Chronic kidney disease in pregnancy
BMJ 2008; 336 doi: https://doi.org/10.1136/bmj.39406.652986.BE (Published 24 January 2008) Cite this as: BMJ 2008;336:211
- David Williams, consultant obstetric physician 1,
- John Davison, emeritus professor obstetric medicine 2
- 1Institute for Women’s Health, EGA Obstetric Hospital, University College London Hospitals, London WC1E 6DH
- 2Royal Victoria Infirmary and Newcastle University, Newcastle upon Tyne
- Correspondence to: D Williams d.williams{at}uclh.nhs.uk
Chronic kidney disease is often clinically and biochemically silent until renal impairment is advanced. Symptoms are unusual until the glomerular filtration rate declines to <25% of normal, and more than 50% of renal function can be lost before serum creatinine rises above 120 μmol/l. Women who become pregnant with serum creatinine values above 124 μmol/l have an increased risk of accelerated decline in renal function and poor outcome of pregnancy (see Scenario box).1234 w1 Several factors must be considered when managing pregnant women with chronic kidney disease to minimise the adverse effects of pregnancy on maternal renal function and the consequent effects on the fetus.
Methods
Evidence for this review came from Medline and Cochrane database searches, as well as the authors’ reference archives.
How common is chronic kidney disease in pregnancy?
Chronic kidney disease is now widely classified into five stages according to the level of renal function (table 1⇓).w2 Stages 1 and 2 (normal or mild renal impairment with persistent albuminuria) affect up to 3% of women of child bearing age (20-39 years).w3 Stages 3-5 (glomerular filtration rate <60 ml/min) affect around one in 150 women of childbearing age,w3 but because of reduced fertility and an increased rate of early miscarriage, pregnancy in these women is less common. Studies of chronic kidney disease in pregnancy have mostly classified women on the basis of serum creatinine values, but we estimate that around one in 750 pregnancies is complicated by stages 3-5.w4 Some women are found to have chronic kidney disease for the first time during pregnancy. Around 20% of women who develop early pre-eclampsia (≤30 weeks’ gestation), especially those with heavy proteinuria, have previously unrecognised chronic kidney disease.w5
Stages of chronic kidney diseasew2
How do physiological changes of pregnancy affect the kidney?
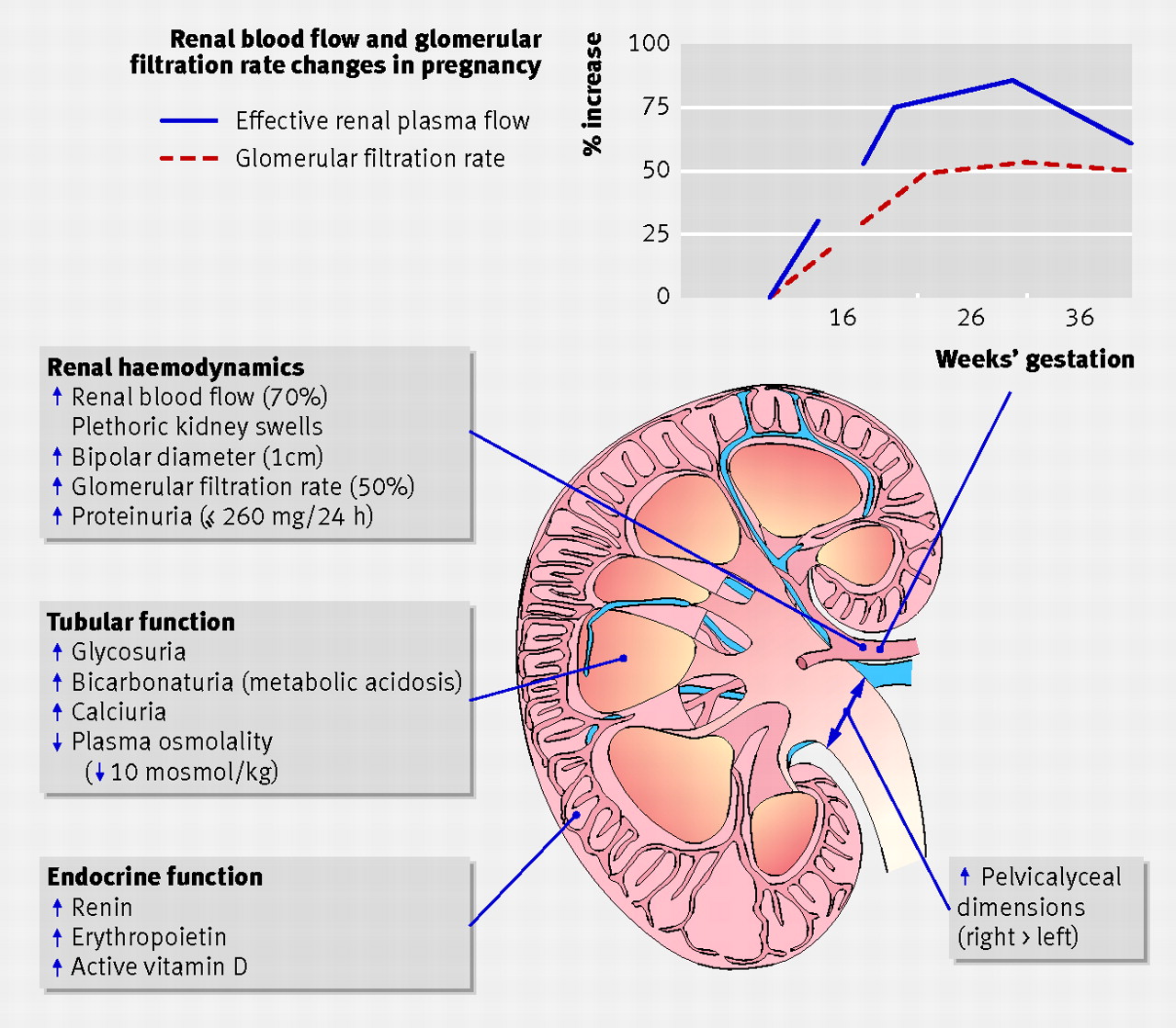
The kidneys undergo pronounced haemodynamic, renal tubular, and endocrine changes during pregnancy (figure⇓; table 2⇓).5 w6 During healthy pregnancy the kidney increases production of erythropoietin, active vitamin D, and renin.6
Physiological changes to the kidney during healthy pregnancy
{kind=link}
Physiological changes in common indices of renal function during healthy pregnancy. Values are mean (SD)5 w6
From early pregnancy, increased renal blood flow leads to an increase in glomerular filtration rate of more than 50% (figure⇑). Gestational hyperfiltration is accompanied by a relative decrease in concentrations of serum creatinine and urea, so values considered normal in the non-pregnant state may be abnormal in pregnancy (table 2⇑). The plethoric kidneys appear larger on ultrasonography and—combined with renal pelvis and ureteric dilatation—these normal changes seen in pregnancy mimic outflow obstruction.w7 A 5-10 g/l fall in plasma albumin, a rise in serum cholesterol, and oedema in late pregnancy can also occur in normal pregnancy, and sometimes simulate nephrotic syndrome.
Can diseased kidneys tolerate normal physiological changes of pregnancy?
Women with chronic kidney disease are less able to make the renal adaptations needed for a healthy pregnancy. Their inability to boost renal hormones often leads to normochromic normocytic anaemia, reduced expansion of plasma volume, and vitamin D deficiency.6 The gestational rise in glomerular filtration rate is blunted in women with moderate renal impairment and usually absent in those with a serum creatinine higher than 200 µmol/l.4 7 8 If pre-eclampsia develops, maternal renal function often deteriorates further, but the addition of a prerenal insult that will reduce renal blood flow, such as peripartum haemorrhage or regular use of a non-steroidal anti-inflammatory drug, can seriously threaten maternal renal function. In such circumstances, nephrotoxic drugs must be avoided and maternal circulation restored with careful fluid management, as women with pre-eclampsia are prone to pulmonary oedema.
How does pregnancy affect maternal kidney function?
Mild renal impairment (stages 1-2)
Most women with chronic kidney disease who become pregnant have mild renal dysfunction and pregnancy does not usually affect renal prognosis (table 3⇓). A case-control study of 360 women with primary glomerulonephritis and mild renal dysfunction (serum creatinine <110 μmol/l), minimal proteinuria (<1 g/24 h), and absent or well controlled hypertension before pregnancy showed that pregnancy had little or no adverse effect on long term (up to 25 years) renal function in the mother.9 The situation is different for women with moderate to severe renal impairment.
Estimated effects of prepregnancy renal function on pregnancy outcome and maternal renal function. Values are the estimated percentage of women or neonates affected
Moderate to severe renal impairment (stages 3-5)
Small mainly uncontrolled retrospective studies have shown that women with the worst renal function before pregnancy are at greatest risk of an accelerated decline in renal function during pregnancy (table 3⇑). Pre-existing proteinuria and hypertension both increase this risk.2 4 8 w17 w18 A retrospective series of women with chronic kidney disease (87 pregnancies) found that those who initially had moderate renal impairment (serum creatinine 124-168 mmol/l) had a 40% risk of a decline in renal function during pregnancy, which persisted after birth in about half of those affected.3 However, 13 of 20 women with severe renal impairment (serum creatinine >177 mmol/l) had a decline in renal function during the third trimester, which persisted in most women and deteriorated to end stage renal failure in seven.3 w1
A prospective study assessing the rate of decline of maternal renal function during pregnancy in 49 women with chronic kidney disease stages 3-5 before pregnancy confirmed these earlier observations.2 Women with both an estimated glomerular filtration rate <40 ml/min/1.73 m2 and proteinuria >1 g/24 h before pregnancy showed an accelerated decline in renal function during pregnancy.2 Chronic hypertension predisposes women to pre-eclampsia—this may explain why some women with milder renal dysfunction also have a gestational decline in renal function.2 3 The risk of such a decline is reduced when hypertension is controlled.
How does chronic kidney disease affect pregnancy outcome?
Maternal hypertension, proteinuria, and recurrent urinary tract infection often coexist in women with chronic kidney disease, and it is difficult to tell how much each of these factors contributes to a poor pregnancy outcome. It seems, however, that each factor is individually and cumulatively detrimental to fetal outcome.234 678 w1
Women with severe renal impairment have the greatest difficulty conceiving, the highest rate of miscarriage, and the poorest pregnancy outcome.1234 78 The degree of renal dysfunction correlates with the risk of a poor pregnancy outcome (table 3).
How should chronic kidney disease be managed in pregnancy?
All women with chronic kidney disease should be referred early in pregnancy to an obstetrician and other specialist as necessary, to plan subsequent antenatal care. However, with a few exceptions, the most important aspects of managing chronic kidney disease in pregnancy relate to managing associated clinical features, rather than the type of kidney disease. Regular monitoring of maternal renal function (serum creatinine and serum urea), blood pressure, midstream urine (for infection), proteinuria, and when appropriate ultrasound (to detect urological obstruction) should identify pathological changes and allow timely intervention to optimise perinatal outcome and maternal renal outcome (table 4⇓).
Care of women with chronic kidney disease during pregnancy
Before pregnancy
Ideally, all women with chronic kidney disease should be made aware of the risks to their long term renal function and to the fetus before they conceive (table 3). Women with chronic kidney disease often have amenorrhoea but may still occasionally ovulate and thus conceive. Contraceptive measures that consider clinical comorbidities should be taken by those who do not wish to become pregnant.
Folic acid 400 µg daily should be given as usual before conception until 12 weeks’ gestation. Low dose aspirin (50-150 mg/day) should be started in early pregnancy to reduce the risk of pre-eclampsia and improve perinatal outcome.10 Regular drugs should be reviewed. Fetotoxic drugs—such as angiotensin converting enzyme inhibitors and angiotensin II receptor blockers—should be stopped before pregnancy if equally effective drugs are available, or as soon as pregnancy is confirmed, if they are thought to be important for protecting maternal renal function.w22
During pregnancy
Chronic kidney disease includes a wide range of different conditions, and monitoring during pregnancy must be tailored to the severity of the disease and its complications (tables 4, 5⇓). In general, all clinical and biochemical features should be checked more often as pregnancy progresses or if changes suggest deteriorating kidney function. Specialist care should begin early in pregnancy, but much of the monitoring of women with stage 1-2 disease can be done by primary care doctors.
Summary of important points regarding specific kidney diseases during pregnancy
When should specialists be involved?
Optimal management of pregnant women with chronic kidney disease often involves the combined expertise of specialists in obstetrics, nephrology, urology, fetal medicine, and neonatology. Impressive improvements in perinatal outcome over recent decades have been driven by advances in all of these specialties.234 w1 Sonographic assessment of uterine artery blood flow at 20-24 weeks’ gestation can refine the risk of later pre-eclampsia and fetal growth restriction.w32 Difficult decisions about the timing of delivery and managing renal function in women with kidney transplants and systemic disorders such as systemic lupus erythematosus and other vasculitidies require expert management.6 Urological expertise is necessary for the management of obstructive disorders involving renal stones, congenital pelvo-ureteric abnormalities, or rare gestational obstructive disorders.6 Maternal renal conditions with a genetic basis sometimes require specialist fetal medicine or genetic advice. The most common inherited renal condition, autosomal dominant polycystic kidney disease, is passed on to 50% of offspring.
Postpartum care
It can take up to three months, occasionally longer, for the physiological changes of pregnancy to disappear. During that time, close monitoring of fluid balance, renal function, blood pressure, and a further review of drug treatment are necessary. Women who have new onset proteinuria associated with pre-eclampsia should be followed until proteinuria disappears, or until a diagnosis of renal disease is made.
Breast feeding should be encouraged in women with chronic kidney disease. Information is confusing as to the extent to which some immunosuppressive drugs—such as ciclosporin and tacrolimus—appear in breast milk,w33 but prednisolone, azathioprine, and angiotensin converting enzyme inhibitors are barely detectable in breast milk. It is still unclear whether the benefits of breast feeding are countered by neonatal absorption of immunosuppressive drugs. We generally encourage mothers who want to breast feed but are taking immunosuppressive drugs to do so as long as the baby is thriving.
Conclusions
Women with chronic kidney disease who become pregnant usually have mild renal dysfunction (stages 1-2) and have an uneventful pregnancy and good renal outcome. Clinical features, in particular uncontrolled hypertension, heavy proteinuria (>1 g/24 h), and recurrent urinary tract infections have an independent and cumulative negative effect on the outcome of pregnancy. Women with moderate to severe disease (stages 3-5) are at highest risk of complications during pregnancy and of an accelerated decline in renal function. Successful management of women with chronic kidney disease during pregnancy requires team work between primary care clinicians, midwives, specialists, and the patient. Frequent monitoring of simple clinical and biochemical features will guide timely expert intervention to achieve optimal pregnancy outcome and conservation of maternal renal function.
Scenario
A 37 year old woman with a history of reflux nephropathy and recurrent urinary tract infections presented for prepregnancy counselling with a serum creatinine of 153 μmol/l, hypertension controlled with ramipril 5 mg daily, and proteinuria of 1.4 g/24 h. The effect of pregnancy on her renal function and the increased risk of complications during pregnancy were explained. She was advised to take folic acid 400 μg daily and as soon as she knew she was pregnant to stop ramipril and start low dose aspirin (75 mg daily) to reduce the risk of pre-eclampsia.
She presented again 18 months later at 10 weeks’ gestation. Her blood pressure was 144/92 mm Hg with no antihypertensives, serum creatinine was 136 μmol/l, and she had an asymptomatic urinary tract infection with Escherichia coli. The infection was treated with cefalexin 500 mg three times daily for seven days, and prophylactic cefalexin 125 mg nightly was continued for the rest of the pregnancy. Thromboprophylaxis with low molecular weight heparin (enoxaparin 40 mg daily) was started because of the prothrombotic effect of proteinuria (>1 g/24 h) and pregnancy. At 28 weeks, her blood pressure was 152/98 mm Hg and she was treated with nifedipine SR 10 mg twice daily. At 29 weeks, her blood pressure rose to 166/104 mm Hg, despite increased nifedipine SR 20 mg twice daily, and her renal function started to deteriorate (serum creatinine 188 μmol/l). Pre-eclampsia was diagnosed from the rise in blood pressure, raised liver transaminases (alanine transaminase 147 IU/l, aspartate transaminase 96 IU/l), and fall in platelet count (to 82×109/l) Fetal growth was at the fifth centile and had been reviewed with ultrasound every two weeks since 24 weeks’ gestation. A caesarean section was carried out at 30+2 weeks because of signs of fetal distress and worsening maternal pre-eclampsia and renal function (serum creatinine 209 μmol/l), and a 1.1 kg baby boy was delivered.
Six months later, maternal renal function had not recovered to prepregnancy levels (serum creatinine 193 μmol/l). Hypertension was treated with ramipril and nifedipine SR. The baby was doing well, although he was still small for age.
Footnotes
This is one of a series of occasional articles about how to manage a pre-existing medical condition during pregnancy.
Contributors: DW and JD both contributed to the research and writing of this manuscript.
Funding: DW works at UCLH/UCL and receives a proportion of his salary from the Department of Health’s NIHR Biomedical Research Centres funding scheme.
Competing interests: None declared.
Provenance and peer review: Commissioned; externally peer reviewed.