Article Text

Statistics from Altmetric.com
Since the outbreak of the pandemic until early 2022, SARS-CoV-2 infection (COVID-19) has affected more than 410 million individuals worldwide, and of those almost 5.9 million people have died. COVID-19 mortality is strongly associated with advanced age, comorbidities, thromboembolism and vaccination status (www.COVID-19.who.int). Atrial fibrillation (AF) is the most common sustained arrhythmia. Globally, more than 37 million patients have AF, and its prevalence is forecasted to increase more than twofold by 2060.1 Mortality in patients with AF is closely related to the same comorbidities as in COVID-19 including congestive heart failure (CHF) and thromboembolic complications. The risk of AF is elevated among patients with COVID-19, and vice versa.2
In the study published in this issue of Heart, Handy et al evaluated antithrombotic use and the impact of various antithrombotic agents on the outcomes of patients with AF and COVID-19.3 Using routinely updated, linked population-scale electronic health records for 56 million people in England, they found 972 971 individuals with AF and CHA2DS2-VASc score ≥2. Due to the massive sample size, it was possible to control for a wide range of confounding variables without losing statistical power.
AF and COVID-19: a potentially lethal combination
AF and COVID-19 are a common and potentially lethal combination. AF is independently associated with a 1.5-fold to 2-fold increase in all-cause death,1 and although most people with coronavirus infection will develop mild to moderate illness, COVID-19 has been associated with excess mortality. That is, during the pandemic, the number of deaths has been above and beyond what we would have expected under normal conditions (www.COVID-19.who.int). In a scenario where someone has both AF and COVID-19, the prognosis is even worse. Handy et al reported that 3.8% of patients with AF had COVID-19-related hospitalisation and 2.2% of them died. Concurrent AF has been associated with a fourfold increased risk of all-cause death and fivefold greater chance of developing critical COVID-19.2
The CHA2DS2-VASc score is widely used to predict the risk of stroke and systemic emboli in patients with AF. The main components in the risk calculator include age, CHF, hypertension, vascular disease, diabetes and prior thromboembolic events. Since severe COVID-19 infection is commonly associated with venous thromboembolism (VTE), pulmonary embolism (PE), and possibly also with stroke or transient ischaemic attack, it is likely that COVID-19 and AF are synergistic risk factors for poor outcome, and the CHA2DS2-VASc score may underestimate risk of stroke during COVID-19 infection.
Mechanisms of the thromboembolic complications
AF and COVID-19, both high-risk thrombotic disorders, have been associated with the activation of thrombo-inflammatory pathways (figure 1). During AF, aberrant blood flow in the left atrial appendix triggers activation of coagulation and formation of fibrin which can be detected with biomarkers indicating thrombin generation (e.g., D-dimer). Several studies have demonstrated that an elevated D-dimer level is associated with the presence of atrial thrombosis and correlates with the degree of hypercoagulability and thromboembolic risk in patients with AF.4 COVID-19enhances the thrombo-inflammatory cascade, which intensifies coagulation and may increase the risk of cardiac embolism in patients with AF.

SARS-CoV-2 virus and atrial fibrillation both activate thrombo-inflammatory interactions at the vulnerable vascular sites. COVID-19 activates inflammatory cells and damages the endothelium exposing collagen. Platelets adhere to these sites via von Willebrand factor (VWF) and collagen, generating thrombin. Thrombin converts soluble fibrinogen to fibrin to stabilise the thrombus. Platelet–neutrophil interactions perpetuate these processes by releasing neutrophil extracellular traps (NETosis). During atrial fibrillation, the main trigger of the thrombo-inflammatory cascade is aberrant blood flow in the left atrial appendix. IL-1β, interleukin 1β; PF4, platelet factor 4; TF, tissue factor.
In the beginning of the pandemic, it was anticipated that coronavirus infection caused a disseminated intravascular coagulation (DIC). Before long it was shown that DIC is rare; rather the hallmarks of coronavirus infection are cytokine storm, loss of protective vascular endothelial glycocalyx, microvascular inflammation, platelet activation, deposition of platelets and fibrin in multiple organs, and increasing levels of fibrinogen.5 Elevated von Willebrand factor, factor VIII, and in particular D-dimer levels, associate with poor outcome in patients with COVID-19. Most strikingly, high initial levels (>4 mg/L) and progressively increasing D-dimer values have been associated with up to 20-fold to 50-fold enhanced risk of mortality.6
COVID-19: another reason for anticoagulation in patients with AF
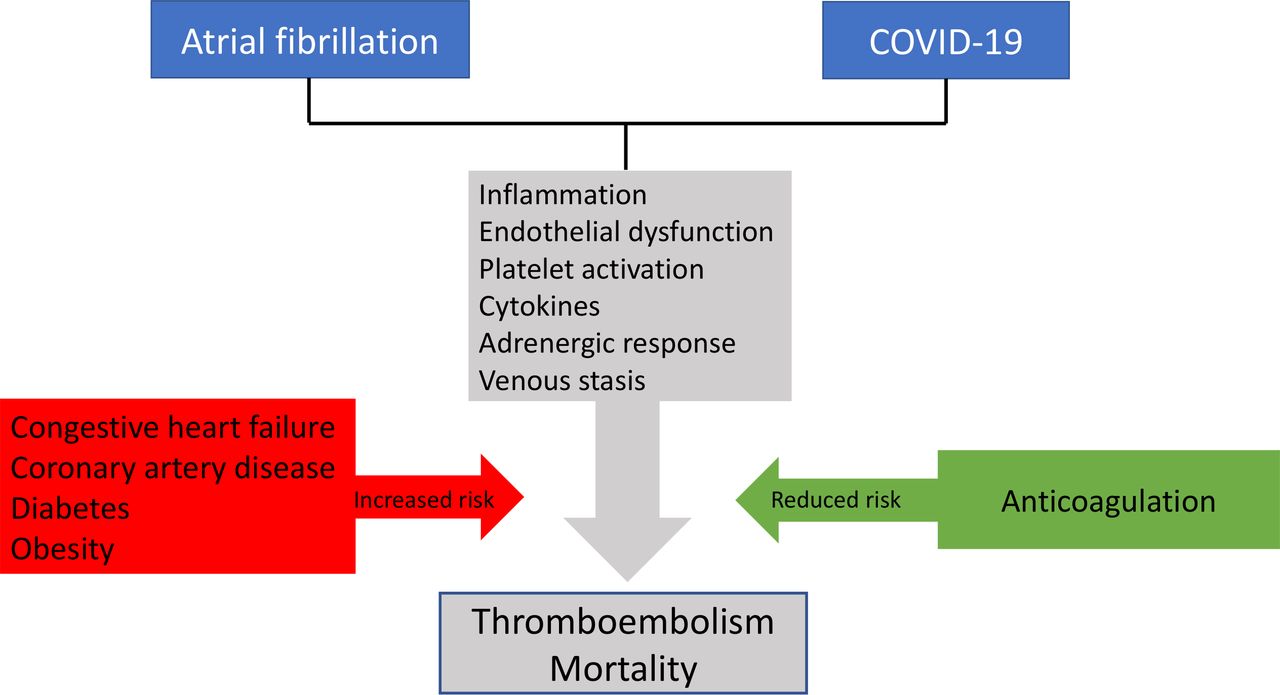
Thromboembolic complications have a substantial impact on morbidity and mortality in patients with AF and coronavirus infection, and the use of anticoagulants has been shown to improve outcome in both diseases (figure 2). In patients with AF, vitamin K antagonists (VKAs) compared with placebo reduce the risk of stroke by 64% and mortality by 26%, and direct oral anticoagulants (DOACs) may provide even greater protection against thromboembolism.1 In the beginning of the COVID-19 pandemic, the incidence of VTE and PE in hospitalised patients was about 30%; since then, with better thromboprophylaxis, it has been reduced to 10-15 %.7

{kind=link}
{kind=link}
Atrial fibrillation (AF) and COVID-19 infection are synergistic high-risk thrombotic disorders, which are associated with the activation of thrombo-inflammatory pathways. Congestive heart failure, coronary artery disease, diabetes and other comorbidities increase the risk of thromboembolism and mortality, while anticoagulation reduces the risk of thrombus formation and improves survival. Optimisation of the management of all modifiable comorbidities alleviates thrombo-inflammation and improves outcome both in AF and COVID-19.
Handy et al showed that in patients with concurrent AF and COVID-19, the use of any antithrombotic medication was associated with marginally lower odds of death (2.1% vs 2.5%), and foremost the survival rate was higher among patients using OAC than in those taking antiplatelets (APs). This is in line with prior data indicating that the OACs are more effective than APs in preventing thromboembolism not only in patients with AF1 but also in patients with COVID-19.
Despite the mortality benefit, the use of OAC did not reduce hospitalisation. Quite the reverse, hospitalisation was somewhat less frequent among patients using no antithrombotics than in those using antithrombotic medication. Although the specific reason(s) for the difference in the hospitalisation rate are uncertain, we agree with the authors that this may reflect greater awareness and health-seeking behaviour among OAC-using patients and/or more cautious attitude among the physicians managing them.
In the current study, only patients with CHA2DS2-VASc ≥2 were included, and the impact of therapeutic OAC in patients with only one risk factor or no risk factors was not studied. It is possible that some patients with AF with COVID-19 may benefit from therapeutic anticoagulation despite low CHA2DS2-VASc score. Hopefully, this issue will be addressed in future studies.
Antithrombotic agents are not equal
There is striking difference between anticoagulants and AP agents. Anticoagulants are used for conditions that involve stasis, whereas APs are used for conditions that involve endothelial damage and platelets sticking to the injured site. Hence, it was understandable that OAC provided better protection against death in patients with AF with COVID-19 than did APs.
VKAs have a broad inhibitory mode of action on vitamin K-dependent coagulation factors. On initiation, VKAs, unlike DOACs, are inherently prothrombotic because they inhibit the natural anticoagulant proteins C and S faster than modulating the coagulation factors. Nevertheless, Handy et al observed no significant difference in mortality between patients using VKAs and DOAC.3 However, the COVID-19 hospitalisation rate was marginally elevated in patients with pre-existing VKA versus DOAC therapy. Potential explanations to this observation are the complex pharmacological characteristics and narrow therapeutic window of warfarin, many drug–drug and drug–food interactions, and need for regular coagulation monitoring and dose adjustments. The finding that the direct thrombin inhibitor dabigatran was associated with lower odds of death compared with the factor Xa inhibitors was appealing, but it needs to be confirmed in other large-scale studies before any recommendation on specific DOAC for patients with COVID-19 can be made.
The best evidence of the benefits of anticoagulation in patients with COVID-19 has been offered by low-molecular-weight heparin (LMWH). Early initiation of LMWH at a thromboprophylaxis dose versus no LMWH leads to a 40% reduction in COVID-19 mortality. In addition, in non-critically ill patients hospitalised with COVID-19, therapeutic dose of LMWH increased the probability of survival and reduced the need for cardiovascular or respiratory organ support compared with usual thromboprophylaxis. However, in critically ill patients with COVID-19, it did not provide any survival benefit compared with normal thromboprophylaxis.8 Hence, the net effect of OAC on the clinical outcome appears to depend on the timing of the medication. That is, pre-existing use or early initiation of OAC may protect from severe COVID-19, while after severe COVID-19 illness has already developed OAC initiation may be too late and can no longer alter the progression of the disease.
Take home message
In the light of these and prior findings, it is obvious that COVID-19 is a dangerous disease in patients with AF and vice versa. While not evidence of causality, the data by Hardy et al imply that anticoagulation may play an important prognostic role in patients with AF with COVID-19. Although better than in most prior studies, the use of OAC in the study cohort was still suboptimal as only about 80% of the patients with CHA2DS2-VASc score ≥2 used OAC. On the other hand, current data offered no information concerning the role of OAC in patients with AF with COVID-19 who had only one or no CHA2DS2-VASc points. Finally, we need to bear in mind that VKA and DOAC dosing is challenging in patients with acute infection due to enhanced coagulation activity, and a switch to LMWH may be beneficial to optimise the safety and effectiveness in patients progressing towards critical illness.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Contributors Both authors have been involved in writing the editorial and approved it.
Funding This study was funded by Finnish Foundation for Cardiovascular Research.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Cardiac risk factors and prevention