Article Text

Abstract
Background Cardiovascular co-morbidities are common in chronic obstructive pulmonary disease (COPD). Retrospective studies on selected patients have indicated that cardiac troponin elevation is frequent during acute exacerbations of COPD (AECOPD), and that this is associated with poor survival. In the present prospective study the prevalence and prognostic value of elevated cardiac troponin T (cTnT) in unselected patients with AECOPD have been investigated, using a novel high-sensitivity assay (hs-cTnT assay).
Methods and results 99 patients hospitalised for AECOPD were included. They were followed until death or study termination. During a median follow-up time of 1.9 years, 57 patients (58%) died. 97 patients (98%) had measurable levels of hs-cTnT and 73 (74%) had hs-cTnT above the normal range (≥14.0 ng/l). The crude mortality rates in patients having hs-cTnT <14.0, 14.0–39.9 and ≥40 ng/l were 4.6, 30.2 and 58.3 per 100 patient-years, respectively. Adjusting for relevant covariables using an extended Cox regression analysis, the HRs (95% CI) for death were 4.5 (1.2 to 16) and 8.9 (2.4 to 32) among patients having hs-cTnT 14.0–39.9 and ≥40 ng/l, respectively, compared with patients with hs-cTnT <14.0 ng/l. The association between mortality and hs-cTnT was strongly modified by heart rate at admission (p<0.001)—that is, the association between mortality and hs-cTnT was stronger among patients with tachycardia.
Conclusion Elevated hs-cTnT during AECOPD is frequent, and it is associated with increased mortality. The effect is stronger among patients having tachycardia than among patients with normal heart rate.
- COPD
- troponin
- mortality
- COPD epidemiology
- COPD exacerbations
Statistics from Altmetric.com
Key messages
What is the key question?
Is Acute Exacerbation of COPD (AECOPD) associated with myocardial injury, and is myocardial injury in this setting associated with long-term mortality?
What is the bottom line?
Using a highly sensitive troponin T assay, myocardial injury is detected in the majority of patients with AECOPD, and troponin elevation is independently associated with death in this setting.
Why read on?
The high prevalence and major clinical impact of even modest troponin elevation in this group suggest that myocardial injury in COPD is an issue that merits increasing attention.
Background
During the course of the disease, patients with chronic obstructive pulmonary disease (COPD) may experience acute exacerbations (AECOPD). The prevalence of COPD is reported to be from 6% to 25%.1 Using the GOLD (Global Initiative for Chronic Obstructive Lung Disease) criteria, a prevalence of 7% was found in a Norwegian population.2 Co-morbidities including osteoporosis, depression, weight loss, anaemia, lung cancer and cardiovascular disease (CVD) are frequent.1
Smoking is the leading risk factor for COPD. It is also a major risk factor for the development of CVD. Additionally, hypoxaemia, oxidative stress and systemic inflammation are assumed to contribute to the development of atherosclerosis in COPD.3 CVD is more common among patients with COPD than in the general population.4–8 In TORCH and the Lung Health Study, 26% and 25% of deaths, respectively, were from CVD.9 10 Epidemiological studies have indicated that patients with COPD more often are hospitalised and die from CVD than from their lung disease.5 11 In spite of this, autopsy material and ECG analysis indicate that myocardial infarction (MI) in patients with COPD often remains undiagnosed.12 13
Detection of myocardial damage, as measured by elevated levels of cardiac-specific troponin T and I (cTnT and cTnI), is a cornerstone in the diagnosis of MI.14 However, a range of cardiac and non-cardiac conditions may all lead to elevated troponin.15 16 Elevated levels of troponin are associated with increased mortality in pulmonary embolism, renal failure, ischaemic stroke and sepsis.15 16 With the evolution of a new, highly sensitive assay for measurement of cTnT (hs-cTnT assay), the detection level has been moved down to 3.0 ng/l.17 It has been shown that 98% of patients with coronary artery disease have measurable levels of hs-cTnT, even in a stable state, and that even marginal elevation, at levels below what was previously detectable, is associated with increased mortality.18
In retrospective studies of patients hospitalised for AECOPD using conventional troponin assays, 18–70% had elevated troponin levels,19–22 and troponin elevation in this setting has been associated with worse prognosis.19 21–23 Because of the retrospective design of these studies, troponin was only available in selected patients. We therefore included patients with AECOPD prospectively with the objective to assess the distribution of troponin levels, using a highly sensitive assay. Further, we wanted to assess the association between troponin and mortality while controlling for relevant confounders.
Methods
Patients were included from 3 January 2005 to 30 November 2006 and followed until 31 December 2008 or death. All patients admitted with assumed AECOPD were eligible for preliminary inclusion in the emergency room, prior to the emergency physicians' knowledge of any blood tests. The research fellow contacted the patient on the ward within a day to retrieve written informed consent and medical history. Exclusion criteria were: age <50 years, metastatic cancer and ECOG (Eastern Cooperative Oncology Group) performance status grade ≥2, neuromuscular disease with respiratory failure and non-cooperability. The diagnosis, as defined by the British Thoracic Society in 2004,24 was later verified by two study doctors by independent review of the hospital records, blinded for the result of the troponin analysis. In case of disagreement, the diagnosis was settled by consensus. Mortality data were gathered from the National Population Registry.
The following data were recorded in the emergency room: heart rate, blood pressure (BP), body temperature, respiratory rate, arterial blood gas (pH, Paco2, Pao2), arterial oxygen saturation (Sao2), use of accessory respiratory muscles, wheezing and chest pain. Mean arterial pressure (MAP) was estimated by the formula MAP=1/3×systolic BP + 2/3×diastolic BP.
Serum and plasma from blood drawn on admission was stored at −80°C for subsequent analysis of creatinine and hs-cTnT (cobas e 411 immunoanalyser, Roche Diagnostics, Mannheim, Germany). The lower limit of detection of hs-cTnT is 3.0 ng/l, and the 99th percentile in healthy volunteers was 14 ng/l. The lowest level with 10% coefficient of variation was 13 ng/l. Haemoglobin (Hb), leucocytes, platelets, electrolytes, and C-reactive protein (CRP) were collected from the hospital records. Chest radiographs were subsequently examined by two study doctors blinded for clinical data. The presence or absence of cephalisation (a composite of Kerley B-lines, enlarged vessels in the lung apex and interstitial or perihilar oedema), pneumonic infiltrates, pleural effusion, the size of the heart and the thoracic cavity in the frontal plane were recorded.
Spirometry during the stable phase was recorded when available. Postbronchodilatation measurements from the chest outpatient clinic prior to inclusion were preferred. Body mass index (BMI) was calculated from body weight and height as recorded on the spirometry report. Patients were categorised as current, former (>1 year abstinence) or never smokers.
In a pilot study of 29 consecutive patients with AECOPD, seven (24%) had elevated cTnT (≥0.04 μg/l). During 10 months follow-up, six of these (86%) died compared with two of the patients (9%) with normal cTnT. Assuming a mortality of 43% in patients with elevated cTnT (ie, allowing for 50% improved survival), unchanged mortality among the remaining patients, α =0.05, and that the prevalence of elevated cTnT is 25%, 104 patients would be required to achieve 90% power to detect a significant association between mortality and cTnT.
The study was approved by the Data Inspectorate, and reviewed by the Regional Committee for Research Ethics.
Statistical analyses
Hs-cTnT levels were categorised into three groups: <14.0, 14.0–39.9 and ≥40 ng/l. First, univariable associations between hs-cTnT and covariables at inclusion were investigated using χ2 test for categorical covariables and Kruskall–Wallis test for continuous variables. Secondly, if the association between the covariable and hs-cTnT in the univariable analysis had a p value <0.2, an age-adjusted log-rank test regarding mortality was performed. Thirdly, if the age-adjusted log-rank test for mortality revealed a p value <0.2, the corresponding association between the covariable and hs-cTnT was tested for homogeneity using Mantel–Haenszel test. Fourthly, if the log-rank test revealed a p value <0.2 the covariable was included in an initial multivariable extended Cox model. If the Mantel–Haenszel test revealed a p value <0.05 for homogeneity, the corresponding interaction term between hs-cTnT and the covariable was included in the initial multivariable model. If this interaction term confirmed the significance (p<0.05) of the bivariable homogeneity test, the covariable was considered an effect modifier, and the remaining multivariable analyses were stratified accordingly. The models were then reduced using backward elimination. If the association between a covariable and mortality had a p value >0.05 and removal of the covariable changed the estimate of the coefficient between hs-cTnT and mortality by <20%, it was removed from the model. We also performed the regression analysis ignoring any interaction term.
In the survival analyses, we used time-dependent covariables in an extended Cox model.25 In these models, time is counted until death or censoring, while variables that may vary between admissions are updated at each admission. To assess the differential effect of using time-dependent covariables (model 1) versus standard Cox regression, we also performed an analysis based on data recorded at baseline only (model 2) and compared the two models using the likelihood ratio test.
Univariable associations between hs-cTnT and the following variables were investigated: gender, age, forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio, FEV1, BMI, history of coronary artery disease, heart failure, hypertension and diabetes, smoking status, BP, heart rate, atrial fibrillation, peripheral oedema, chest pain, cephalisation or infiltrates on chest radiograph, Hb, CRP, leucocyte count, creatinine, pH, Paco2, Pao2 and Sao2. Continuous covariables having p <0.2 in the univariable analyses were dichotomised in the stratified analyses: BMI at 20 kg/m2, heart rate at 100/min, Hb at 13 g/l in males and 12 g/l in females, CRP at 50 mg/l, leucocytes at 10×109/l, creatinine at 100 μmol/l, Paco2 at 6.3 kPa, Paco2 at 7.0 kPa and Sao2 at 90%. Age was categorised into three groups: <65 years, 65–74 years and ≥75 years.
In model 2, the proportional hazards assumption was checked using the Schoenfeld residuals. The survival analyses were done using STATA 10 (StataCorp). The remaining analyses were done using SAS 9.1.3 (SAS Institute).
Results
On admission, data were obtained from 234 patients admitted with assumed AECOPD. Out of these, 114 were not included either because the research fellow was absent or because he had not been informed of the patients' arrival. Of the remaining 120 patients, nine failed to fulfil study entry criteria, leaving 111 consenting patients. Nine patients were excluded as review of their spirometry showed that they did not have COPD. Three patients with COPD were excluded as the primary cause of hospitalisation was pulmonary embolism or pneumothorax, leaving 99 patients for analysis. During the inclusion period, 47 previously included patients were readmitted with verified AECOPD, a total of 191 readmissions. In 120 of these, clinical data were recorded and blood was drawn on admission; thus data from 219 admissions were available for analysis. Median time from spirometry (n=88) to inclusion was 179 days (IQR 11–416 days). The stable phase includes both before (maximum 1250 days) and after (maximum 341 days) inclusion.
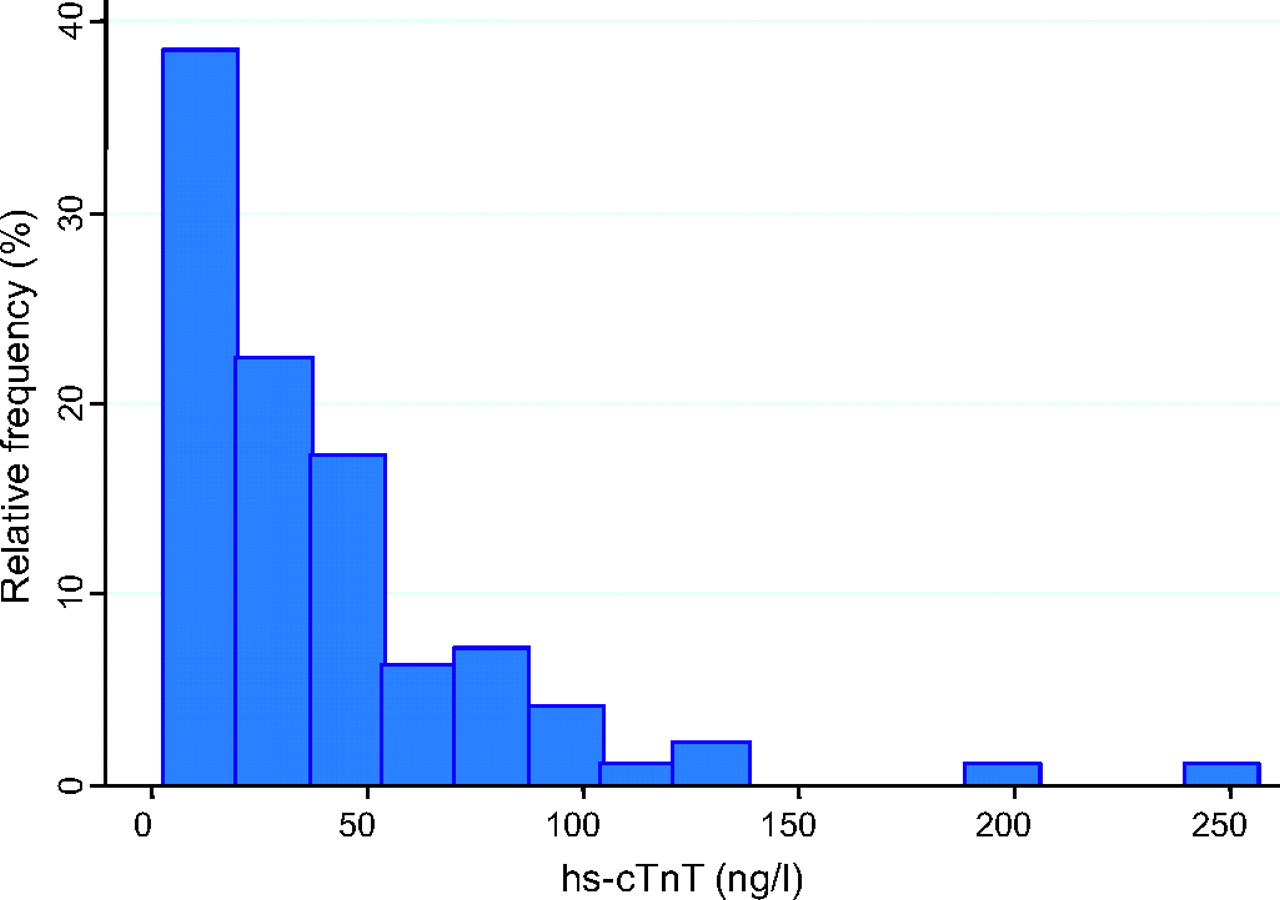
Median hs-cTnT at inclusion was 27.0 ng/l (IQR 13.4–51.0). The prevalence of patients having hs-cTnT <14.0, 14.0–39.9 and ≥40 ng/l was 26.3, 37.4 and 36.4%, respectively. The distribution of hs-cTnT at inclusion is displayed in figure 1. Of all 219 samples, two (0.9%) had hs-cTnT below the detection limit. The median observation time was 1.9 years. Mean age at inclusion was 71.5 years (SD 9.0), and 47 (47%) were female. Fifty-seven patients (58%) died during follow-up, and median survival time was 2.3 years. The crude mortality rates per 100 patient-years (95% CI in parentheses) were 4.6 (1.5 to 14.2), 30.2 (20.3 to 45.1) and 58.3 (40.8 to 83.4) in patients having hs-cTnT <14.0, 14.0–39.9 and ≥40 ng/l, respectively. Median survival time in patients having hs-cTnT 14.0–39.9 and ≥40 ng/l was 2.4 and 1.1 years, respectively. Among patients having hs-cTnT <14.0 ng/l, 89% survived the follow-up period (figure 2).
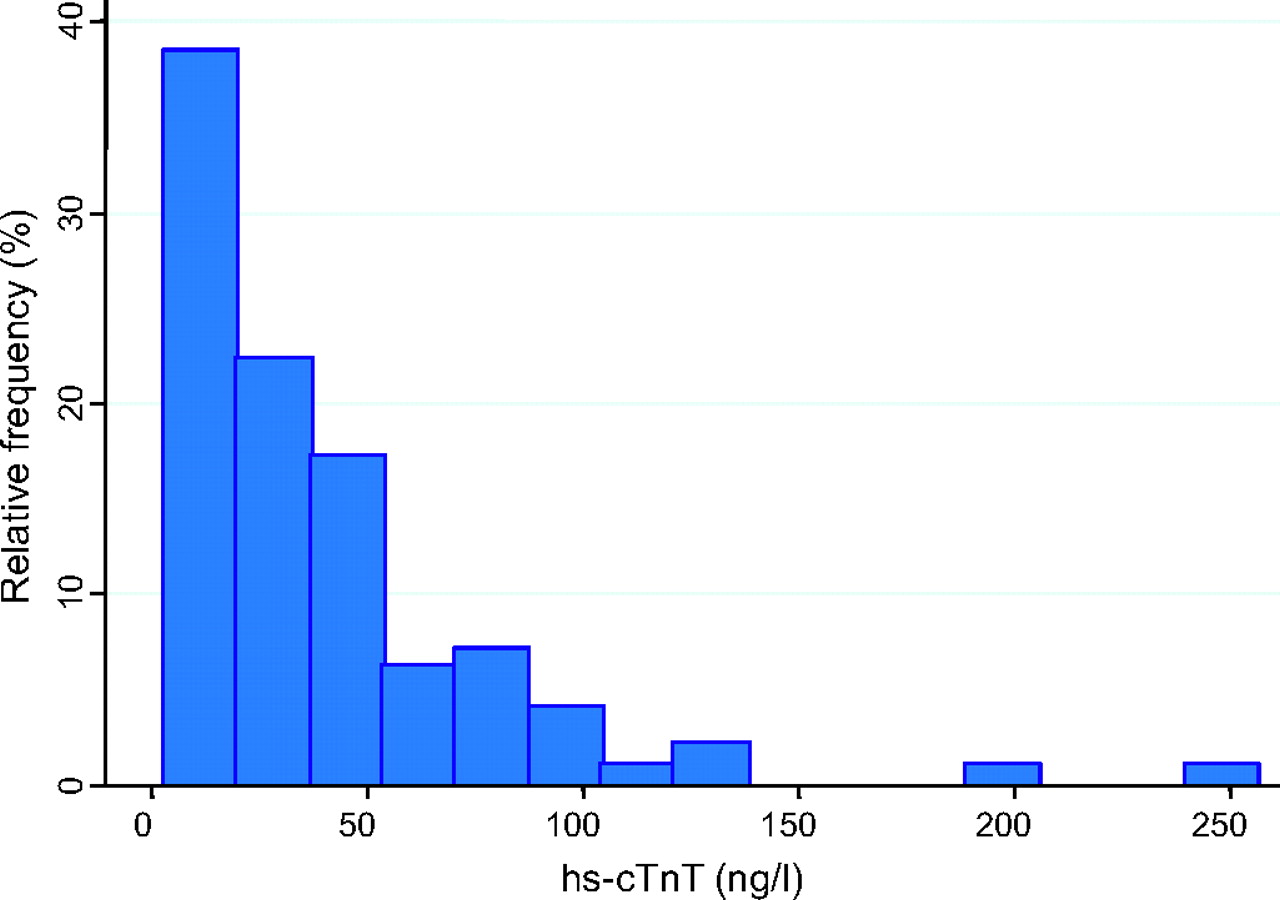
Distribution of high-sensitivity cardiac troponin T (hs-cTnT) in 99 patients with acute exacerbations of chronic obstructive pulmonary disease. The figure is based on each patient's index admission.

Survival after admission for acute exacerbations of chronic obstructive pulmonary disease by level of high-sensitivity cardiac troponin T (hs-cTnT), n=99. The figure is based on 219 admissions among 99 patients as explained in the text.
During the index admissions, no patients were diagnosed with heart failure. Two patients received a diagnosis of heart failure during subsequent admissions (hs-cTnT 18 and 71). Both patients died. One patient (hs-cTnT 133) received a discharge diagnosis of an acute coronary syndrome (ACS) during the index hospitalisation. Four patients received the diagnosis of ACS during subsequent admissions. All five patients survived. Of the 11 patients who did not have spirometry available, eight died during follow-up.
Univariable analyses between hs-cTnT and covariables revealed p values <0.2 for the following covariables (table 1): gender, age, history of heart failure and hypertension, heart rate, cephalisation, pulmonary infiltrate, leucocyte count, creatinine, Paco2, Pao2 and Sao2. BMI as a continuous variable showed no significant association with hs-cTnT, but analysis of the association between BMI <20 kg/m2 and hs-cTnT revealed a p value of 0.059. Hence, BMI was included in the age-adjusted survival analyses.
The distribution of high-sensitivity troponin T by relevant covariables in 99 patients hospitalised for acute exacerbation of chronic obstructive pulmonary disease
Table 2 shows the number of deaths and mortality rates in the three levels of hs-cTnT stratified by the covariables that were associated with hs-cTnT at inclusion (p<0.2).
Mortality (m), mortality rate/100 years (MR), mortality rate ratio (MRR) expressed as score test for trend for a one unit increase in troponin category, by selected covariables (explained in the text)
The mortality rate ratio (MRR) between each level of hs-cTnT is given as crude MRR as well as MRR adjusted for the corresponding covariable. Overall, the crude MRR between each level of hs-cTnT was 2.5 (95% CI 1.8 to 3.5). The bivariable analyses indicated that the adjusted MRR did not deviate much from the unadjusted value. Thus, there was no meaningful confounding in the data regarding mortality. However, the bivariable analyses indicated that the association between hs-cTnT and mortality was modified by heart rate (dichotomised at 100/min, p=0.010). Other categorisations of both hs-cTnT and heart rate were performed, but the test for homogeneity remained significant. The interaction term between heart rate and hs-cTnT also remained significant (p=0.029) in the initial extended Cox model. The association between hs-cTnT and mortality in patients having a heart rate of <100/min and a heart rate of ≥100/min is shown in figure 3A,B, also indicating that the association between hs-cTnT and mortality is much stronger in patients with tachycardia.

{kind=link}
{kind=link}
{kind=link}
(A) Survival after admission for acute exacerbations of chronic obstructive pulmonary disease (AECOPD) by level of high-sensitivity cardiac troponin T (hs-cTnT) in patients with heart rate <100/min. The figure is based on 219 admissions among 99 patients as explained in the text. (B) Survival after admission for AECOPD by level of hs-cTnT in patients with heart rate ≥100/min. The figure is based on 219 admissions among 99 patients as explained in the text.
Using the criteria for model selection outlined above, age, sex and cephalisation were included in the final model. In patients with tachycardia we found a strong association between hs-cTnT and mortality (p trend <0.001). In patients with a heart rate <100/min the association between hs-cTnT and mortality was not significant (p trend=0.250). The associations between mortality and sex, age and cephalisation were about the same in each model (table 3).
HR for death and the corresponding 95% CI among patients hospitalised for acute exacerbations of chronic obstructive pulmonary disease by selected covariables
Using model 2, we found no evidence of interaction between heart rate and hs-cTnT, thus the multivariable analysis was performed without stratification. The results obtained by using models 1 and 2 are compared in table 4.
HR for death and the corresponding 95% CI among patients hospitalised for acute exacerbations of chronic obstructive pulmonary disease by selected covariables
The difference in the log-likelihood statistics was 36.3—that is, a highly significant difference favouring the extended model. Finally, when using both the first and last hs-cTnT observation in the same Cox model, the association between mortality and baseline hs-cTnT became non-significant (p=0.313), whereas the association with the last observed value remained highly significant (p=0.001).
Model 2 did not violate the proportional hazards assumption.
At inclusion, the proportion of patients on β-blockers was 35% (heart rate <100/min) versus 20% (heart rate ≥100/min), p=0.099. The corresponding proportion of patients on calcium blockers with cardiac effects (ie, Verapamil, Diltiazem) was 13% versus 6% (p=0.279).
Discussion
This is the first study to prospectively measure hs-cTnT in an unselected cohort of patients with AECOPD, and to analyse the association between hs-cTnT and mortality after AECOPD. We found that hs-cTnT was measurable in 99.1% of the blood samples. Moreover, we found that even minor elevation of hs-cTnT was an important determinant of mortality. In patients with both elevated hs-cTnT and tachycardia, the prognosis was particularly poor.
At least four mechanisms should be considered when explaining troponin elevation in AECOPD: first, increased pressure in the pulmonary circulation leads to increased right ventricle afterload, which may promote cardiomyocyte damage or death. AECOPD due to concomitant pulmonary embolism may be included in this category. Secondly, a considerable proportion of patients with COPD may have undiagnosed coronary heart disease and suffer a type 1 MI.12 13 Thirdly, patients with COPD may have left heart failure accompanied by troponin elevation, and exacerbation of their heart failure may trigger an AECOPD. Fourthly, hypoxia and tachycardia may result in imbalance between oxygen demand and delivery, causing a type 2 MI.
Previous studies have indicated that elevated troponin during AECOPD is associated with poor outcome.19 21–23 However, these studies are hampered by methodological concerns that make generalisation difficult. One of the studies had a prospective design,19 but the study population were patients in intensive care units, hardly representative for the general AECOPD population. The three studies on the general AECOPD population were all retrospective, with troponin measured in selected groups (16, 44 and 73% of patients), and the possibility of selection bias arises, as discussed by the authors. Different assays, cut-offs and time of blood sampling further complicate the interpretation.
A novel finding in this study is the impact of tachycardia. That hs-cTnT should be of greater importance when released during tachycardia seems counterintuitive. One would think that myocardial damage at normal heart rate is a more consequential finding than having some ‘troponin leakage’ during tachycardia, which may be observed in otherwise presumed healthy individuals (although at considerably higher heart rates). Based on our findings, one might speculate whether patients with AECOPD with tachycardia and elevated hs-cTnT may benefit from negative chronotropic agents, such as β-blockers. Such a speculation would be supported both by the strong general recommendation to prescribe β-blockers post-MI,26 and observational studies indicating that β-blockers may be beneficial for patients with COPD experiencing an MI.27 28 In this context, it is noteworthy that a 2008 Cochrane review concludes that:29 ‘… it is apparent that patients with COPD should not be excluded from future [cardioselective] betablocker trials so that the treatment effect can be studied in this substantial population.’
In agreement with other studies, we found that patients with AECOPD in general have poor prognosis. Using hs-cTnT we have identified a subgroup at particular risk. A recent meta-analysis of mortality subsequent to AECOPD indicated a 15.6% increase in the mortality rate after hospitalisation.30 It is not unlikely that myocardial injury accounts for a major proportion of these deaths.
Although not designed to permit any conclusions concerning underlying mechanisms for troponin release to be drawn, figure 3A,B suggests a different timing of deaths in patients with and without tachycardia. It is tempting to speculate that tachycardia-related troponin is associated with acute myocardial failure, cardiac arrhythmia or pulmonary embolism, all conditions carrying a poor short-term prognosis, whereas troponin elevation without concomitant tachycardia may be associated with subclinical coronary artery disease, more predictive of long-term outcome.
The choice of survival analyses merits some comments. In general the use of survival analyses with time-dependent covariables is preferable, because it takes into account that variables may change during the course of the study. Thus we believe that this method more accurately reflects the true association between hs-cTnT and survival than if only the first set of hs-cTnT values were to be used. In fact, we document that the model fit of the extended model was superior to that of the standard Cox model. Moreover, whereas the association between mortality and time-dependent hs-cTnT remains highly significant after inclusion of the baseline value, the converse is not true.
The main limitations of this study are the relatively small number of patients, and that the diagnosis of COPD was established retrospectively. Regarding the latter, we had spirometry results confirming the diagnosis in 88% of the patients. We believe that it would have been very time consuming and not cost-effective to recruit patients in a stable state before hospitalisation for AECOPD for the purpose of this study. In spite of the small number of patients, the primary predictor variable (ie, hs-cTnT) was associated with the main outcome measure, even after adjustment for four covariables.
Almost half of the eligible patients were not included. However, as failure to include was due to administrative reasons, selection bias is highly unlikely. The effect of heart rate was unexpected, hence the study was not designed to reach significance in the stratified analysis. There is a possibility that some of the patients may have had undiagnosed pulmonary embolism, which is associated with tachycardia, troponin elevation and mortality, and thus may influence the result.
Conclusion
Elevated hs-cTnT during AECOPD is an important and independent determinant of subsequent mortality. The effect seems more pronounced in patients with tachycardia.
References
Footnotes
See Editorial, p 745
An abstract of the results was presented in the poster session of the 2010 American Thoracic Society international conference, New Orleans, LA, USA.
Funding The study was financed by The Norwegian Association of Heart and Lung Patients and EXTRA funds from the Norwegian Foundation for Health and Rehabilitation.
Ethics approval This study was conducted with the approval of the Norwegian Data Inspectorate, and reviewed by the Regional Committee for Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Chronic obstructive pulmonary disease
- Chronic obstructive pulmonary disease
- Airwaves