Antithrombotic therapy for atrial fibrillation
BMJ 2002; 325 doi: https://doi.org/10.1136/bmj.325.7371.1022 (Published 02 November 2002) Cite this as: BMJ 2002;325:1022
- Gregory Y H Lip,
- Robert G Hart,
- Dwayne S G Conway
Atrial fibrillation is the commonest sustained disorder of cardiac rhythm. Although patients often present with symptoms caused by haemodynamic disturbance associated with the rhythm itself, the condition carries an increased risk of arterial thromboembolism and ischaemic stroke due to embolisation of thrombi that form within the left atrium of the heart. Presence of the arrhythmia confers about a fivefold increase in stroke risk, an absolute risk of about 4.5% a year, although the precise annual stroke risk ranges from <1% to >12%, according to the presence or absence of certain clinical and echocardiographically identifiable risk factors.

Severely damaged left atrial appendage endocardial surface with thrombotic mass in a patient with atrial fibrillation and mitral valve disease
From trial data, patients with paroxysmal atrial fibrillation seem to carry the same risk as those with persistent atrial fibrillation. The same criteria can be used to identify high risk patients, although it is unclear whether the risk is dependent on the frequency and duration of the paroxysms.
Randomised controlled trials have shown the benefit of warfarin and, to a lesser extent, aspirin in reducing the incidence of stroke in patients with atrial fibrillation without greatly increasing the risk of haemorrhagic stroke and extracranial haemorrhage. However, anticoagulant therapy is still underprescribed in patients with atrial fibrillation, particularly in elderly patients, who stand to benefit most
Evidence from clinical trials
It is well established that antithrombotic therapy confers thromboprophylaxis in patients with atrial fibrillation who are at risk of thromboembolism. A recent meta-analysis of antithrombotic therapy in atrial fibrillation showed that adjusted dose warfarin reduced stroke by about 60%, with absolute risk reductions of 3% a year for primary prevention and 8% a year for secondary prevention (numbers needed to treat for one year to prevent one stroke of 33 and 13, respectively). In contrast, aspirin reduced stroke by about 20%, with absolute risk reductions of 1.5% a year for primary prevention and 2.5% a year for secondary prevention (numbers needed to treat of 66 and 40, respectively). Relative to aspirin, adjusted dose warfarin reduced the risk by about 40%, and the relative risk reduction was similar for primary and secondary prevention, and for disabling and non-disabling strokes. However, these data, obtained from well planned clinical trials recruiting patients with relatively stable conditions, are unlikely to be fully extrapolable to all patients in general practice, so that some caution is advised.

Meta-analysis of trials comparing warfarin with placebo in reducing the risk of thromboembolism in patients with atrial fibrillation AFASAK=Copenhagen atrial fibrillation, aspirin, and anticoagulation study; BAATAF=Boston area anticoagulation trial for atrial fibrillation; CAFA=Canadian atrial fibrillation anticoagulation study; EAFT=European atrial fibrillation trial; SPAF=Stroke prevention in atrial fibrillation study; SPINAF=Stroke prevention in non-rheumatic atrial fibrillation
{kind=link}
Overall, warfarin (generally at a dose to maintain an international normalised ratio (INR) of 2-3) is significantly more effective than aspirin in treating atrial fibrillation in patients at high risk of stroke, especially in preventing disabling cardioembolic strokes. The effect of aspirin seems to be on the smaller, non-cardioembolic strokes from which elderly, and often hypertensive, patients with atrial fibrillation are not spared.
Recent clinical trials have suggested that there is no role for minidose warfarin (1 mg/day regardless of INR), alone or in combination with antiplatelet agents or aspirin, as thromboprophylaxis in atrial fibrillation. However, the role of other antiplatelet agents (such as indobufen and dipyridamole) in atrial fibrillation is still unclear. One small trial (SIFA) compared treatment with indobufen, a reversible cyclo-oxygenase inhibitor, with full dose warfarin for secondary prevention and found no statistical difference between the two groups, who were well matched for confounding risk factors. Trials of other antiplatelet and antithrombotic drugs (including low molecular weight heparin) have been performed but have generally been too small and underpowered to show significant differences. Large multinational trials comparing a direct thrombin inhibitor (ximelagatran) with adjusted dose warfarin in over 7000 patients at high risk of atrial fibrillation are nearing completion and should be reported in 2003.

Meta-analysis of trials comparing aspirin with placebo in reducing risk of thromboembolism in patients with atrial fibrillation AFASAK=Copenhagen atrial fibrillation, aspirin, and anticoagulation study; EAFT=European atrial fibrillation trial; ESPS II= European stroke prevention study II; LASAF=Low-dose aspirin, stroke, and atrial fibrillation pilot study; SPAF=Stroke prevention in atrial fibrillation study; UK-TIA=United Kingdom TIA study
{kind=link}
The reduction in relative risk with warfarin applies equally to primary and secondary prevention but, as history of stroke confers an increased annual stroke risk (12% v 4.5%), the absolute risk reduction is greater for secondary prevention. The number of patients with atrial fibrillation needing treatment with warfarin to prevent one stroke is therefore about three times greater in primary prevention (37) than in secondary prevention (12).
Treatment with full dose anticoagulation carries the potential risk of major bleeding, including intracranial haemorrhage. Meta-analysis of the initial five primary prevention trials plus a further secondary prevention trial suggests the risk of haemorrhagic stroke is only marginally increased from 0.1% to 0.3% a year. Higher rates of major haemorrhage were seen in elderly patients and those with higher intensity anticoagulation. Further recent trials have confirmed an increased bleeding risk in patients with INR >3.

Meta-analysis of trials comparing warfarin with aspirin in reducing risk of thromboembolism in patients with atrial fibrillation AFASAK=Copenhagen atrial fibrillation, aspirin, and anticoagulation study; EAFT=European atrial fibrillation trial; PATAF=Prevention of arterial thromboembolism in atrial fibrillation; SPAF=Stroke prevention in atrial fibrillation study
{kind=link}
Antiplatelet therapy in atrial fibrillation
Several clinical trials have studied the effects of aspirin in atrial fibrillation, with doses ranging from 25 mg twice daily to 1200 mg a day. Overall, aspirin reduces the relative risk of stroke by about 20% (a figure which just reaches statistical significance) with no apparent benefit of increasing aspirin dose. Aspirin seems to carry greater benefit in reducing smaller non-disabling strokes than disabling strokes. This may be due to an effect primarily on carotid and cerebral artery platelet thrombus formation, rather than on formation of intra-atrial thrombus. A meta-analysis of trials directly comparing full dose warfarin with aspirin confirmed significant reductions in stroke risk about three times greater with warfarin. The SPAF III trial demonstrates that addition of fixed low doses of warfarin to aspirin treatment is not sufficient to achieve the benefits of full dose warfarin alone.
Putting the evidence into practice
Despite the evidence from the trials, many doctors are reluctant to start warfarin treatment for patients with atrial fibrillation. This could be due to fears (of patient and doctor) of haemorrhagic complications in an elderly population, logistical problems of INR monitoring, and a lack of consensus guidelines on which patients to treat and the ideal target INR. Such attitudes may result in otherwise avoidable stroke and arterial thromboembolism. A systematic evidence based approach needs to be encouraged, targeting appropriate antithrombotic therapy at those patients who stand to gain most benefit (those at greatest risk of thromboembolism) and using levels of anticoagulation that have been proved both effective and reasonably safe for both primary and secondary prevention of stroke, if we are to realise in clinical practice the large reduction in incidence of stroke achieved in the clinical trials.
Independent predictors of ischacmic stroke in non-valve atrial fibrillation
Consistent predictors
Old age
Hypertension
Previous stroke or transient ischaemic attack
Left ventricular dysfunction*
Inconsistent predictors
Diabetes
Systolic blood pressure >160 mm Hg†
Women, especially older than 75 years
Postmenopausal hormone replacement therapy
Coronary artery disease
Factors which decrease the risk of stroke
Moderate to severe mitral regurgitation
Regular alcohol use (>14 drinks in two weeks)
*Recent clinical congestive cardiac failure or moderate to severe systolic dysfunction on echocardiography
†In some analyses, systolic blood pressure >160 mm Hg remained an independent predictor after adjustment for hypertension
Who to treat?
Even though there are impressive figures for relative risk reduction with warfarin, the figures for absolute risk reduction (more important in clinical practice) depend greatly on the underlying risk of stroke if untreated. Elderly patients are often denied anticoagulant therapy because of fears of increased haemorrhage risk. However, the benefits of anticoagulant therapy are greater for elderly patients because of the increased underlying thromboembolic risk. Conversely, young patients at relatively low risk of stroke have less to gain from full dose anticoagulation as there may be little difference between the number of strokes prevented and the number of haemorrhagic complications. Risk stratification is possible using the clinical and echocardiographic parameters and can be used to target treatment at the most appropriate patients.
Practical guidelines for antithrombotic therapy in non-valvar atrial fibrillation
Assess risk, and reassess regularly High risk (annual risk of cerebrovascular accident=8-12%)
All patients with previous transient ischaemic attack or cerebrovascular accident
All patients aged 75 with diabetes or hypertension
All patients with clinical evidence of valve disease, heart failure, thyroid disease, and impaired left ventricular function on echocardiography*
Treatment—Give warfarin (target INR 2-3) if no contraindications and possible in practice
Moderate risk (annual risk of cerebrovascular accident=4%)
All patients <65 with clinical risk factors: diabetes, hypertension, peripheral vascular disease, ischaemic heart disease
All patients >65 not in high risk group
Treatment—Either warfarin (INR 2-3) or aspirin 75-300 mg daily. In view of insufficient clear cut evidence, treatment may be decided on individual cases. Referral and echocardiography may help
Low risk (annual risk=1%)
All patients aged <65 with no history of embolism, hypertension, diabetes, or other clinical risk factors
Treatment—Give aspirin 75-300 mg daily
*Echocardiogram not needed for routine risk assessment but refines clinical risk stratification in case of moderate or severe left ventricular dysfunction (see figure below) and valve disease. A large atrium per se is not an independent risk factor on multivariate analysis
Risk stratification for thromboprophylaxis can be undertaken in many ways. Clinical risk factors would assist with risk stratification in most cases. Although echocardiography is not mandatory, it would help refine risk stratification in cases of uncertainty. Based on echocardiographic data on 1066 patients, atrial fibrillation investigators reported that the only independent predictor of stroke risk was moderate or severe left ventricular dysfunction on two dimensional echocardiography. Left atrial size on M mode echocardiography was not an independent predictor on multivariate analysis. Transoesophageal echocardiography is rarely needed to undertake risk stratification, but “high risk” features include the presence of dense spontaneous echocardiographic contrast (often with low atrial appendage velocities, indicating stasis), the presence of thrombus of the atrial appendage, and complex aortic plaque.
Different risk stratification schemes for primary prevention of stroke in non-valvar atrial fibrillation
Different risk stratification schemes for primary prevention of stroke in non-valvar atrial fibrillation

Two dimensional echocardiography showing left atrial thrombus in patient with prosthetic valve

Effect of left ventricular funtion on stroke rate in atrial fibrillation LV=left ventricle
{kind=link}
Which INR range?
The evidence suggests that INR levels greater than 3 may result in an excess rate of haemorrhage, whereas low dose warfarin regimens (with INR maintained below 1.5) do not achieve the reductions in stroke of higher doses. An INR range of between 2 and 3 has been shown to be highly effective without leading to excessive haemorrhage and should therefore be recommended for all patients with atrial fibrillation treated with warfarin unless they have another indication for higher levels of anticoagulation (such as a mechanical heart valve). Although INR monitoring is often coordinated by hospital based anticoagulant clinics, general practitioners are likely to play a more important part with the development of near patient INR testing.
Recommendations for anticoagulation for cardioversion of atrial fibrillation
For elective cardioversion of atrial fibrillation of >48 hours duration start warfarin treatment (INR 2-3) three weeks before and continue for four weeks after cardioversion
In urgent and emergency cardioversion administer intravenous heparin followed by warfarin
Treat atrial flutter similarly
No anticoagulation treatment is required for supraventricular tachycardia or atrial fibrillation of <48 hours duration
Continue anticoagulation in patients with multiple risk factors or those at high risk of recurrent thromboembolism
Based on the 6th ACCP Consensus Conference on Antithrombotic Therapy
Particular care must be taken and INR levels closely monitored when warfarin is used in elderly patients. It has been suggested that an INR of between 1.6 and 2.5 can provide substantial, albeit partial, efficacy (estimated to be nearly 90% of the highest intensities). Given the uncertainty about the safety of INRs >2.5 for atrial fibrillation patients over 75 years, a target INR of 2 (range 1.6-2.5) may be a reasonable compromise between an increased risk of haemorrhage and a reduced risk of thrombotic stroke for some patients within this age group, in the absence of additional risk factors, pending further data about the safety of higher intensities.
The ongoing MRC sponsored Birmingham atrial fibrillation trial of anticoagulation in the aged (BAFTA) is comparing warfarin with aspirin in atrial fibrillation patients over 75 years to further define the relative benefits and risks.
Further reading
Hart RG, Pearce LA, Rothbart RM, McAnulty JH, Asinger RW, Halperin JL. Stroke with intermittent atrial fibrillation: incidence and predictors during aspirin therapy. Stroke Prevention in Atrial Fibrillation Investigators.
Lip GYH. Does atrial fibrillation confer a hypercoagulable state? Lancet 1995;346:1313-4
Lip GYH. Thromboprophylaxis for atrial fibrillation. Lancet1999; 353:4-6
Lip GYH, Kamath S, Freestone B. Acute atrial fibrillation. Clinical Evidence June Issue 7. BMJ Publishing Group. 2002
Straus SE, Majumdar SR, McAlister FA. New edvidence for stroke prevention: scientific review. JAMA 2002;288:1388
Thomson R, Parkin D, Eccles M, Sudlow M, Robinson A. Decision analysis and guidelines for anticoagulant therapy to prevent stroke in patients with atrial fibrillation. Lancet 2000;355:956-62
DC cardioversion
No hard evidence exists in the literature that restoration of sinus rhythm by whatever means reduces stroke risk. Transoesophageal echocardiography performed immediately before cardioversion (to exclude intra-atrial thrombus) may allow DC cardioversion to be performed without prior anticoagulation. However, as the thromboembolic risk may persist for a few weeks postprocedure, it is still recommended that patients receive warfarin for at least four weeks afterwards.
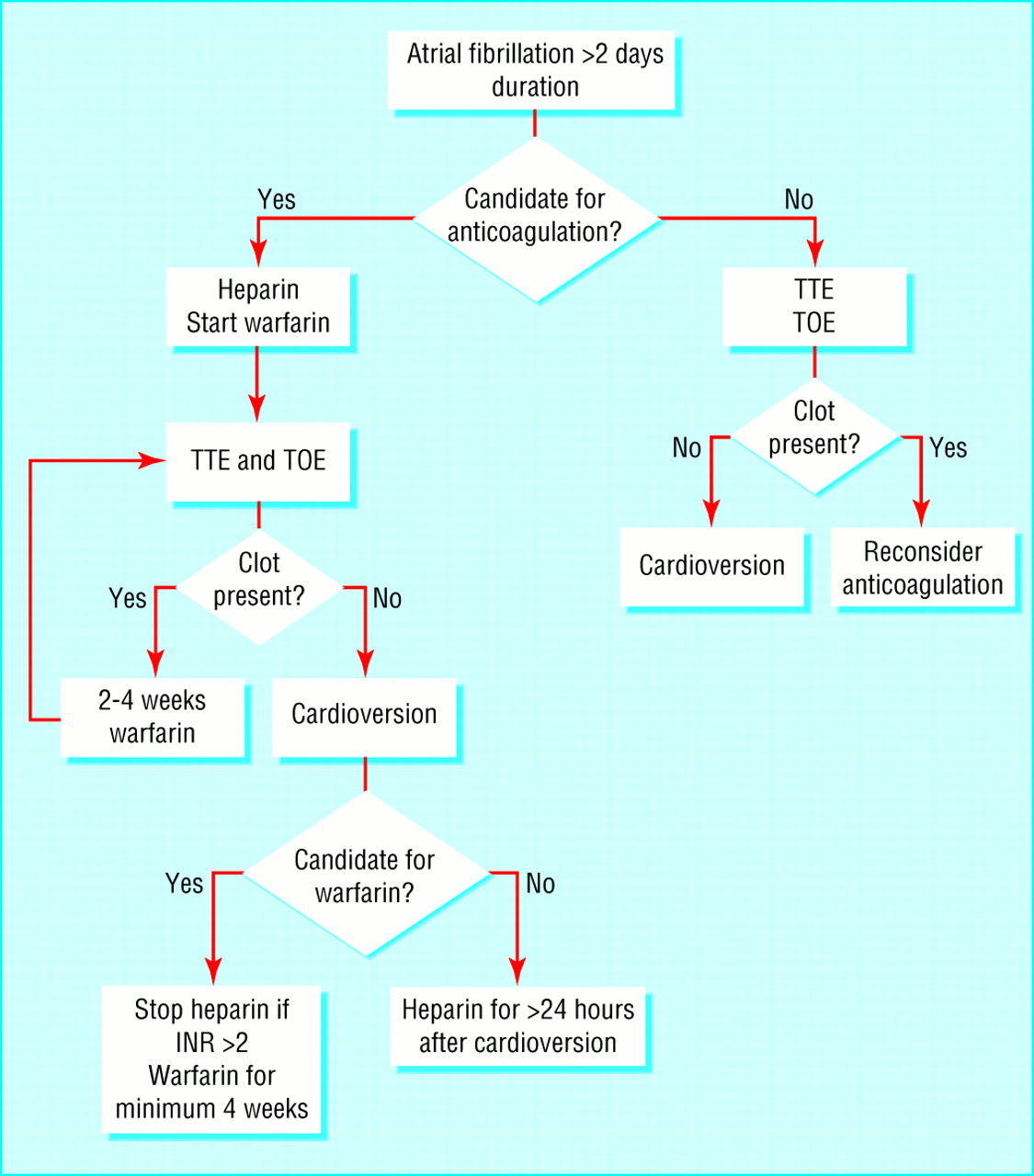
Guidelines for transoesophageal echocardiography guided cardioversion TOE=transoesophageal echocardiography; TTE=transthoracic echocardiography
{kind=link}
Acknowledgments
The figures showing a severely damaged left atrial appendage endocardial surface is reproduced from Goldsmith I et al, Am Heart J2000;140:777-84 with permission from Mosby. The figures showing results of trials comparing warfarin with placebo, aspirin with placebo, and warfarin with aspirin are adapted from Hart RG et al, Ann Intern Med 1999;131:492-501. The independent predictors of ischaemic stroke are adapted from Hart RG et al, Ann Intern Med 1999;131:688-95. The practical guidelines for antithrombotic therapy in non-valvar patients is adapted from Lip GYH, Lancet 1999;353:4-6. The table containing risk stratification schemes for primary prevention of stroke is adapted from Pearce LA et al, Am J Med 2000;109:45-51. Guidelines for transoesophageal echocardiography guided cardioversion is adapted from the ACUTE Study, N Engl J Med 2001;344:1411-20. The recommendations for anticoagulation for cardioversion of atrial fibrillation are based on the 6th ACCP Consensus Conference on Antithrombotic Therapy. Albers GW et al, Chest 2001;119:194-206S.
Footnotes
-
Gregory Y H Lip is professor of cardiovascular medicine and Dwayne S G Conway is research fellow at the haemostasis thrombosis and vascular biology unit, university department of medicine, City Hospital, Birmingham, Robert G Hart is professor of neurology, department of medicine (neurology), University of Texas Health Sciences Center, San Antonio, USA.
The ABC of antithrombotic therapy is edited by Gregory Y H Lip and Andrew D Blann, senior lecturer in medicine at the haemostasis thrombosis and vascular biology unit, university department of medicine, City Hospital, Birmingham. The series will be published as a book in spring 2003.