Article Text

Statistics from Altmetric.com
For symptomatic patients presenting with chronic severe, primary mitral regurgitation, American College of Cardiology/American Heart Association guidelines recommend surgical mitral valve repair for those with ejection fraction ≥30% or consideration of transcatheter mitral valve repair (TMVR) for those with prohibitive surgical risk.1 2 Contemporary clinical trial evidence also suggests benefit of TMVR for patients with heart failure and moderate-to-severe or severe secondary mitral regurgitation who remain symptomatic despite optimal medical therapy.3
As such, clinicians are often on the lookout for patients with mitral regurgitation and subjective complaints of dyspnoea, fatigue, palpitations as well as objective findings including decreased exercise capacity, elevated left atrial pressure (LAP), elevated pulmonary pressures, atrial fibrillation and/or the presence of abnormal biomarkers including brain natriuretic peptide to inform clinical decision-making.2 In a young, otherwise healthy patient without multisystem disease and multiple concordant clinical and imaging findings consistent with haemodynamically significant mitral regurgitation, decision-making is generally clear-cut. More often than not, clinicians are faced with a nuanced picture involving an older patient with comorbid disease and/or discordant imaging findings. Whether these patients have symptoms of mitral valve regurgitation or some other physiological derangement may not be readily obvious. To what extent these individuals will benefit from mitral valve intervention to reduce mitral regurgitant volume may be equally challenging using contemporary clinical practice recommendations for guidance.
The challenges inherent to evaluating and treating patients presenting with mitral regurgitation are highlighted in the accompanying publication by Sims and colleagues.4 They retrospectively compare a cohort of 31 patients with normal LAP (mean 10.5 mm Hg) to 173 patients with elevated LAP (mean 19 mm Hg) who underwent TMVR for treatment of mitral regurgitation. While the mean effective regurgitant orifice area was less in patients with normal LAP (0.40 cm2 vs 0.47 cm2, p=0.02), most patients nevertheless had severe mitral regurgitation (71.0% normal LAP vs 76.9% elevated LAP, p=0.48). One-year mortality was higher in the normal LAP cohort (32.3% vs 12.7%, p=0.006) despite paradoxically longer baseline 6 min walk distance (6MWD; 352 m vs 297 m, p=0.04) and lower mean New York Heart Association (NYHA) class (2.9 vs 3.2, p=0.04). The authors note a higher incidence of chronic lung disease among patients with normal LAP (45.2% vs 17.3%, p<0.001) which in turn may explain the observed increase in 1-year mortality and lower likelihood of benefit from TMVR.
Before drawing conclusions about these observations, we must acknowledge several limitations of the study. Beyond the inherent limitations of any retrospective analysis, the assessment of mitral regurgitation is often difficult owing to dynamic changes in loading conditions and is prone to subjectivity based on clinical suspicion. We must also assume that the two groups had comparable reductions in mitral regurgitant volume post-procedure, a variable which is difficult to assess. While post-procedure quantitative data are not available, we are presented with qualitative data suggesting similar rates of procedural success including comparable rates of residual severe mitral regurgitation (25.8% vs 33.0%, p=0.43) and follow-up mean NYHA class (1.8 vs 1.7, p=0.54).
Are we to conclude that patients in the normal LAP cohort did not benefit from TMVR simply because they had severe underlying lung disease driving their symptoms and in turn an increased risk of non-cardiac death compared with the elevated LAP cohort? Should we look for alternate causes of dyspnoea when mitral regurgitation severity and LAP appear discordant? Is LAP simply a marker of mitral regurgitation severity? In fact, the authors provide a nuanced haemodynamic assessment offering insight to these questions and prompting us to explore the role of left atrial compliance in mitral regurgitation.
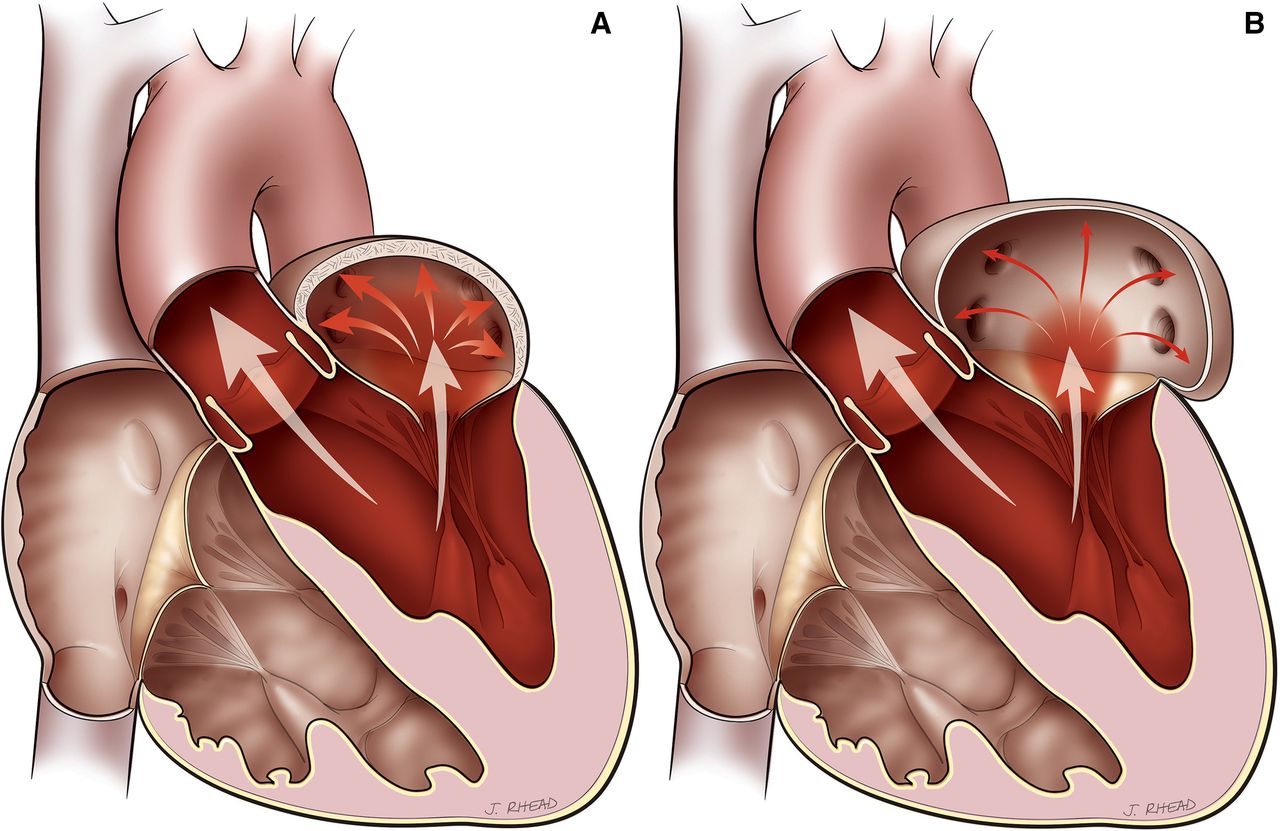
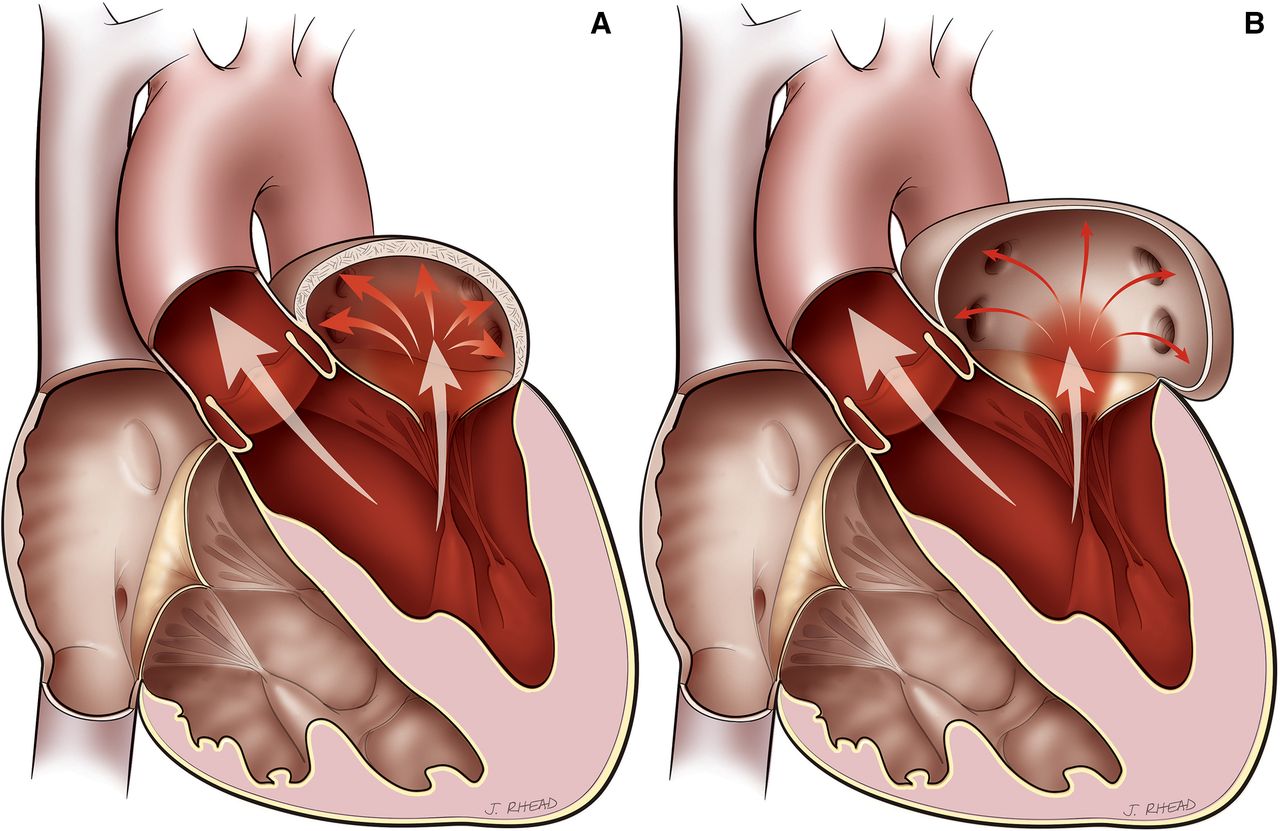
Compliance is the proportionate change in volume relative to change in pressure (figure 1). Patients with less compliant left atria have a relatively greater increase in pressure with increasing volume load. Conversely, patients with more compliant left atria have a relatively smaller increase in pressure with increasing volume load. Sims and colleagues make several interesting observations suggesting key differences in left atrial compliance between the two study cohorts which may in turn predict long-term benefit of TMVR in patients with comorbid disease. Patients with normal LAP were noted to have smaller mean V waves (16.5 mm Hg vs 32.5 mm Hg, p<0.0001) as well as a lower V wave to systolic blood pressure ratio (0.16 vs 0.30, p<0.0001) consistent with a more compliant left atrium. Second, patients with elevated LAP had a higher baseline incidence of atrial fibrillation (45.2% vs 65.9 %, p=0.03) which may also serve as a marker of decreased left atrial compliance. Following TMVR, there was a greater reduction in LAP in the elevated LAP cohort (1.9 mm Hg vs 2.8 mm Hg, p=0.08) again consistent with differences in left atrial compliance which clinically translated into a greater increase in 6MWD at 30 days (−3.6 m vs +25 m, p=0.11), although these observations did not meet statistical significance in this relatively small sample size.
{kind=link}
(A) Non-compliant (ie, small, fibrotic) LA with severe mitral regurgitation associated with increased LA pressure. (B) Compliant (ie, large, elastic) LA with severe mitral regurgitation associated with minimally increased LA pressure. LA, left atrium.
While cardiologists are well versed in the methods of assessing haemodynamic loading conditions and mitral valve regurgitation severity, an oft overlooked variable of the disease is assessment of left atrial compliance. Data presented by Sims et al, suggest that left atrial compliance, in addition to mitral regurgitant volume, may play a critical role in predicting which patients benefit from mitral intervention. A multitude of clinically relevant questions warrant further investigation: To what extent does left atrial compliance (or lack thereof) modify the natural history of mitral regurgitation? Can we develop standardised methods for assessment of left atrial compliance? How should left atrial compliance and LAP affect the manner in which we assess/treat mitral regurgitation? What impact will novel left atrial therapies including left atrial radiofrequency ablation, left atrial appendage occlusion and/or ligation have on left atrial compliance and concurrent mitral regurgitation?
A necessary caveat of personalised medicine is recognising that not all patients with seemingly similar problems will benefit from the same treatment. As such, we must tailor our therapies based on data and sound clinical judgement.
Acknowledgments
The authors thank medical illustrator Jill Rhead for the creation of Illustration 1.
Footnotes
Contributors All authors have made substantial contributions to the conception or design of the work, have together drafted and revised for important intellectual content, and provided final approval. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.