Article Text

Statistics from Altmetric.com
Learning objectives
Contemporary indications for mitral valve repair in patients with degenerative mitral valve disease.
Patient selection criteria for minimally invasive mitral valve repair.
Technical mandates of minimally invasive mitral valve repair including mini-thoracotomy and robotic approach.
Pros and cons of minimally invasive approaches.
Introduction
Modified cardiopulmonary bypass techniques, including vacuum-assisted venous drainage, were introduced in 1995 and enabled safe and effective minimally invasive mitral valve (MV) surgery. Approaches have evolved since the first successful right parasternal, trans-sternal and right mini-thoracotomy heart valve surgeries.1–3 However, difficulties performing complex MV repair using two-dimensional vision and long-shafted instruments limited adoption. Development of the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, California) addressed this limitation and allowed surgeons to perform complex reconstructive operations using three-dimensional (3D) visualisation. Falk and colleagues reported on the first robotic system for valvular heart surgery.4 Soon thereafter, Carpentier and colleagues performed the first successful robotic MV repair using the da Vinci Surgical System (Intuitive Surgical).5 In 2000, Chitwood and colleagues carried out the first robotically assisted MV repair in the USA as part of the initial Food and Drug Administration clinical trial.6
The most important benefits of robotic MV surgery include enhanced surgical dexterity with precise movements of instruments in the closed chest, excellent visualisation of the subvalvular apparatus and quicker patient return to normal activity with superior cosmetic results compared with sternotomy approaches. In this review, we delineate different aspects of mini-thoracotomy and robotic approaches to MV repair.
Contemporary indications for MV repair
Over the past decade, there has been a growing body of data highlighting the deleterious consequences of uncorrected severe degenerative mitral regurgitation (MR). Evidence supporting early MV repair in patients with severe asymptomatic MR and preserved cardiac structure and function includes (1) reduced severity of degenerative MR with MV repair; (2) excess long-term mortality and risk of heart failure in patients with severe uncorrected MR7–9; (3) effective, durable and safe MV repair with very low risks of postoperative mortality and morbidity, regardless of complexity of degenerative MV disease7 10–12; and (4) routinely available ‘small incision’ approaches that minimise the perceived burden of early surgical intervention. Minimally invasive and robotic procedures are associated with rapid patient recovery and excellent safety and quality and offer similar costs compared with sternotomy operations at certain centres.7 10–12
Therefore, the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) guidelines strongly recommend (class I) prompt surgical correction of MR for patients in stages D (severe symptomatic MR) and C2 (severe asymptomatic MR with left ventricular ejection fraction (LVEF) <60% or left ventricular end-systolic diameter (LVESD) >40 mm) and also include a new recommendation (class IIa) for early correction of MR in stage C1 patients (severe asymptomatic MR with LVEF >60% or LVESD <40 mm) if mortality risk is <1% and rate of repair is >95%.8
Patient selection
Minimally invasive mitral repair is appropriate for both degenerative and functional MV disease. However, operative risks and mitral anatomy should be considered when selecting patients for the procedure. Patients should be screened for comorbidities that may preclude safe application of this technique.13 Mini-thoracotomy and robotic MV repair generally are accomplished through a right chest approach, and thus, intra-thoracic pathology may be a contraindication (table 1). Many of these contraindications are relative and can be safely managed to enable a minimally invasive MV repair.
Contraindications and relative contraindications for minimally invasive mitral valve repair
Patients at risk for coronary artery disease should undergo a cardiac catheterisation or CT angiography. Patients with significant risk factors for carotid/peripheral vascular disease should be screened by ultrasound/CT. A right heart catheterisation may be indicated in patients who have significant pulmonary hypertension, particularly in the setting of depressed right ventricular function.
Minimally invasive approaches mandate peripheral vascular access for cardiopulmonary bypass. Specifically, establishment of cardiopulmonary bypass via retrograde perfusion of the femoral vessels requires that atherosclerotic disease is evaluated in elderly to prevent cerebral embolism or retrograde aortic dissection.14 15 Furthermore, severe sternal or thoracic deformities can compromise thoracoscopic or robotic instrument trajectories. Therefore, candidates should be evaluated by CT scan of the chest, abdomen and pelvis.
A transthoracic echocardiography (TTE) or transoesophageal echocardiography (TOE) study should be performed to confirm the diagnosis and determine the repair plan. TOE is also essential in the operating room to identify detailed MV anatomy/pathology.
Technical mandates of minimally invasive MVR
Minimally Invasive MV repair techniques, including anterolateral right mini-thoracotomy and robotic approaches, share procedural similarities including retrograde perfusion, exposure of the valve and repair techniques.
Robotic approach
The patient is intubated with a double-lumen endotracheal tube, and a TOE probe is placed. Pulmonary artery vent and retrograde coronary sinus cardioplegia catheters (CardioVations; Ethicon) may be placed via the right internal jugular vein under TOE guidance. However, we have not found them to be necessary. The patient is positioned at the right edge of the operating room table with a transverse roll under the chest. The right femoral artery and vein are exposed via an oblique incision above the groin crease and assessed for appropriateness for cannulation.16
The endoscope camera port is placed in the fourth intercostal space (ICS), 2 to 3 cm lateral to the nipple. In female patients, the breast is retracted superiorly, and the incision is placed in the infra-mammary crease to enter the chest in the fourth or fifth ICS. The working port incision (for a 15 mm soft rubber retractor) is placed in the fourth ICS 4 cm lateral to the camera port. The left instrument port is placed two interspaces above and approximately halfway between the shoulder and the camera port. The right instrument port is two interspaces below and near the anterior axillary line. The fourth robotic port for the atrial retractor instrument is placed in the fourth ICS medial to the camera port (figure 1A).16
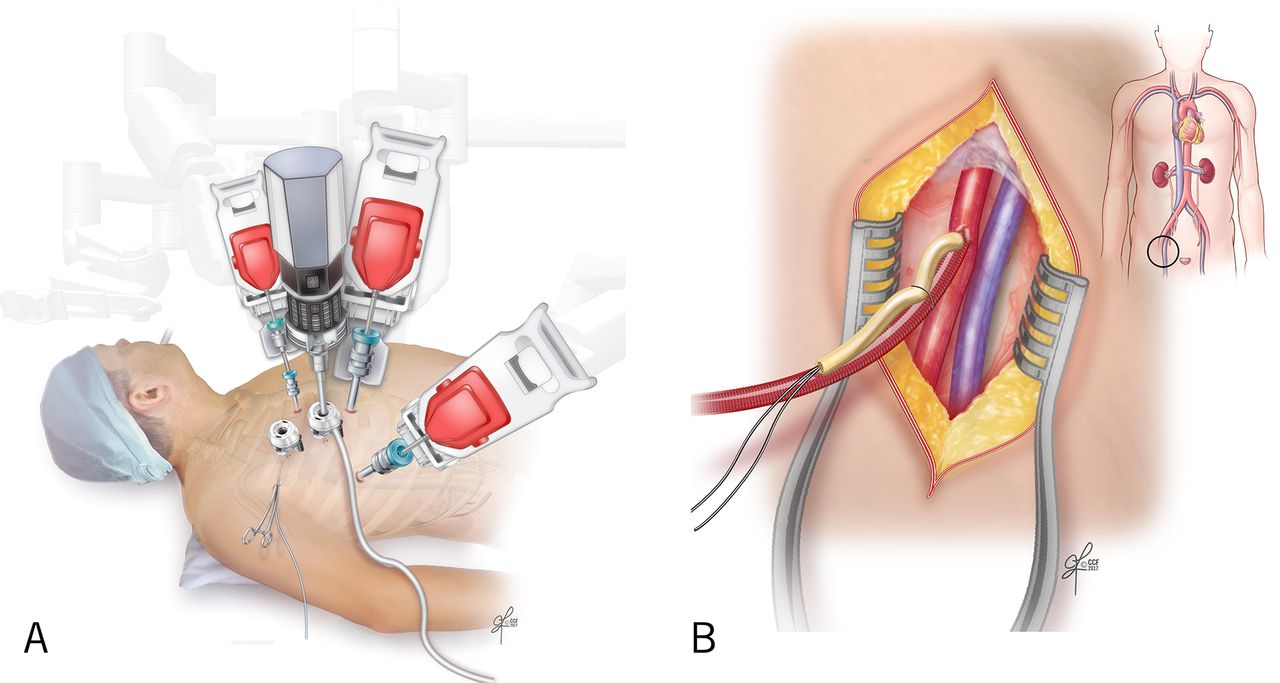
Patient setup. (A) Port placement. (B) Cannulation of the femoral vessels.
A purse-string suture is placed in the anterior surface of the femoral vein, and then a guidewire is passed through the femoral vein into the superior vena cava under TOE guidance. A venous cannula is passed over the wire and positioned so that the tip is several centimetres up the inferior vena cava (IVC). The femoral artery is cannulated using Seldinger technique (figure 1B). Cardiopulmonary bypass is initiated. The pericardium is opened anterior to the phrenic nerve. The pericardiotomy extends from near the IVC to up over the ascending aorta (figure 2).16
Opening of the pericardium.
The table is rotated all the way to the left and placed in reverse Trendelenberg. The da Vinci robot is brought to the surgical field, and the arms and camera are positioned in the respective ports.
Aortic occlusion (figure 3A) is achieved using the thransthoracic clamp (via a stab wound in the axilla), and cardioplegia is delivered antegrade and can be readministered every 15–20 min throughout the cross-clamp time. The endoballoon may be used. However, we have not found it to be necessary in the majority of the cases. A left atriotomy incision is made anterior to the right pulmonary veins (figure 3B). The atrial retractor is positioned to elevate the atrial septum and enhance the exposure of the MV. A small suction vent is positioned in the left pulmonary veins to clear the surgical field of blood.
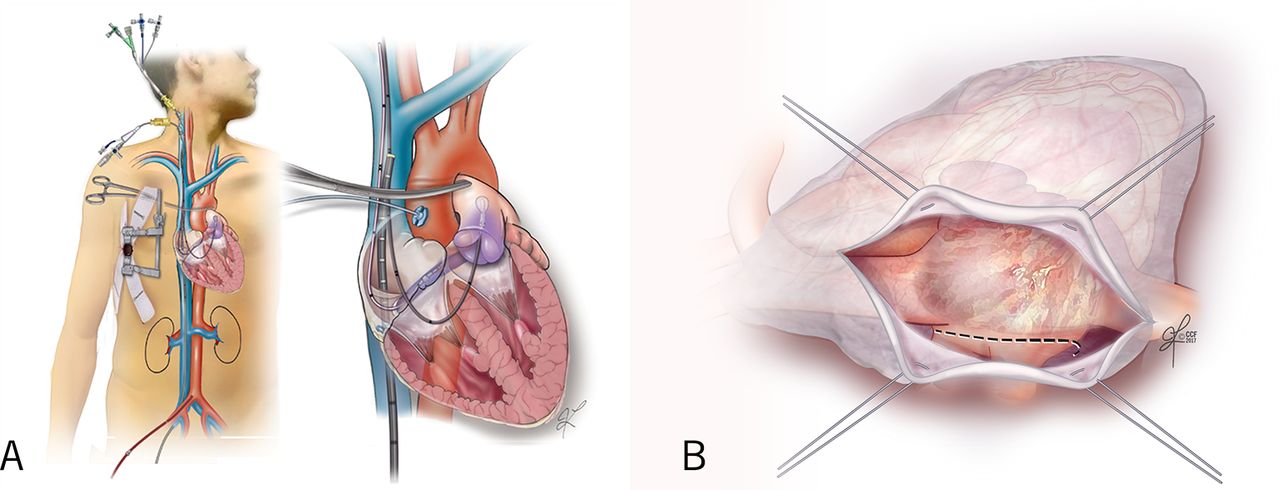
Patient setup. (A) Transthoracic clamp. (B) Left atriotomy.
Anterolateral right mini-thoracotomy approach
As in the robotic approach, the patient is intubated with a double-lumen endotracheal tube, and standard monitoring lines are placed. In the right mini-thoracotomy, an anterolateral working port (4–6 cm) is made along the infra-mammary crease lateral to the nipple and through the right fourth ICS. The procedure is performed under direct visualisation or with the aid of an endoscopic camera, and long-shafted instruments are employed. A fixed left atrial blade retractor is introduced into the right side of the chest through the working port and connected to a 2 mm shaft penetrating the chest wall in the fourth ICS, just lateral to the right internal thoracic artery (figure 4). Cardiopulmonary bypass is initiated using right femoral artery and vein cannulation; the endoballoon or thransthoracic clamp is used to occlude aorta. The left atriotomy is made as discussed above.
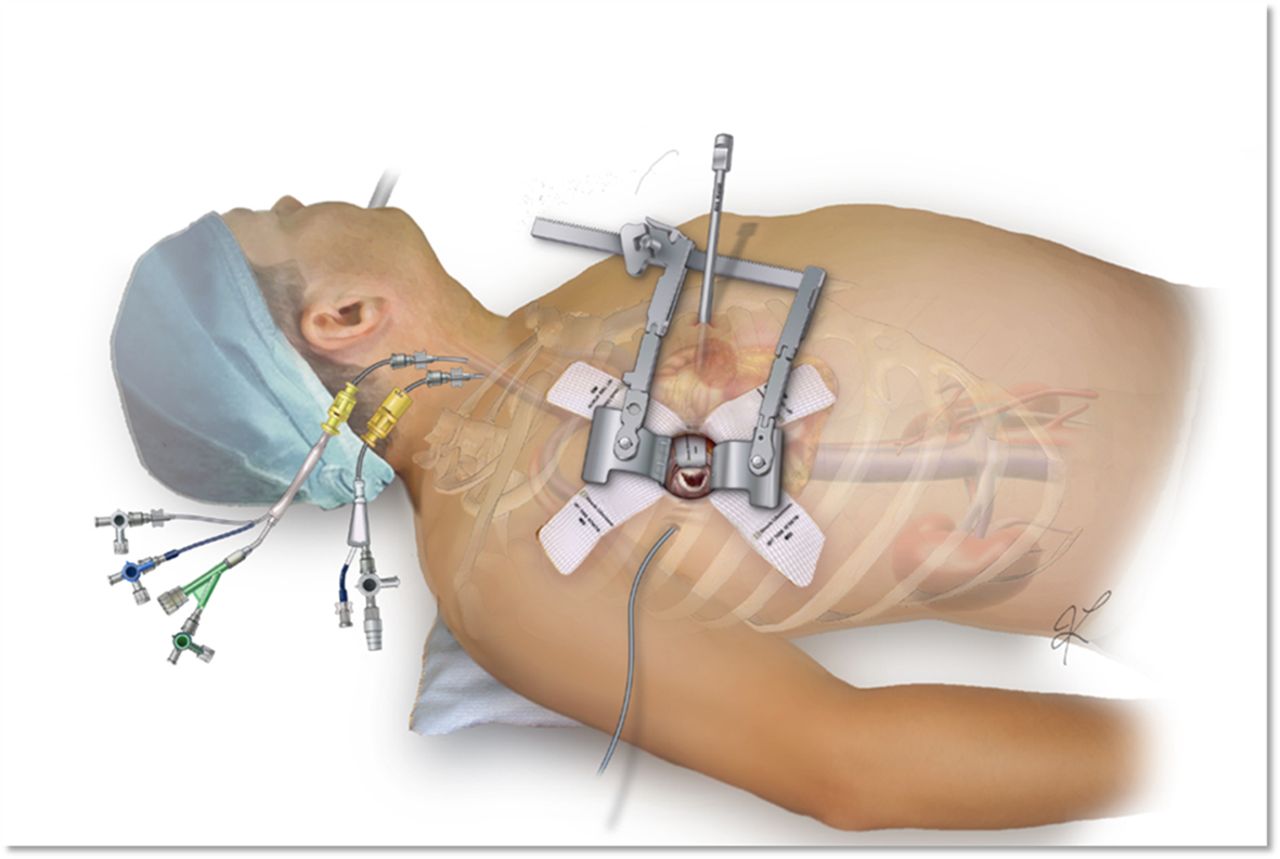
Mini-thoracotomy working port.
Minimally invasive MV repair
MV repair techniques are similar for robotic and right mini-thoracotomy approaches.
Triangular resection
This technique is ideal for patients with posterior leaflet prolapse. The MV is exposed, and the normal chordae on either side of the prolapsing portion are identified to determine the extent of resection. A triangular-shaped segment of tissue is excised with a curved scissor (figure 5A). Running 4–0 polypropylene suture (figure 5B) with or without a ventricularisation technique17 is used to close the defect in the leaflet.

MV repair techniques. (A) Triangular resection of the posterior leaflet. (B) Posterior leaflet repair using running technique. (C) Repair of the posterior leaflet using ventricularisation technique. (D) Running closure of the posterior defect. (E) Final stitch next to the annulus.
In the ventricularisation technique, each needle of a double-armed suture is passed through the free edge of one leaflet remnant and then through the mid-portion of that leaflet segment to ‘ventricularise’ (ie, move closer to the ventricle) the free edge, thereby reducing the leaflet height (figure 5C). Each needle is then used for a running closure of the posterior leaflet defect (figure 5D), and the stitch is tied at the base of the resection (figure 5E).
Quadrangular resection with sliding repair
A quadrangular resection of the posterior leaflet is employed for management of extensive, redundant posterior leaflet prolapse. The prolapsing, excessively tall segment of posterior leaflet is excised, and then the remaining portions of posterior leaflet are detached from the annulus and advanced centrally, ‘sliding’ them over, to meet. The leaflet base is reattached to the annulus with running 4–0 polypropylene, and the leaflet edges are reapproximated.
Neochordae implantation
Polytetrafluoroethylene (PTFE) neochordae placement is facilitated by the robotic approach and is particularly useful for treatment of anterior leaflet prolapse. The anterior leaflet is lifted upward using the dynamic left atrial retractor. The neochordae are created using 5–0 PTFE suture. One arm of the suture is passed twice through the fibrous tip of the papillary muscle, then twice through the free edge of the corresponding prolapsing segment. The second suture arm is then passed twice through the free edge of the prolapsing segment. The length of the chordae is adjusted based on (1) the height of the nearest normal segment of the leaflet, (2) shorter than elongated chords and (3) in a position which puts edge of MV leaflet at the level of mitral annulus. The suture is tied on the atrial side of the MV leaflet (figure 6).

Repair of the mitral valve using artificial chordae.
Annuloplasty
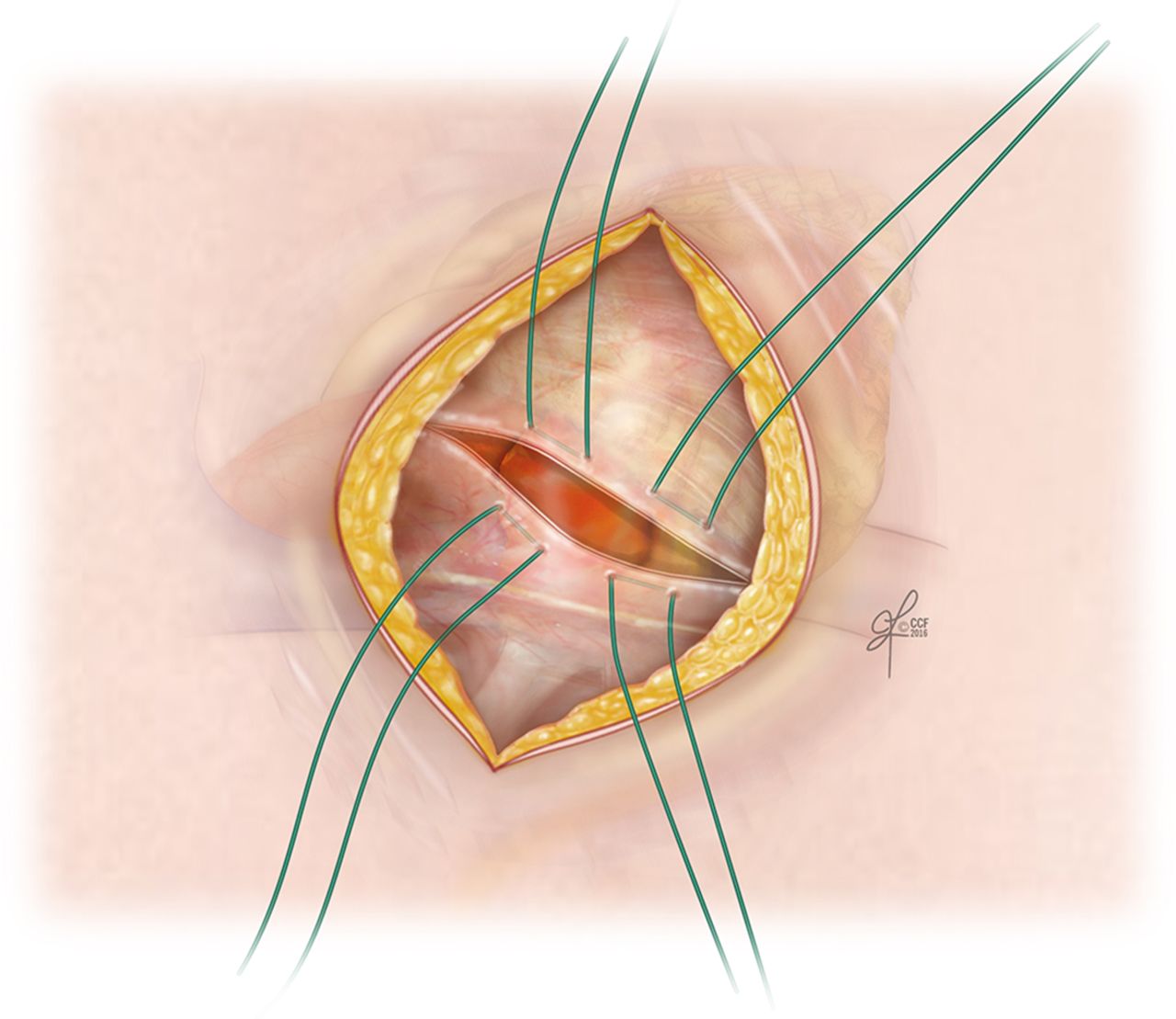
All repairs are completed using a flexible, standard-length annuloplasty band (63 or 65 mm). The band is first secured at the right (medial) trigone, and additional sutures are placed from the medial to the lateral part of the annulus using either running18 or interrupted technique.
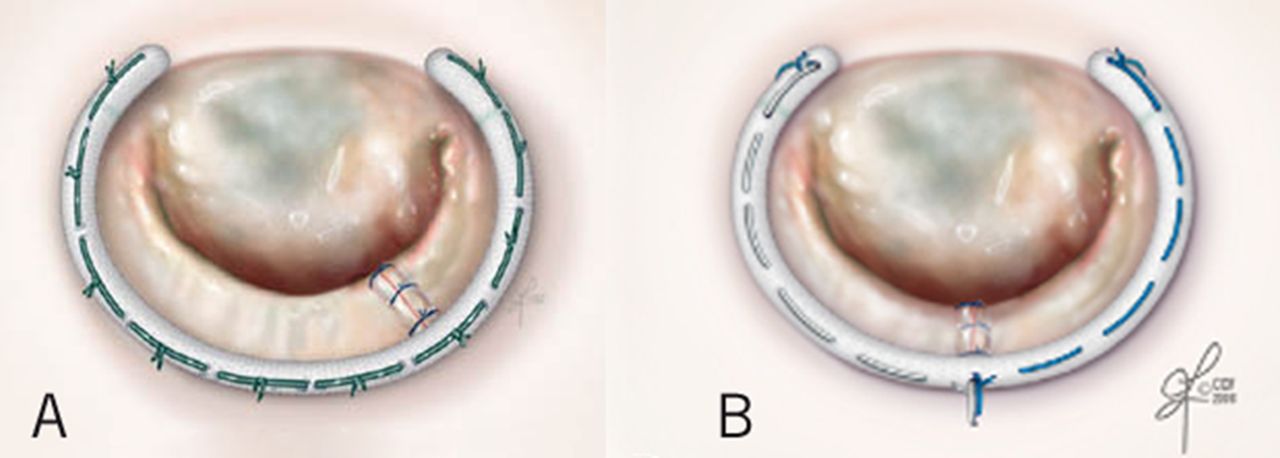
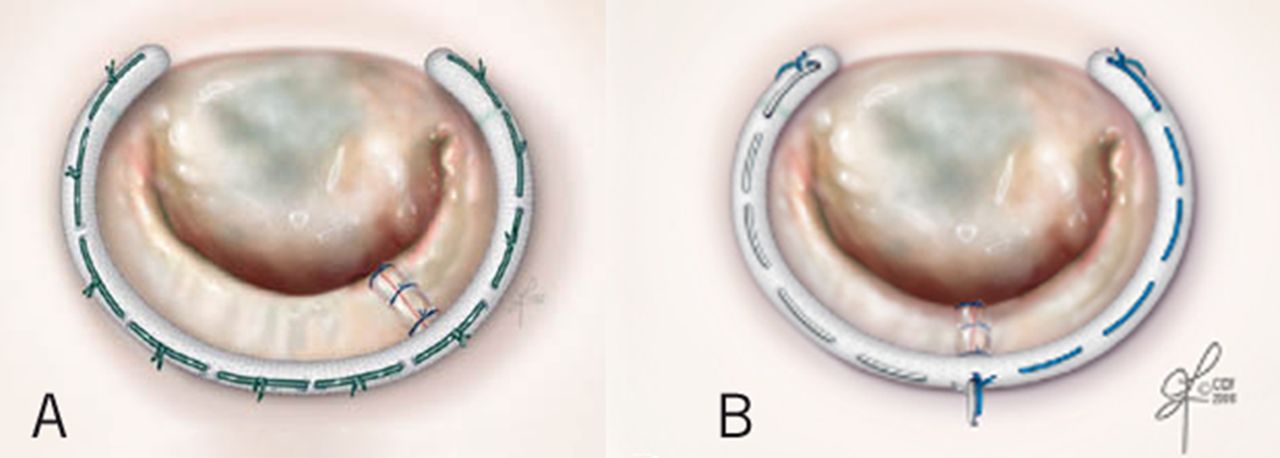
For the interrupted suture technique, 2–0 braided polyester sutures are used to secure the annuloplasty ring in standard fashion (figure 7A). For the running suture technique, three 2–0 braided polyester sutures (Ticron, Covidien, Massachusetts) are used to secure the annuloplasty ring as follows. The first suture is tied down between the right trigone and the ring and run clockwise to the midportion of the ring. The second suture is started at this point with a single interrupted stitch and tied to the first suture. The remainder of the second suture is then run clockwise to the left trigone. The third suture (9 cm in length) is passed through the ring, through the left trigone and then back through the ring. This third suture is tied down, and the tail is used to secure the second suture (figure 7B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Band annuloplasty. (A) Interrupted stitch. (B) Running stitch.
Final steps
All repairs are assessed using saline insufflation to fill and pressurise the left ventricle before closure, de-airing and cross-clamp removal. Integrity of the repair (≤+1 residual MR) and adequacy of de-airing should be confirmed with the patient off cardiopulmonary bypass before decannulation. Once the heart is beating (and preliminary evaluation of the repair by TOE is satisfactory), the antegrade cardioplegia catheter is removed from the aorta, and the puncture site is closed.
The pericardium is loosely approximated with two sutures to prevent cardiac torsion.19 A 19-Fr Blake drain (Ethicon, Johnson & Johnson) is brought into the chest via the right instrument port. The instruments and ports are all removed, and both lungs are ventilated. The patient is then separated from cardiopulmonary bypass, and the repair is evaluated by TOE. If MR is more than mild or there is significant SAM that does not resolve with medical therapy, we would (1) study the echocardiogram to determine the mechanism of dysfunction and (2) return to full cardiopulmonary bypass and rearrest the heart to correct the dysfunction. It is rare to have to perform a sternotomy in these instances. While protamine is administered, the cannulas are removed, the purse-string in the femoral vein is tied and the femoral arteriotomy is repaired primarily. After protamine is administered, the right lung is deflated, and the camera is reintroduced into the chest to examine the aortic cardioplegia site, as well as all port sites to ensure good hemostasis. All patients undergo TTE before discharge from hospital. It is our practice to recommend lifelong annual echocardiographic surveillance after MV repair.20–23 If severe MR recurs, we wish to reoperate before the patient develops adverse sequelae like left ventricular dysfunction or atrial fibrillation.
Published outcomes
The common goal of all minimally invasive MV repairs is developing a procedure at least equal to the gold standard ‘sternotomy’ technique. Important principals are maintaining the same indications for MV repair, upholding the technical and safety standards of sternotomy and successful elimination of significant MR.24 Safety and effectiveness of minimally invasive approaches have been facilitated by modifications in perfusion technology, intraoperative TOE and novel repair techniques.7 25 26 Recently, the Society of Thoracic Surgeon’s adult cardiac surgery database demonstrated that the application of less invasive MV surgery has increased from 11.9% of cases in 2004 to 20.1% in 2008 across the USA.27
Several studies have documented the benefits of mini-thoracotomy MV repair including faster extubation,28 29 less postoperative pain,24 30 bleeding and transfusion,31 better cosmetic results and shorter duration of intensive care unit and hospital stay,26 while hospital cost and long-term survival and durability of repair were similar to the sternotomy approach.32–34 Furthermore, although cross-clamp and operative times are longer in some studies compared with conventional median sternotomy, there has been no compromise in operative safety and efficacy.
Lack of tactile feedback has not been a limitation in practice. Highly disciplined movement of robotic instruments, advanced echocardiographic imaging and gaining ‘ocular tactility’ through experience have addressed this issue. There are several potential advantages of robotic MV repair in comparison to mini-thoracotomy approaches. The robot facilitates precise movements of instruments in the closed chest and avoids the difficulties associated with using long-shafted endoscopic instruments. The high-definition 3D view facilitates visualisation of the subvalvular apparatus and enables repair of any type of myxomatous pathology.
The collective results of robotic MV repair in experienced groups include a hospital mortality rate of <0.9%, stroke rate of 0.6%–1.7%, re-exploration for bleeding of <2.2%–4.7% and rare chest wall infections.35–40 Furthermore, the incidence of iatrogenic aortic dissection, phrenic nerve palsy and groin infections have all decreased to near 0%.40
Conclusion
Development of any new surgical skill has three phases: (1) cognition (identifying choice of operation), (2) integration (guided learning with iterative feedback) and (3) autonomy (skill refinement).41 Team learning effectiveness varies among institutions for minimally invasive cardiac surgery,42 and efforts should be made to emphasise on technique consistency, effective communication, team stability, explicit reflection and team empowerment from the outset. As team becomes faster and more comfortable, more complex procedure can be performed with less error, better patient care and more efficient resource utilisation. Proper planning and commitment including conservative approach permit surgeons to progressively gain experience without compromising procedural success, effectiveness or patient safety.21
Mini-thoracotomy and robotic MV repair are now routinely performed with or without concomitant tricuspid valve repair and atrial fibrillation ablation procedures.7 36 These approaches are safe, effective and durable for complete correction of MV prolapse, regardless of complexity. Furthermore, both techniques offer reduced blood loss, lower risk of incisional infection and atrial fibrillation, shorter hospital length of stay, quicker return to normal activities and a superior cosmetic result.7 38 43 44
Key messages
The 2017 American College of Cardiology/American Heart Association guidelines recommend (class IIa) early correction of mitral regurgitation (MR) in stage C1 patients (severe asymptomatic MR with left ventricular ejection fraction >60% or left ventricular end-systolic diameter <40 mm) if mortality risk is <1% and rate of repair is >95%.
Mini-thoracotomy and robotic mitral valve (MV) repair, with or without concomitant tricuspid valve repair and atrial fibrillation ablation procedures, are safe, effective and durable for complete correction of MV prolapse, regardless of complexity.
Minimally invasive techniques offer reduced blood loss, lower risk of incisional infection and atrial fibrillation, shorter hospital length of stay, quicker return to normal activities and a superior cosmetic result.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Acknowledgments
We would like to thank TM, SM and MYD for contributing their knowledge and expertise to this paper.
References
Footnotes
Contributors All coauthors contributed to all stages of this manuscript preparation.
Funding AMG receives research funding from St. Jude Medical and Tendyne.
Competing interests AMG is a consultant for CryoCath Technologies, Edwards Lifesciences, Medtronic, St. Jude Medical, Abbott Laboratories, and Atricure.
Provenance and peer review Commissioned; externally peer reviewed.
Author note References which include a * in the reference list have been identified as a key reference.