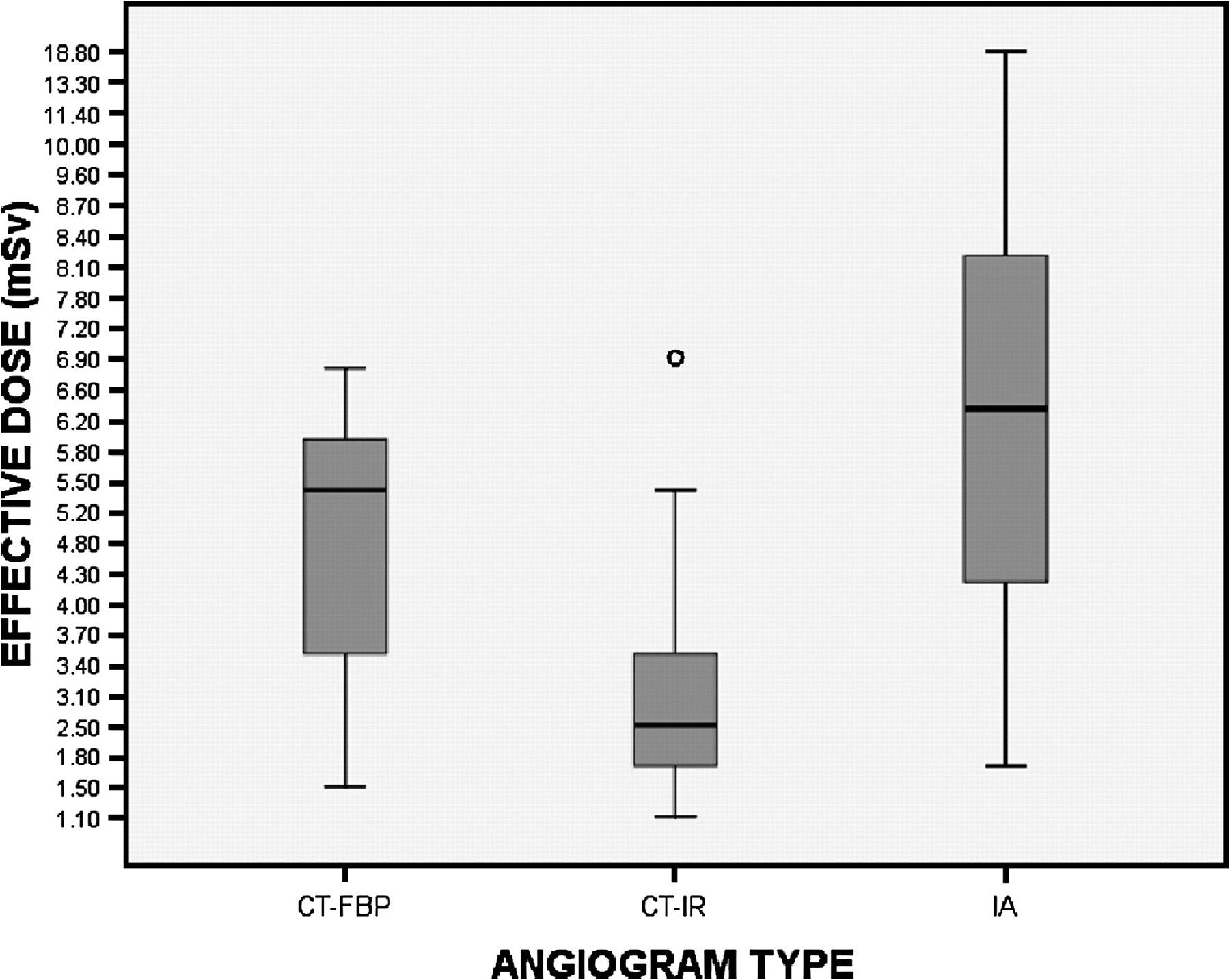
Over the same period, the details of 84 CTCA scans were interrogated. Each scan was assessed with the ImPACT calculator to derive an effective dose. The mean BMI was 27 (3.8), and the mean age was 59 (11) years; 62% were men. The median effective dose was 5.4 mSV (IQR 3.5–5.9). The calculated median effective dose was higher in the invasive angiography group compared with the CTCA group (p<0.001; figure 3). Following the instalment of the HD750 scanner, the first 39 patients scanned with iterative reconstruction were included in this study. The median effective dose of 2.5 mSv (IQR 1.6–3.5) was significantly lower (p<0.001) than the doses from cardiac CT with standard FBP and invasive angiography.

{kind=link}
{kind=link}
{kind=link}
Patient radiation dose in mSv according to angiographic type expressed as medians. Boxes: upper to lower quartile. Thin lines: maximum and minimum (excluding outliers and extreme values). CT-FBP, CT with filtered back-projections; CT-IR, CT with iterative reconstruction; IA, invasive angiography.
Discussion
CTCA has, over the last decade, developed from research to an invaluable clinical tool.22 23 Quite rightly, there have been concerns regarding the radiation exposure to the patients from the early multidetector scanners. Einstein et al24 estimated the lifetime risk of cancer to be as high as 1:143 for a 20-year-old woman if a scan was performed retrospectively with no dose modulation. The early studies, which used retrospective gating with no dose modulation, would regularly deliver a dose of >15 mSv.15 With the introduction of more slices per rotation, the radiation dose from cardiac CT increased7; however, with the use of dose saving algorithms, the effective dose from CTCA has been reported as <2 mSv.5
Differing imaging modalities deliver differing doses of radiation. The scanner-derived DLP and the catheterisation equipment-derived DAP do not allow comparisons between the two imaging methods. However, the calculation of effective dose (mSv) using a computer-based anthropomorphic model allows a comparison of the radiation doses. The calculation of the effective dose takes into account the biological effect of the radiation on a particular organ because each organ is given a tissue weighting depending on its individual susceptibility to the effects of ionising radiation.
The tissue weightings are derived from the ICRP, an international organisation founded in 1928, which now focuses on all aspects of protection from ionising radiation. In 2007, the ICRP released the 103 publication updating the 16-year-old ICRP 60 data set. The new tissue weightings are based on further epidemiological research compiled from studies of the Japan atomic bomb survivors and smaller medical, occupational and environmental studies.14
We used the latest data set from the ICRP 103 to calculate a conversion factor for the catheter laboratories at a university teaching hospital. Previous conversion factors for invasive coronary angiography have ranged6 17–19 from 0.12–0.26 mSv/Gy cm2. These are based on older ICRP data sets, although they are of the same magnitude as our own locally calculated conversion factor (0.24 mSv/Gy cm2).
The DAP for the invasive coronary angiography is similar to previously published17 18 levels (mean 27 Gy cm2) and are lower than the published national diagnostic reference levels25; therefore, the angiogram effective dose does not represent an artificially high level for comparison with cardiac CT.
As discussed, the previously published conversion factors for cardiac CT are based on a significantly larger scanning volume and the ICRP 60 tissue weightings. These two fundamental differences mean that, in our opinion, older conversion factors do not give an accurate assessment of the effective dose from modern multislice cardiac CT. When a chest conversion factor is used, the figure obtained is artificially low because it includes the relatively radio-resistant tissues of the upper chest. Cardiac CT is performed of the lower chest and typically contains almost the majority of the breast tissue, which is radiosensitive and therefore is under-represented with such an assumption.
Our data set for the cardiac CT scans is based not on a conversion factor but on an individually calculated dose from the ImPACT calculator using radiation data recorded from the scanner; these data included the radiation exposure measured from a variety of different scanner programmes.
Recently, two groups have published comparisons of effective dose between CTCA and invasive coronary angiography.6 26 While these papers use a head-to-head comparison design, the calculation of effective dose for cardiac CT was made using conversion factors based on the out-dated ICRP 60 tissue weightings for a chest CT scan rather than a cardiac CT scan. We, however, have calculated each patient's effective dose using a computer-based calculator employing dosimetric measurements taken from the scanner. Because of these differences in methodology, we feel that our estimation of effective dose for cardiac CT is the most accurate published to date. A chest CT conversion factor applied to our data set would result in a significant underestimation of the effective dose from cardiac CT to approximately half of the mean dose. The mean DLP derived from the scans utilising iterative reconstruction is 94 mGy cm; a conversion factor27 of 0.014 would give a dose estimation of 1.3 mSv, a significant under-estimation.
The cardiac CT data presented are derived from a GE VCT Lightspeed scanner with ECG prospective gating. This system is >3 years old. The technology behind cardiac CT is a rapidly developing field. The more modern scanner utilising iterative reconstruction techniques results in a significant reduction in effective dose.
The dose from cardiac CT is already low and is likely to reduce even further with advances in dose reduction technology; however, it is important that studies reporting radiation dose reduction techniques use a robust calculation method rather than a conversion factor based on out-dated ICRP tissue weightings and a scanning volume, which is not well reflected by cardiac CT and underestimates actual dose delivered.
Limitations
The effective dose calculations from the cardiac CT only take into account the radiation exposure from the main contrast--enhanced scan, not on the scout or unenhanced scans. Therefore, the effective dose for the complete CT examination will be marginally higher than those quoted. This method is in line with those of other publications,7 and the dose from the scout and unenhanced scan is minimal.
While the PCXMC simulator is flexible enough to include the size of the patient in the calculation of the effective dose, the ImPACT calculator is not. One of the inadequacies of the software, and all present research regarding CT radiation dose, is the lack of information regarding the relationship between the body habitus and the radiation dose the individual receives—an important factor in the prediction of dose during fluoroscopy.28
The two models (PCXMC and ImPACT) for the calculation of effective dose also have inherent faults. The degree of uncertainty in estimation of the effective dose for medical examination has been estimated10 up to ±40%; however, the dose audit methods from this study are in line with the National Protocol for Patient Dose Measurements in Diagnostic Radiology, and similar methods are used to populate the National Patient Dose Database (maintained by the Health Protection Agency), which has in part been utilised by the Department of Health to establish current national diagnostic reference levels in the UK.
The data collected from the audit will be specific for a prospectively gated scan performed on a GE Light Speed VCT/GE HD750 scanner. There are currently no mathematical CT simulations that enable accurate modelling of segmented radiation fields. For this study, radiation doses were calculated, assuming that the radiation dose per slice was averaged over a 360° rotation rather than a partial gantry rotation.
The invasive angiography conversion factor was based exclusively on radial rather than femoral access and therefore may not be comparable with that in studies of the femoral route.
Conclusions
The accuracy of coronary cardiac CT has been fully evaluated over the last 5 years and is now beyond doubt.13 22 23 With the advent of prospective gating, the doses from cardiac CT have significantly fallen. We have now demonstrated that despite the recent increase in ICRP tissue weightings and the use of the most accurate methods of dose estimation, the radiation dose from prospectively gated cardiac CT with standard FBP is comparable with the dose received from invasive coronary angiography; however, with the use of iterative reconstruction techniques, the effective dose is significantly lower than that received from invasive coronary angiography.
Acknowledgments
We would like to acknowledge the support and help of all the catheter laboratory and radiology staff at Derriford Hospital, Plymouth, and the continuing support of the Gawthorn Trust, Royal Devon and Exeter Hospital.
References
Footnotes
Competing interests Declared. GM-H and CR have received lecture fees from GE Healthcare.
Provenance and peer review Not commissioned; externally peer reviewed.