Article Text

Abstract
Background Exercise improves the clinical outcome of patients with coronary artery disease (CAD); however, the ideal exercise duration for each patient remains unclear.
Objective To investigate the effects of exercise duration on arterial elastic properties and antioxidant/pro-oxidant mechanisms in patients with CAD.
Design, setting, patients, interventions Sixty male patients with CAD were randomised into two groups, and underwent exercise for 30 min or 60 min in a crossover design with 2 weeks' wash-out period. In all participants aortic and radial blood pressures (BP) and arterial elastic properties (augmentation index (AIx)/pulse wave velocity (PWV)) were determined at baseline and 24 h after exercise. Plasma malonyldialdehyde (MDA) and superoxide dismutase (SOD)1 and SOD2 levels were also measured.
Results Exercise had no effect on aortic and radial BP (p=NS for all). Walking for 30min improved AIx (from 33.79±0.91% to 31.73±0.86%, p<0.001) and PWV (from 9.26±0.95m/s to 9.06± 0.21m/s, p<0.001), while exercise for 60min had adverse effects on vascular stiffness (for AIx: from 33.37± 0.93% to 33.73± 1.05%, p=NS and for PWV: from 9.25±0.19m/s to 9.37±0.21m/s, p<0.05 mainly in older patients). Exercise for 60min was associated with a significant 20% increase in MDA levels (p<0.05). Exercise had no effects on SOD1 levels, however it significantly increased SOD2 levels after 30min (from 2.26±0.22ng/mL to 2.36±0.18ng/mL, p<0.05) but not after 60min (p=NS).
Conclusion Shorter exercise duration was associated with favourable antioxidant and vascular effects, while longer exercise blunted these beneficial effects and was accompanied by adverse effects on vascular function, mainly in older coronary patients. Further studies are required to explore the hypothesis that a more individualised approach to the selection of the appropriate exercise programme should be considered for patients with CAD.
- Exercise
- coronary artery disease
- MDA
- superoxide dismutase
- augmentation index
- pulse wave velocity
- electrocardiography
- exercise testing
- exercise training
- atherosclerosis
- free radicals
Statistics from Altmetric.com
- Exercise
- coronary artery disease
- MDA
- superoxide dismutase
- augmentation index
- pulse wave velocity
- electrocardiography
- exercise testing
- exercise training
- atherosclerosis
- free radicals
Physical inactivity and a sedentary lifestyle are well-established risk factors for cardiovascular disease.1 Strong epidemiological, clinical and basic science data support regular exercise training in the primary and secondary prevention of atherosclerotic vascular disease.1 Regular exercise is associated with decreased morbidity and mortality both in the general population1 and in patients with coronary artery disease (CAD)2 and improved short-term3 and long-term prognosis4 after acute myocardial infarction. Indeed the protective effects of exercise on the cardiovascular system extend beyond traditional risk factors (blood pressure (BP) levels, lipids, glucose metabolism, obesity), including beneficial effects on endothelial function,5 arterial elastic properties,6 autonomic nervous system activity and inflammatory mechanisms.7
Although the exact mechanisms by which exercise improves clinical outcome are unclear, physical training cardioprotective properties are thought to be predominantly linked with favourable effects on redox homoeostasis. Single bouts of exercise increase production of reactive oxygen species, which is an apparently harmful process.8 Nevertheless, regular exercise training activates damage repair systems and upregulates antioxidant enzymes expression to counter-regulate oxidative burden.8 Furthermore, exercise-induced stress stimulates late ischaemic preconditioning of the myocardium9 and promotes overall beneficial redox adaptations.8
Current recommendations for secondary prevention of CAD suggest 30–60 min of moderate-intensity aerobic activity for all patients, such as brisk walking, on most, preferably all, days of the week.10 However, the ideal exercise duration needed to achieve the optimum benefit remains unclear. In addition, current recommendations do not clarify the ideal duration and intensity of exercise for specific patient groups—for example, some patients may receive maximum benefit with less than the recommended exercise duration, while others might be put at risk of ischaemia and sudden cardiac death with prolonged duration and increased intensity of exercise.11 Consequently, there is need for a more individualised and sophisticated approach to physical activity recommendations in patients with CAD.
The aim of this study was to investigate whether the duration of exercise has an impact on the response of antioxidant defence systems and systemic oxidative stress in patients with CAD. Moreover, we examined whether exercise duration has an impact on the responses of vascular elastic properties to acute exercise.
Methods
Study population and study design
All the participants were sedentary men, not taking part in any regular physical training in daily life, with angiographically documented stable CAD and a recent positive exercise treadmill test. Any patient with physical inability to exercise, decompensated heart failure, left ventricular ejection fraction <45%, arrhythmias, severe chronic obstructive pulmonary disease, any inflammatory disease, malignancies or receiving treatment with corticosteroids or anti-inflammatory drugs was also excluded from the study. The patients' demographic characteristics are shown in table 1.
Patients demographic characteristics
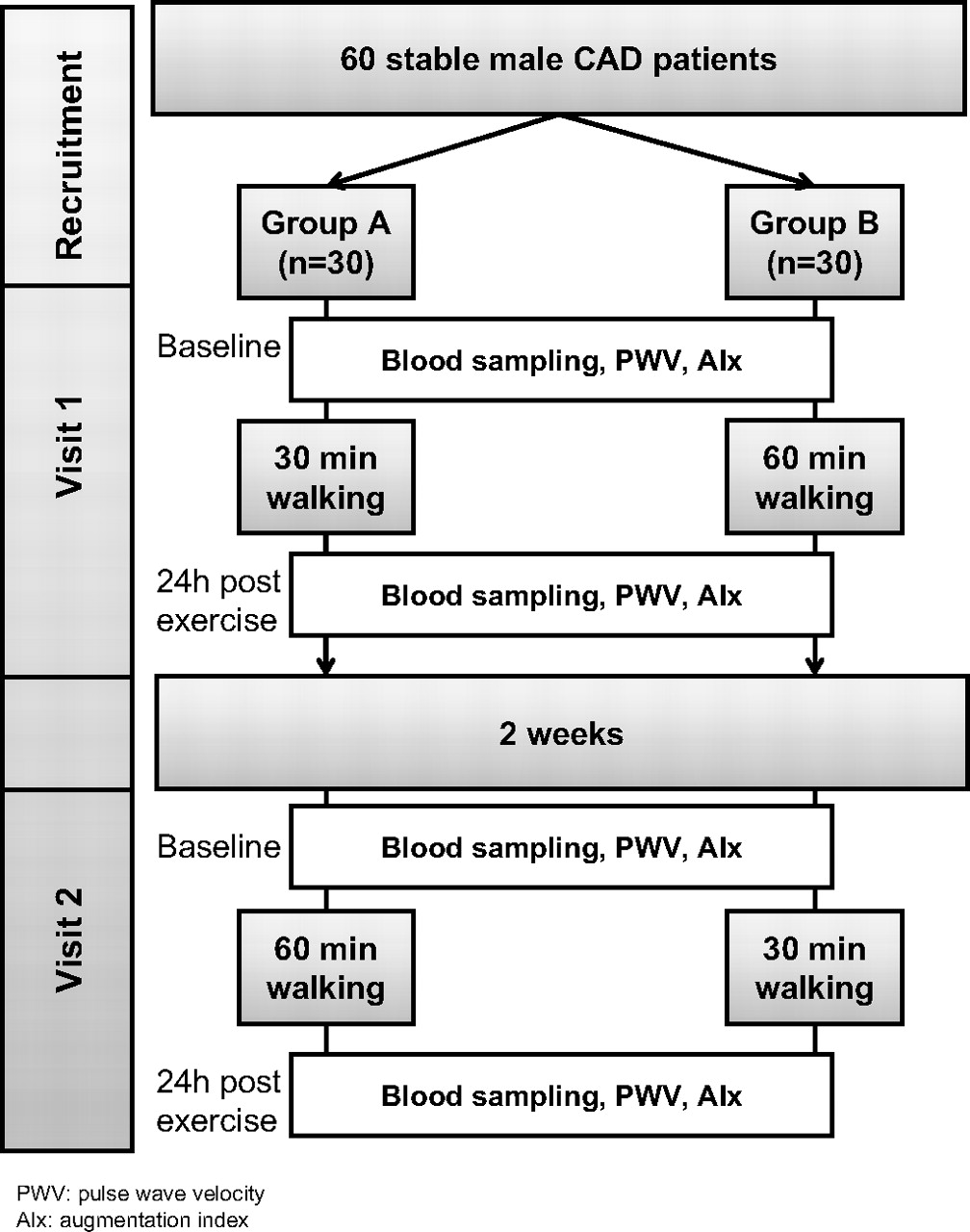
The study was performed in a cross-over design (figure 1). The study population consisted of 60 patients, randomised into two groups: group A (n=30) and group B (n=30). During the first visit group A exercised for 30 min, while group B exercised for 60 min. After a 2 week wash-out period, in a follow-up visit, group A exercised for 60 min, while group B for 30 min. Two weeks before each visit all participants received a standard exercise programme as recommended by the AHA/ACC guidelines10 and every participant was asked to stop any vasoactive agent, smoking and coffee consumption for at least 12 h and abstain from exercise or strenuous walking for at least 4 days before each visit. During each visit, all participants underwent blood sampling and evaluation of arterial elastic properties twice—before the exercise protocol and 24 h after exercise. Venous blood samples were centrifuged within 15 min after venepuncture at 3000 g at 4°C for 10 min and plasma was collected and stored at −80°C until assayed.
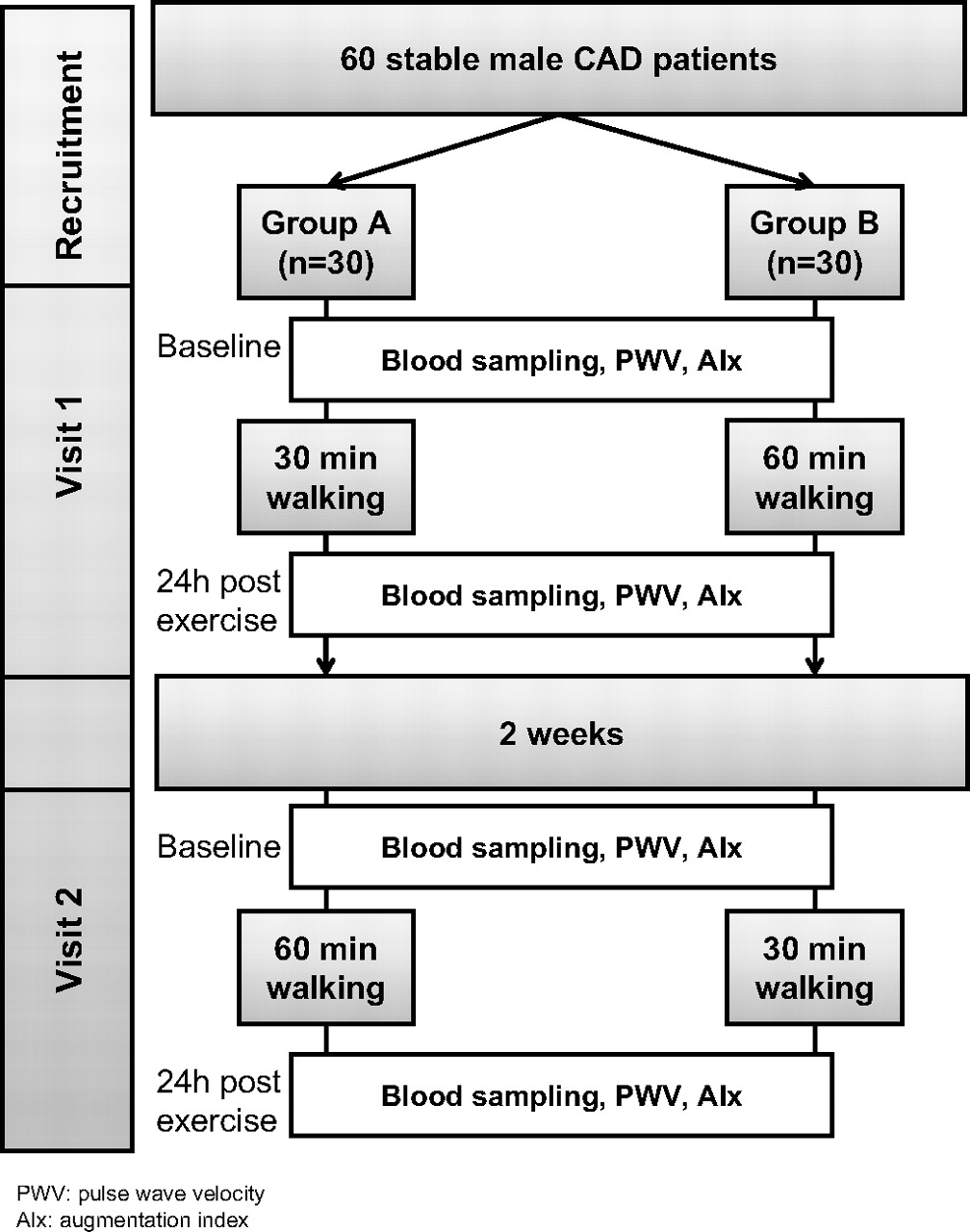
Study design. CAD, coronary artery disease.
Walking protocol
The walking protocol was performed on an exercise treadmill device (General Electric CASE T-2000, Freiburg, Germany) under continuous ECG monitoring and at zero degrees angle. In more detail, the walking protocol was designed as follows: (a) 30 min walking: 1.7 km/h for 2 min, 2.7 km/h for 3 min, 5 km/h for 20 min, 2.7 km/h for 3 min and 1.7 km/h for 2 min; (b) 60 min walking: 1.7 km/h for 2 min, 2.7 km/h for 3 min, 5 km/h for 50 min, 2.7 km/h for 3 min and 1.7 km/h for 2 min. During the treadmill exercise BP was determined at baseline and every 5 min by a brachial sphygmomanometer.
Determination of aortic and radial haemodynamics
Radial artery recordings were determined by using applanation tonometry (SphygmoCor, AtCor Medical, IL, USA). The central (aortic) arterial pressure was derived with the use of a generalised transfer function shown to give an accurate estimate of the central arterial pressure waveform and its characteristics. Waveforms of radial pressure were calibrated according to sphygmomanometric systolic and diastolic pressures measured in the brachial artery.
Evaluation of aortic elastic properties
Carotid-femoral pulse wave velocity (PWV), an established index of aortic stiffness was calculated from measurements of pulse transit time and the distance travelled between two recording sites with a validated non-invasive device (Complior, Artech Medical, Pantin, France). Two different pulse waves were obtained simultaneously at two sites (at the base of the neck for the common carotid and over the right femoral artery) with two transducers. Distance was defined as the distance from the suprasternic notch to the femoral artery minus the distance from the carotid artery to the suprasternic notch.
Measurement of wave reflection index
Augmentation index (AIx) of the central (aortic) pressure waveform was measured as an index of wave reflection. The AIx is defined as the augmented pressure divided by pulse pressure and is expressed as a percentage. Large values of AIx indicate increased wave reflection from the periphery and/or earlier return of the reflected wave as a result of increased PWV (owing to increased arterial stiffness) and vice versa. Because AIx is influenced by changes in heart rate, it was also corrected accordingly. AIx was measured with a validated, commercially available system (SphygmoCor, AtCor Medical).
Measurements of plasma malonyldialdehyde levels
Systemic lipid peroxidation was quantified by measuring malonyldialdehyde (MDA) levels in plasma. Briefly, blood samples were collected into tubes containing EDTA as anticoagulant, centrifuged and appropriately stored at −80°C until assayed. The determination of MDA was based upon its reaction with thiobarbituric acid. Briefly, 50 μl of plasma/standards was placed into tubes containing thiobarbituric acid dissolved in acetic acid. Samples were heated at 95–100°C for 1 h and thereafter they were cooled and subsequently, HCl and butanol were introduced into the mixture. After centrifugation at 3500 rpm for 10 min the butanol phase was removed. The fluorescence of the butanol extract was measured by a Perkin–Elmer fluorometer.
Measurements of levels of plasma superoxide dismutase isoforms 1 and 2
Systemic levels of superoxide isoforms 1 (SOD1) and 2 (SOD2) were measured in plasma by ELISA (LabFrontier Co, Ltd, Seoul, Korea).
Statistical analysis
All continuous variables were tested for normal distribution by the Kolmogorov–Smirnov test. Non-normally distributed variables were log-transformed for statistical analysis. Continuous variables between two independent groups were compared by an unpaired t-test. Continuous variables between two time points within each group were compared by a paired t-test. All variables are presented as means±SEM. All analyses were carried out by using the SPSS version 15.0 statistical package (SPSS Inc) and p<0.05 was considered statistically significant.
Results
Effects of exercise on haemodynamic profile
No patient exhibited electrocardiographic signs of ischaemia during the exercise protocol. Heart rate and brachial systolic BP (SBP) significantly increased during exercise for either 30 or 60 min (p<0.0001 compared with resting levels, table 2). Walking for 60 min was associated with significantly higher maximum heart rate during the exercise protocol than walking for 30 min (p=0.003). No difference was seen in maximum blood pressure levels between the two exercise protocols (table 2). However, during 60 min exercise older patients (age≥median) attained higher maximum BP levels (149.83±4.87 mm Hg vs 136.46±4.29 mm Hg, p<0.05) and achieved higher percentage levels of their maximum heart rate (76.5% vs 68.6%, p<0.05) than younger patients (age<median), while no differences were seen between the two age groups during walking for 30 min.
Exercise-induced changes in central and peripheral haemodynamics
Both aortic and radial SBP levels tended to decrease 24 h after walking for 30 min; however, this change did not reach statistical significance (SBP 24 h after walking for 30 min vs baseline levels: p=0.052 for aortic SBP and p=0.051 for radial SBP). No significant changes were seen in heart rate, radial SBP, aortic and radial diastolic blood pressure (DBP) and aortic and radial pulse pressure (PP) 24 h after walking for 30 min. Similarly, no significant changes were observed in heart rate and in either aortic or radial SBP, DBP and PP after walking for 60 min (table 2). Furthermore, there were no significant differences in aortic or radial BP changes after walking between the two types of exercise (30 min vs 60 min). In bivariate analysis aortic or radial BP changes were not associated with any demographic variable.
Effects of exercise on arterial elastic properties
Walking for 30 min induced a beneficial effect on arterial elastic properties, as both AIx and carotid-femoral PWV were significantly reduced 24 h after exercise compared with baseline levels. Walking for 60 min induced a significant increase in carotid-femoral PWV 24 h after exercise, while AIx increase remained unchanged (figure 2, panels A and B). Taken together, the changes in arterial elastic properties (AIx and PWV) were significantly different between the two types of exercise (figure 2, panels C and D). These findings indicate that exercise duration might differentially affect arterial elastic properties, with exercise prolongation above 30 min being associated with an adverse effect on arterial elastic properties.
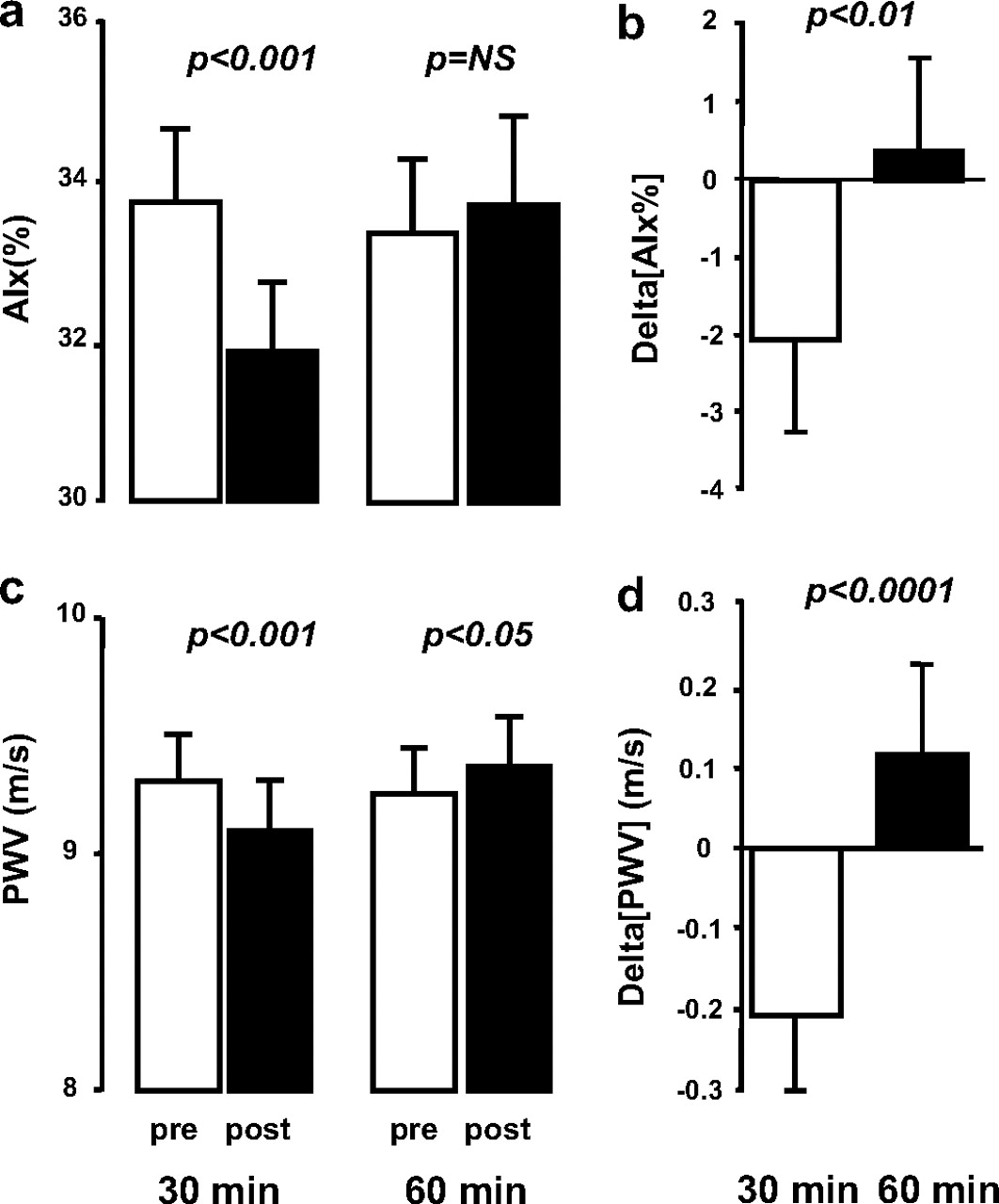
Exercise duration and arterial elastic properties. The change in augmentation index (AIx) 24 h after exercise for 30 min was significantly different from the AIx change after exercise for 60 min (panels A and B); similarly, the change in pulse wave velocity (PWV) 24 h after exercise for 30 min was significantly different from the PWV change after exercise for 60 min (panels C and D).
We then searched for other clinical predictors that might explain the differential effect of exercise duration on indices of arterial stiffness like AIx and PWV. Classic cardiovascular risk factors such as arterial hypertension, dyslipidaemia, smoking and obesity could not account for the differential effect of exercise duration on arterial elastic properties (p=NS for all).
Nevertheless, age was significantly associated with AIx changes after walking in bivariate analysis (r=0.399, p=0.002 for 30 min walking and r=0.36, p=0.007 for 60 min walking). Indeed, when the population was split into halves according to age median, 30 min walking still had a significantly beneficial effect on AIx but only in younger patients. On the contrary the adverse effects of 60 min walking on AIx were mainly driven by the negative effects observed only in the group of older coronary patients (figure 3, panel A). Furthermore, only older patients showed an improved PWV after 30 min walking, while there was no difference in PWV changes between the two age groups after 60 min walking (figure 3, panel B).
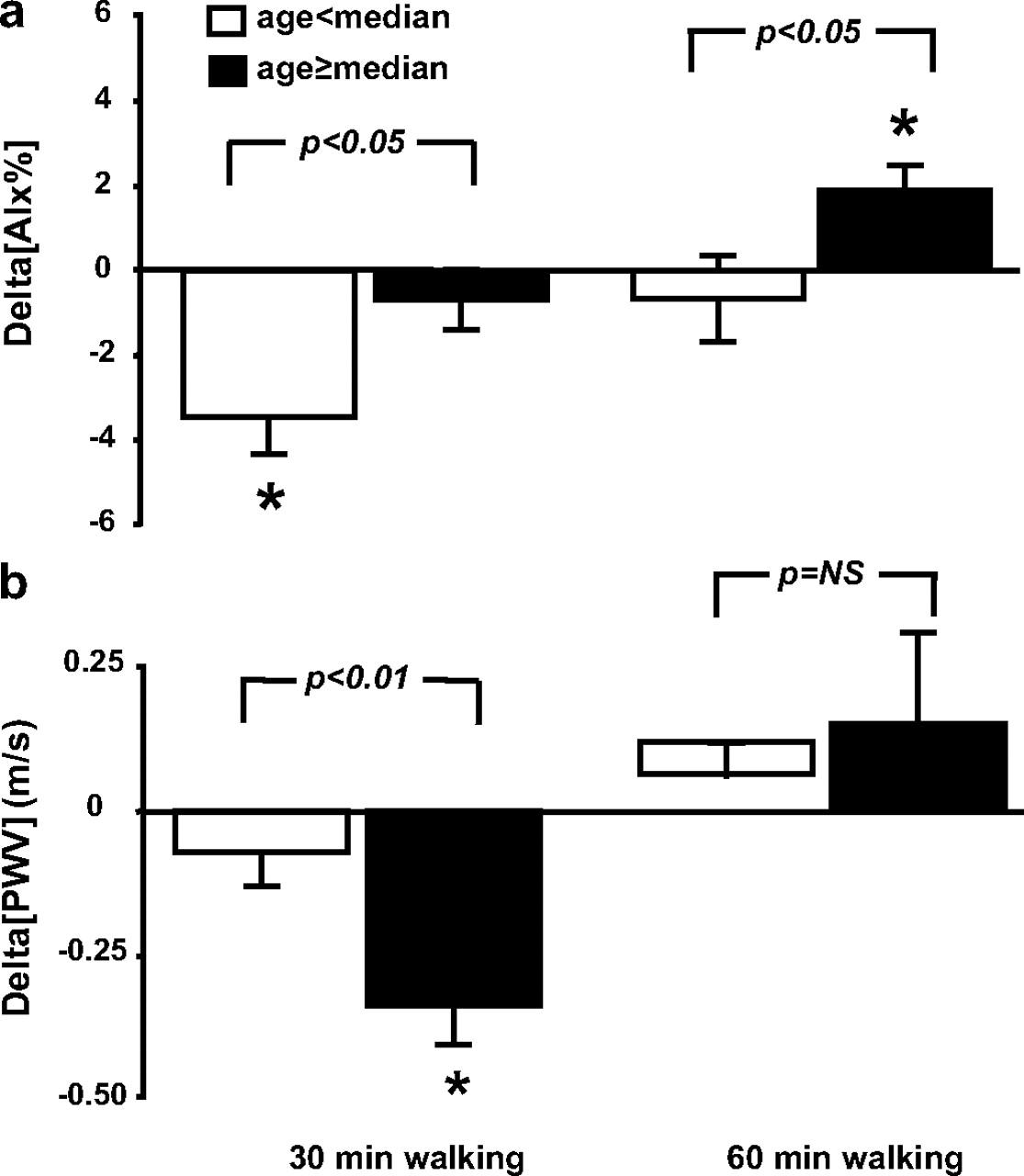
Exercise duration effects on augmentation index (AIx) according to age groups. The changes of AIx induced by exercise were significantly different between the age groups above and below the median, for both types of exercise. However, walking for 30 min induced a beneficial effect on AIx only in the group of younger patients (age< median, panel A). On the contrary, 60 min walking increased AIx only in older patients (age≥median, panel A). On the other hand, exercise for 30 min induced a significant reduction of pulse wave velocity (PWV) in older individuals while 60 min walking had a trend to increase PWV in these subjects (age≥median, panel B). *p<0.05 for the change before versus after exercise.
Finally, the maximum BP levels attained during exercise were significantly associated with carotid–femoral PWV 24 h after walking (for 30 min walking: 9.51±0.32 m/s vs 8.64±0.24 m/s for maximum BP ≥median vs maximum BP <median (p=0.039) and for 60 min walking: 9.85±0.29 m/s vs 8.83±0.27 m/s for maximum BP ≥median vs maximum BP <median (p=0.016)).
There was no association between the presence of hypertension or the angiographic extent of CAD, and the exercise-induced changes of PWV or AIx (data not shown).
Effects of exercise on oxidative stress and antioxidant defences
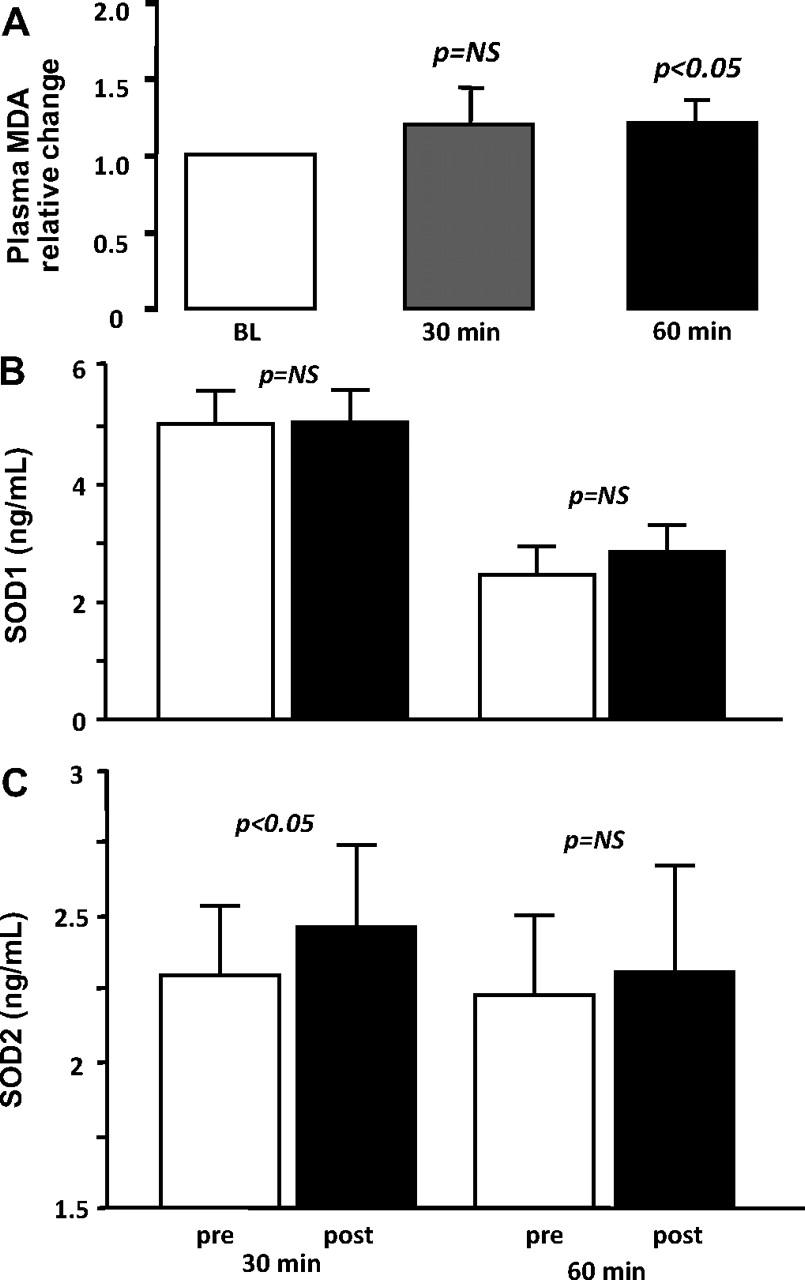
We then examined the effects of exercise on systemic oxidative stress, using MDA levels as a marker of systemic oxidative stress. Walking for 30 min had a borderline but not statistically significant impact on circulating plasma MDA levels (p=NS for MDA levels before and after walking for 30 min, figure 4, panel A). However, walking for 60 min, induced a significant 20% increase in plasma MDA compared with baseline levels (p=0.016, figure 4, panel A), although there was no statistically significant difference in MDA levels between 30 and 60 min, probably owing to the small study population. The change in plasma MDA levels was not associated with any demographic variable, haemodynamic parameter or arterial elastic property changes after walking for either 30 or 60 min (p=NS for all).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Exercise duration and systemic oxidative stress status. Walking for 30 min did not significantly alter plasma malonyldialdehyde (MDA) levels after exercise. However, walking for 60 min was associated with a significant 20% increase in plasma MDA levels from baseline. (B) Exercise duration and superoxide dismutase 1 (SOD1). SOD1 plasma levels remained unchanged after exercise for either 30 or 60 min. (C) Exercise duration and superoxide dismutase 2 (SOD2). SOD2 plasma levels were significantly increased after walking for 30 min while remained unchanged after exercise for 60 min.
Then we examined the effects of exercise duration on the antioxidant defence system, defined by the plasma levels of SOD1 and SOD2. We observed that systemic levels of SOD1 remained unchanged 24 h after walking for either 30 or 60 min (p=NS for both, figure 4, panel B). However, walking for 30 min had a favourable effect on systemic SOD2 levels (p<0.05), an effect not observed after 60 min of exercise (figure 4, panel B).
Importantly, the change in plasma MDA levels correlated significantly with the change in systemic SOD2 levels after 30 min walking (r=0.674, p=0.003). However, there was no association between the change in MDA levels and the change induced in SOD1 levels after 30 min walking (p=NS). Similarly, there was no association between the change in MDA levels and the change in SOD1 or SOD2 plasma levels after 60 min walking (p=NS for both).
There was no association between the presence of hypertension or the angiographic extent of coronary atherosclerosis and the exercise-induced changes of MDA, SOD1 or SOD2 (data not shown).
Discussion
In this study we demonstrated that 30 min of exercise is associated with enhanced antioxidant capacity (owing to a rapid activation of antioxidant defence systems such as SOD2), which is also accompanied by an improvement of arterial elastic properties. On the contrary, exercise prolongation for as long as 60 min, induced higher systemic oxidative stress and had overall negative effects on vascular stiffness 24 h after exercise. Importantly, the deterioration of vascular elastic properties after prolonged exercise was more pronounced in older coronary patients.
Despite the lack of large randomised clinical trials, epidemiological data and clinical studies have well documented the beneficial effects of exercise in patients with CAD.1 Regular exercise promotes weight reduction, improves cardiorespiratory fitness, arterial blood pressure levels, lipidaemic profile, glucose metabolism and systemic inflammation. These beneficial effects on classic cardiovascular risk markers have an overall positive effect on life expectancy and clinical outcome of patients with CAD.2–4 However, the exact mechanisms by which exercise improves clinical outcome are still unclear. Furthermore, the ideal duration of exercise for each individual patient remains unknown.
Evidence suggests that both regular and acute exercise improve endothelial function and vascular stiffness, with these changes being reversed after exercise cessation.12 13 Exercise training in spontaneously hypertensive rats improves acetylcholine-dependent vasodilatation.14 In humans acute moderate-intensity exercise improves endothelial function,15 while more intense exercise is associated with a transient decrease in endothelial function immediately after exercise.16 These findings imply that a cut-off point of exercise intensity may exist, beyond which exercise loses its beneficial impact on vascular endothelium and may have detrimental effects.
Evidence suggests that acute exercise is not associated with any changes in arterial elastic properties immediately after exercise in healthy individuals.17 Nevertheless low-intensity treadmill exercise for even 10 min improves vascular stiffness indices in patients with CAD.18 On the contrary, the beneficial effects of regular moderate-intensity exercise on vascular stiffness are better documented. Regular exercise training is associated with beneficial effects on arterial elastic properties in various populations such as elderly subjects19 and individuals at high cardiovascular risk.20
Despite these well-documented beneficial effects of exercise on vascular function, it is unclear whether the duration of exercise has any impact on these effects. The presence of a threshold in exercise intensity/duration beyond which exercise loses its beneficial properties and may even cause vascular damage, is likely. In this study we demonstrate for the first time that walking for 30 min is associated with beneficial effects on arterial elastic properties in almost all patients with CAD. On the contrary, exercise duration prolongation for as long as 60 min in coronary patients adversely affects vascular stiffness, especially in older coronary patients. This finding suggests that the duration of exercise may be a critical parameter determining its effects on vascular structure/function, and the cut-off point could be individualised based on a patient's clinical characteristics.
It is well established that single bouts of exercise increase systemic oxidative stress. High-intensity exercise in healthy men21 is associated with significant increases in circulating MDA levels after exercise. However, regular exercise induces favourable redox adaptations that reduce systemic oxidative stress and upregulate antioxidant defence mechanisms. Previous studies in animals have demonstrated that chronic exercise attenuates peroxidation of lipids after acute exercise,22 and upregulates superoxide dismutase mRNA levels in coronary arterioles.23 Previous epidemiological studies on humans have demonstrated that circulating levels of oxidative stress markers, particularly MDA, are significantly lower in trained subjects than in sedentary individuals.24 Furthermore, regular exercise in older men decreases resting and after-exercise MDA levels and increases resting and after-exercise total antioxidant capacity and glutathione peroxidase levels,25 effects which are reversed with detraining.25
As we have demonstrated in the past, sequential episodes of exercise-induced myocardial ischaemia in middle-aged men upregulate extracellular SOD levels.26 Furthermore, in patients with established CAD, regular exercise for 12 weeks increased plasma SOD levels and decreased plasma 8-isoprostane-F2α levels, an oxidative stress marker.27 However, the effects of acute exercise on SOD isoforms remain obscure. Evidence suggests that exercise induces differential effects on the various SOD isoforms, which are indeed exercise intensity-dependent. While low-intensity exercise upregulates SOD1, higher exercise intensity tends to decrease SOD1 and to significantly increase SOD2 activity.28 Furthermore, in trained individuals, acute exercise has no effect on SOD1 but it increases SOD2 by 34%,29 while a single bout of exercise significantly decreases SOD1 levels 15 min and 24 h after exercise in young untrained men, without any effects on SOD2 levels.30
In agreement with these previous reports, we demonstrated in our cohort of male coronary patients that exercise duration has differential effects on circulating SOD isoforms. Lower exercise duration significantly increased SOD2 levels 24 h after exercise and had no effects on SOD1, while, on the other hand, longer exercise duration had no significant effects on both SOD isoforms, but was associated with a small but significant 20% increase in MDA plasma levels.
It should be noted that in this study, only simplified methods for assessing systemic pro-oxidant/antioxidant balance status were used (circulating MDA and SOD1/2). This limitation may explain the rather weak changes in circulating MDA and SOD2 after exercise, which are, however, accompanied by a striking effect on AIx and PWV, both measures of vascular function that can be highly affected by changes in vascular redox state. Unfortunately, there is no valid method of monitoring the vascular redox state in humans not undergoing surgery, other than indirect measurement of circulating oxidative stress markers. Furthermore, the clinical significance of these biochemical measures in systemic circulation remains unclear, while it is unknown whether changes in circulating oxidative stress markers are linked with changes of the complex pro-oxidant/antioxidant enzymatic systems regulating the vascular redox state in humans. In addition, the effect of age as a regulator of these responses of vascular function to exercise is based on a post hoc analysis of our results and it is, rather, hypothesis generating, therefore further studies designed specifically to examine this point are required.
In conclusion, this study suggests that shorter exercise duration (30 min instead of 60 min) leads to lower systemic oxidative stress status that is accompanied by an improvement of vascular mechanics in sedentary, particularly older, patients with CAD. If these novel, hypothesis-generating findings are confirmed by larger randomised clinical studies, they may have a significant impact on the clinical management of these patients.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Hippokration Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.