Article Text

Statistics from Altmetric.com
Degenerative aortic stenosis accounts for the majority of native valve disease.1 Surgical aortic valve replacement is a treatment option that provides good outcome in the majority of the patients, with good durability of the prosthetic valve.w1 However, a large proportion of patients with severe aortic stenosis are not referred for, or denied, surgery. The Euro Heart Survey on valvular heart disease demonstrated that up to 33% of the patients with severe aortic stenosis did not undergo surgery, although there was an indication.2 Patient’s age and (multiple) comorbidities were the main reasons for denial of surgery.w2 Therefore, there is a need for a less invasive treatment option in older patients with severe aortic stenosis.
In the past few years, new percutaneous aortic valve implantation procedures have been introduced.w3 Two different types of percutaneous aortic valve prostheses now have approval in Europe. In addition, European3 and American4 5 recommendations on percutaneous aortic valve implantation have been published.
In this article, the clinical experience with the two different percutaneous aortic valves will be reviewed. In addition, the role of different imaging modalities in the selection of patients, guidance during percutaneous aortic valve implantation, and follow-up will be discussed.
Prostheses and clinical experience
Currently, two different types of percutaneous aortic valve devices are commercially available. The balloon expandable Edwards SAPIEN valve (Edwards Lifesciences Inc, Irvine, California, USA) and the self expanding CoreValve Revalving prosthesis (CoreValve Inc, Irvine, California, USA). At present, more than 2500 patients worldwide have been treated with percutaneous aortic valve implantation, and the number of studies reporting the clinical experience and results with percutaneous aortic valve procedures is rapidly growing (table 1). In the following paragraphs, technical aspects of the different prostheses and clinical experience with percutaneous aortic valve implantations will be reviewed.
Overview of published reports to date on the results of percutaneous aortic valve implantation
Balloon expandable valve
Andersen et al first tested the balloon expandable percutaneous aortic valve in an animal model in 1992.6 Subsequently, Cribier et al performed the first human implantation in 2002.7 The first generation balloon expandable valve was entitled Cribier-Edwards valve (Edwards Lifesciences Inc), whereas at present the Edwards SAPIEN valve (Edwards Lifesciences Inc) is commercially available (fig 1). This prosthesis incorporates a balloon expandable stainless steel stent, fabric sealing cuff and bovine pericardial leaflets. At present, available prosthesis sizes are 23 and 26 mm for aortic annulus diameters between 18–22 mm and 21–25 mm, respectively.

Currently commercially available prostheses for percutaneous aortic valve implantation. Panel A shows the balloon-expandable Edwards-SAPIEN valve. Panel B shows the self expanding CoreValve prosthesis.
In the first studies, an antegrade implantation of the valve was performed, using transseptal access to the left atrium and passage through the mitral valve to reach the aortic valve.7 However, at present a retrograde approach through the femoral artery is used.8 During the procedure, a balloon valvuloplasty is first performed to facilitate passage of the native aortic valve. During rapid right ventricular pacing, the prosthesis is positioned and deployed under fluoroscopy and echocardiographic guidance. Alternatively, in patients with difficult vascular access because of extensive calcifications or tortuosity of the femoral artery or aorta, a transapical approach can be used. After a partial thoracotomy, direct puncture of the apical portion of the left ventricular free wall is performed to gain catheter access to the left ventricle and aortic valve. The prosthesis is subsequently positioned and deployed, similar to the antegrade approach.9
Clinical experience: Cribier-Edwards and Edwards SAPIEN valve
A single centre phase 1 project was started in 2003 for compassionate use of the Cribier-Edwards valve in patients with end stage aortic stenosis after the first successful animal and human studies. In the Initial Registry of EndoVascular Implantation of Valves in Europe (I-REVIVE) trial, followed by the Registry of Endovascular Critical Aortic Stenosis Treatment (RECAST) trial, a total of 36 patients (mean (SD) EuroSCORE 12 (2)) were included.10 11 Twenty-seven patients underwent successful percutaneous aortic valve implantation (23 antegrade, 4 retrograde). The 30 day mortality was 22% (6 of 27 patients), and the mean (SD) aortic valve area (AVA) increased from 0.60 (0.11) cm2 to 1.70 (0.10) cm2 (p<0.001). Importantly, this improvement in AVA was maintained up to 24 months follow-up.11
After these first trials, the Cribier-Edwards prosthesis and the Edwards SAPIEN prosthesis have been used in numerous studies (table 1). Overall, acute procedural success is achieved in 75–100% of the procedures, and 30 day mortality ranges between 8–50% in the published studies. In a large study using the retrograde approach, Webb et al treated 50 aortic stenosis patients (mean age 82 (7) years, 45 patients in New York Heart Association (NYHA) functional class III or IV).12 A Cribier-Edwards valve was successfully implanted in 43 of the 50 patients (86%). Interestingly, a clear learning curve was observed when comparing the first 25 patients with the second 25 patients. Procedural success increased from 76% in the first 25 patients to 96% in the second 25, and 30 day mortality fell from 16% to 8%.12 Recently, Walther et al reported their initial single centre experience with the transapical implantation of the Edwards SAPIEN valve in 50 high risk aortic stenosis patients.w4 Via an anterolateral minithoracotomy, the prosthesis was successfully implanted in 47 patients (94%); early conversion to conventional sternotomy had to be performed in three patients. Cardiopulmonary bypass was used in 16 patients (32%). After implantation, all prostheses showed good valvular function, with only mild aortic incompetence (mean aortic regurgitation grade 0.5 (0.5)). During the first 30 days postoperatively, four patients died and during follow-up another 10 patients died (overall survival at 12 months 71.4%). A post-hoc analysis of the first 25 patients versus the second 25 patients did not show a difference in long term survival after aortic valve implantation.w4
Importantly, a randomised trial (PARTNER: Placement of AoRTic traNscathetER valves) using the Edwards SAPIEN valve is currently comparing percutaneous aortic valve implantation against surgical aortic valve replacement (objective: demonstrating non-inferiority of the percutaneous prosthesis) and medical treatment (objective: demonstrating superiority of the prosthesis) (fig 2). The primary end point in the two arms is mortality at 12 months follow-up, with secondary end points that focus on long term adverse cardiovascular events composite, valve performance and quality-of-life indicators.w5 The results of this first randomised trial with percutaneous aortic valve implantations are eagerly awaited.

Flowchart of the randomised PARTNER trial. In the first treatment arm (surgical) the Edwards SAPIEN prosthesis is compared against standard surgical aortic valve replacement in 350 patients. The second arm (medical management) compares the Edwards SAPIEN valve against medical treatment and/or balloon valvuloplasty in 250 patients. The primary end point in the two arms is mortality at 12 months follow-up. Secondary end points include an adverse cardiovascular events composite, valve performance, and quality-of-life indicators. AVA, aortic valve area; AVR, aortic valve replacement; NYHA, New York Heart Association; STS, Society of Thoracic Surgeons.
Self expanding valve
The CoreValve Revalving system (CoreValve Inc) consists of a tri-leaflet bioprosthetic porcine pericardial tissue valve, mounted and sutured in a self expanding nitinol alloy stent (fig 1). The device is constrained within a delivery sheath, and expands to its predetermined shape when the sheath is withdrawn. It has a specific design consisting of three distinct parts. The lower portion of the prosthesis has high radial force to expand and avoid recoil. The middle portion includes the pericardial tissue valve and is constrained to avoid coronary occlusion. The upper part is flared to the centre and fixes the prosthesis in the ascending aorta. At present, the third generation CoreValve Revalving system is commercially available. The size of the delivery system has gradually declined from a 25 F and 21 F system (first and second generation, respectively) to the currently available third generation 18 F system. Two different sizes are currently available: a 26 mm prosthesis (aortic annulus diameter 20–24 mm) and a 29 mm prosthesis (aortic annulus diameter 24–27 mm). The CoreValve prosthesis is implanted retrogradely through the femoral artery. While in the first series the prosthesis was implanted under general anaesthesia with a cardiac assist device, extracorporeal membrane oxygenation or a full bypass support,13 at present local anaesthesia combined with mild systemic sedative/analgesic medication is used without cardiac assist or full bypass support.14 After balloon valvuloplasty, the device is positioned under fluoroscopy guidance. Retraction of the outer sheath allows deployment of the self expanding prosthesis. Postdilatation of the prosthesis can be performed if deemed necessary, depending on the position of the prosthesis and the presence of aortic regurgitation.14
Clinical experience: CoreValve Revalving system
Since the first implantation of the CoreValve prosthesis in a patient in 2005,15 a large number of patients have been treated with this device to date (table 1). In the first pilot study, Grube et al treated 25 patients with severe aortic stenosis deemed unsuitable for open heart surgery using first and second generation prostheses.16 Acute procedural success was achieved in 21 of 25 patients (84%). Major in-hospital cardiovascular and cerebral events occurred in eight patients (32%) whereas major bleeding occurred in five of 10 patients (50%) treated with the first generation device and in one of 15 patients (7%) treated with the second generation prosthesis. At 30 days follow-up, the mean (SD) aortic valve gradient decreased from 44.2 (10.8) mm Hg to 11.8 (3.4) mm Hg (p<0.001), and NYHA class improved from 2.9 (0.2) to 1.7 (0.5) (p<0.001).16
Recently, Grube et al reported the results with the three different generations of the CoreValve Revalving system.14 In this non-randomised, prospective study, a total of 136 patients were included. Ten patients were treated with first generation devices, 24 patients with second generation, and 102 patients with third generation devices. At baseline, mean AVA was 0.67 (0.9) cm2 and mean logistic EuroSCORE was 23.1 (15.0)% in the overall study population. Overall procedural success rate increased significantly with the new generation devices from 70.0% and 70.8% to 91.2% for the first, second, and third generation prostheses, respectively (p = 0.003). Interestingly, periprocedural mortality decreased using newer devices from 10% (first generation) to 8.3% (second generation) to 0% (third generation). Overall 30 day mortality for the three generations was 40%, 8.3% and 10.8%, respectively. Pooled data demonstrated a significant improvement in mean (SD) NYHA functional class (from 3.3 (0.5) to 1.7 (0.7), p<0.001), without a difference between the three generations. Importantly, NYHA functional class and mean pressure gradient remained stable up to 12 months follow-up in all three generations. This largest single centre experience with three generations of CoreValve prostheses demonstrates that the use of the latest generation prosthesis is associated with an improved procedural and mid term outcome.14
In addition, the results of a multicentre registry with the third generation CoreValve Revalving system have recently been reported.17 A total of 646 patients from 51 centres were included in the registry. It was a high risk elderly population (mean age 81 (7) years) with a poor functional class (85% of the patients in NYHA class III or IV), and a high logistic EuroSCORE (mean 23.1 (13.8)%). Procedural success was achieved in 628 of the 646 patients (97.2%). All cause 30 day mortality was 8%, and the combined end point of procedural related death, stroke or myocardial infarction was reached in 60 patients (9.3%). After successful implantation, mean pressure gradient decreased from 49 (14) mm Hg to 3 (2) mm Hg.17 This large registry confirms the results of earlier studies, and demonstrates the safety, feasibility and efficacy of the CoreValve Revalving system.
Valve-in-valve procedure
The concept of a percutaneous aortic valve implantation in an existing aortic valve prosthesis (“valve-in-valve”) has recently been introduced. The feasibility was demonstrated in an animal model by Walther et al.18 Afterwards, the valve-in-valve concept was successfully applied in patients with degenerated aortic bioprostheses.w6 w7 It may be of great value in these patients, since reoperation for degenerated xenografts is challenging, and is associated with an increased mortality risk as compared with first isolated aortic valve replacement.w8
Furthermore, the valve-in-valve concept can be used during first percutaneous CoreValve prosthesis implantation, in case of suboptimal implantation of the prosthesis.14 Good function of the prostheses and durability of the valve-in-valve has been demonstrated up to 3 years follow-up.w9 Recently, a multicentre study demonstrated that in up to 2.6% of first CoreValve prosthesis implantation procedures, a valve-in-valve procedure is performed.17 However, it should be performed with caution because future access to the coronary ostia may be limited by the two overlying nitinol frames of the prostheses.
Selection of patients
The selection of patients for percutaneous aortic valve implantation involves several critical steps. In general, a multidisciplinary team, including cardiologists, surgeons, anaesthetists and imaging specialists, should decide if patients are eligible for percutaneous aortic valve implantation. Recently, two position statements on the use of percutaneous aortic valve procedures have been published, that provide important information on the patient selection procedure.3 5 A summary of the European statement (endorsed by the European Association of Cardio-Thoracic Surgery and the European Society of Cardiology) is provided in table 2.
Recommendations on patient selection for percutaneous aortic valve implantation (adapted from Vahanian et al3)
One of the first steps in the selection procedure is the assessment of aortic stenosis severity. At present, percutaneous aortic valve implantation is only recommended in symptomatic patients with severe aortic stenosis. The surgical risk, life expectancy, and quality of life should also be assessed. Preferably, the surgical risk is determined using a combination of clinical judgement and multiple risk scores, such as the logistic EuroSCORE, the STS Predicted Risk of Mortality score, or Ambler score.3 When patients are deemed inoperable due to a high surgical risk, a percutaneous procedure can be considered.
Finally, the feasibility of a percutaneous procedure and contraindications should be assessed in the potential candidates (table 2). Typically, coronary anatomy, the aortic annulus, and the peripheral vessels are evaluated. For this purpose, various imaging modalities are available. These modalities and their relative merits will be reviewed.
Imaging in percutaneous aortic valve implantation
Various imaging modalities are available for the selection of patients, performing percutaneous aortic valve implantation, and for follow-up after the procedure. An overview on the role of various imaging modalities in percutaneous aortic valve implantation procedures is provided in table 3. Whereas transthoracic echocardiography (TTE), multislice computed tomography (MSCT), and magnetic resonance imaging (MRI) are valuable imaging techniques before and after the procedure, transoesophageal echocardiography (TOE) is mainly used during the actual implantation procedure.
The role of imaging in percutaneous aortic valve implantation procedures
Patient selection
The selection of candidates for percutaneous aortic valve implantation involves a number of critical steps. The different imaging modalities can assist in the selection process by providing important information on the aortic valve, coronary arteries, and vascular structures. First, the severity of aortic stenosis should be assessed. Both TTE and TOE are the preferred tools to assess the severity of aortic stenosis.1 However, recent reports have suggested a good correlation between echocardiography and both MSCTw10 and MRIw11 to assess AVA with planimetry.
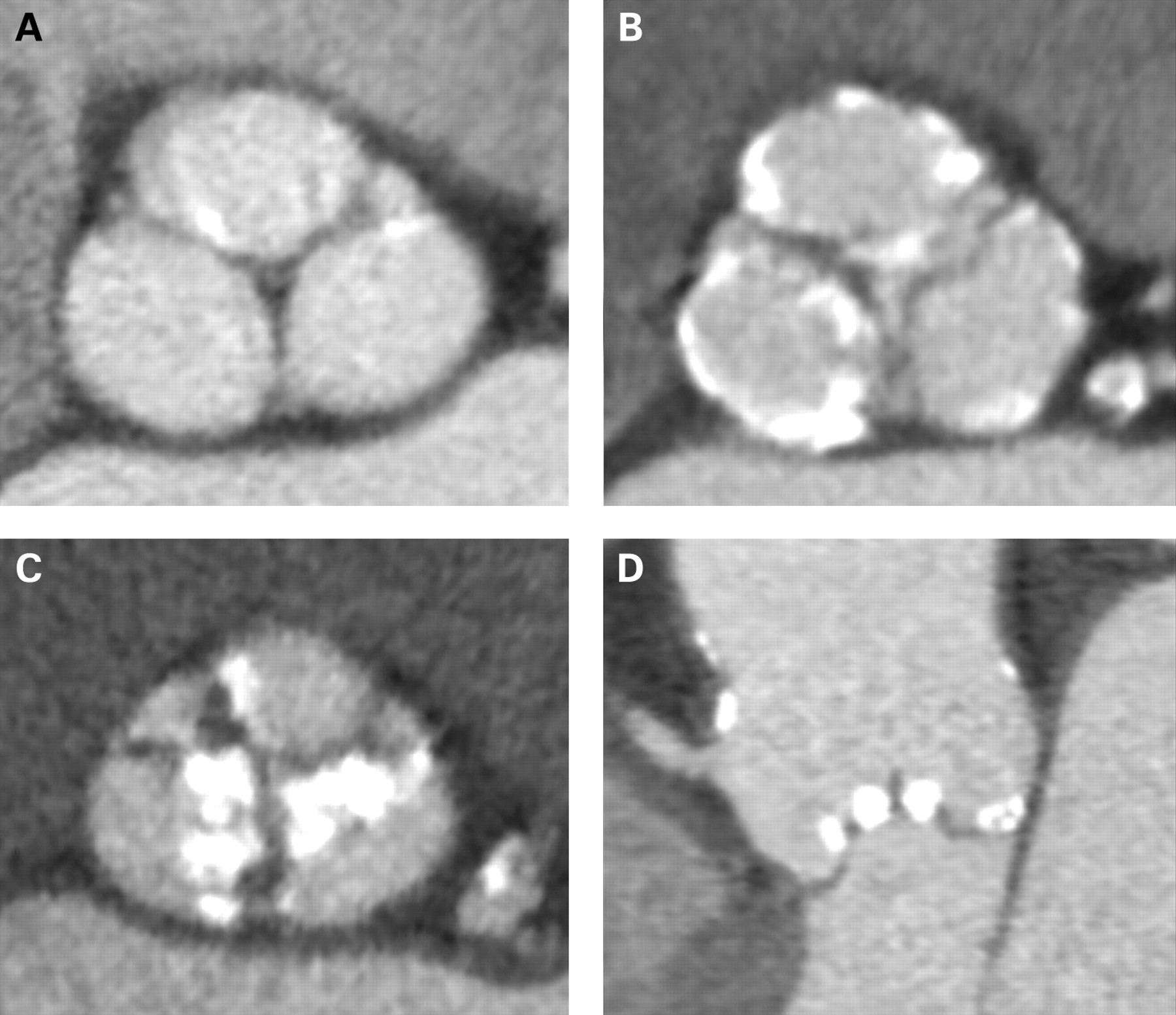
In addition, the exact anatomy of the aortic valve should be assessed. Echocardiography, MSCT and MRI can all help to distinguish between a bicuspid and a tricuspid aortic valve. It has been suggested that a bicuspid aortic valve may result in a higher incidence of stent misdeployment and peri-stent leakage.19 Therefore, at present it is not recommended to perform percutaneous aortic valve implantation in bicuspid aortic valve.3 Furthermore, the exact location and severity of aortic valve calcifications and the presence of bulky aortic valve leaflets should be assessed. Before the implantation procedure, MSCT may be the preferred tool to identify aortic valve calcifications.14 A severely calcified aortic valve may result in the inability to cross the native valve with the catheter. Bulky leaflets and calcifications on the free edge of the leaflets may increase the risk of occlusion of the coronary ostia during aortic valve implantation.12 Therefore, the extent and exact location of calcifications should be carefully assessed before the implantation procedure (fig 3).
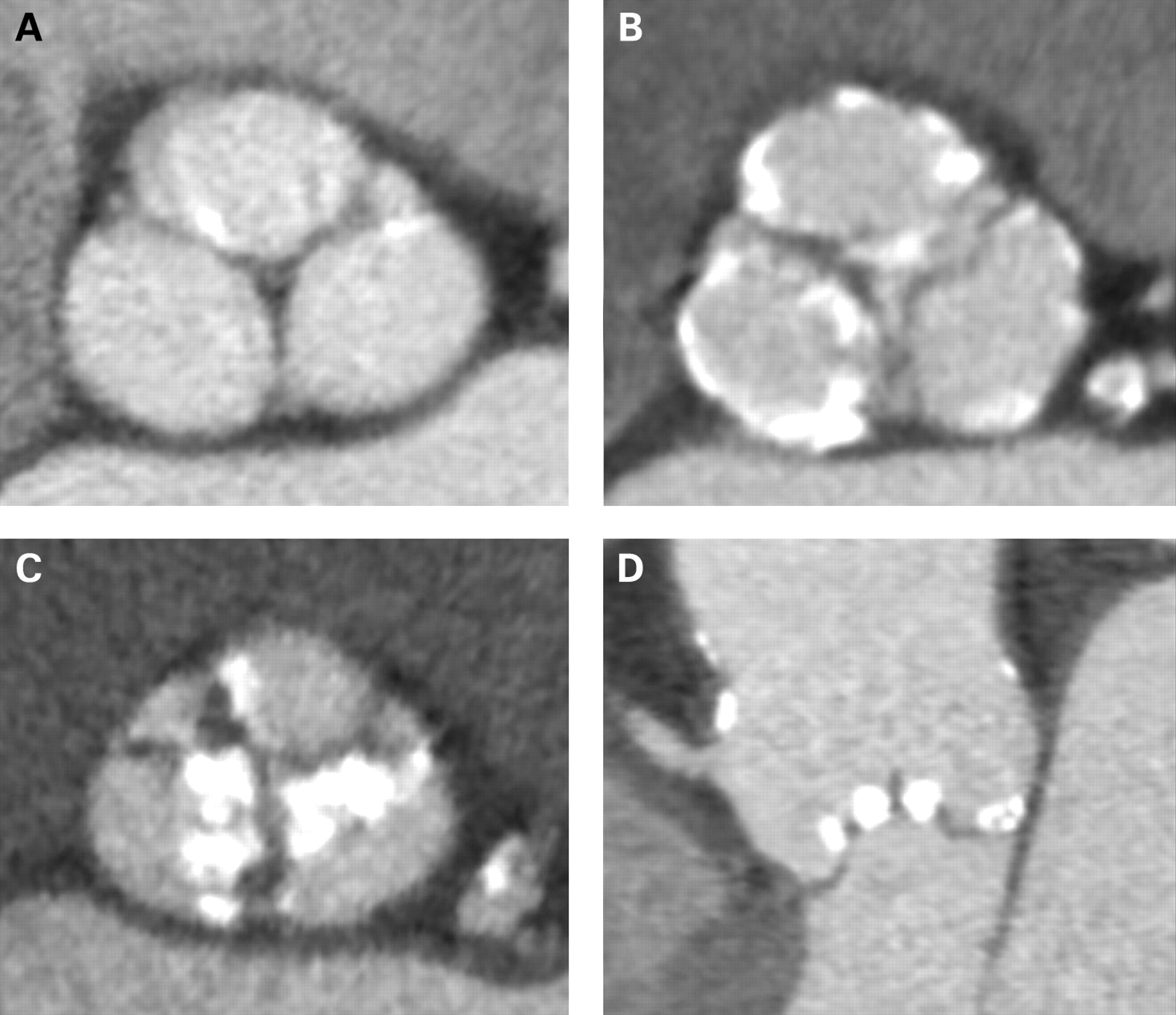
Before the percutaneous valve procedure, multislice computed tomography (MSCT) can depict the extent and exact location of calcifications. During percutaneous aortic valve replacement, extensive calcifications may hamper the ability to cross the native valve. On transverse reconstructions through the plane of the aortic valve, the calcifications can be quantified. Panel A shows small isolated spots (mildly calcified aortic valve). In contrast, panel B shows multiple larger spots, predominantly at the base of the leaflets (moderately calcified aortic valve). Panel C shows a heavily calcified aortic valve, mainly located at the tips of the leaflets. In panel D, a sagittal view through the aortic valve is shown, demonstrating bulky calcifications at the tip of the aortic valve leaflets.
The assessment of coronary anatomy is also important in the selection process. Conventional coronary angiography should be performed to exclude the presence of significant coronary artery disease.3 Although conventional angiography remains the “gold standard”, non-invasive evaluation of coronary artery disease may be performed with MSCT as well. This technique also allows detailed, three dimensional evaluation of the relation between the coronary ostia and the aortic valve leaflets. This may be important to avoid coronary occlusion during aortic valve implantation. It has been demonstrated that the relation between the aortic annulus, the coronary ostia and leaflets is highly variable. In a cohort of 169 patients undergoing MSCT scanning, it was noted that the distance between the aortic annulus and the coronary ostia was smaller than the length of the aortic valve leaflets in up to 49% of the patients.20 In these patients, the risk of coronary occlusion during percutaneous aortic valve implantation may be increased. Therefore, both invasive and non-invasive evaluation of coronary anatomy can provide important information for the selection of candidates for percutaneous aortic valve implantation.
The assessment of aortic annulus diameters is of the utmost importance for correct prosthesis sizing. Various prosthesis sizes for the balloon expandable and self expanding prostheses are available for a wide range of annulus diameters. However, at present no gold standard is available for the exact measurement of the aortic annulus diameter. Typically, TTE is used to assess the aortic annulus diameter (fig 4, panel A). However, it may underestimate the diameter when compared with TOE.21 Importantly, with both techniques the basal attachments of the leaflets are used as landmark points, potentially underestimating the true/full aortic annulus diameter.w12 In contrast, three dimensional echocardiography, MRI and MSCT allow a three dimensional, multi-planar reconstruction of the aortic annulus (fig 4, panels B and C). This may result in a more accurate measurement of the aortic annulus diameter.

Before percutaneous aortic valve implantation, the aortic annulus diameter should be assessed. For this purpose, different imaging modalities are available. Panel A demonstrates conventional transthoracic echocardiography, where the annulus diameter is assessed at the ventricular aspect of the leaflet insertion. In panel B, three dimensional transoesophageal echocardiography is shown. Panel C demonstrates a sagittal reconstruction through the aortic valve. The dotted arrow indicates the measurement of the aortic annulus.
Furthermore, the anatomy of the aorta and peripheral vasculature should be assessed. Conventional angiography is the preferred imaging modality. However, MSCT and MRI may also provide the necessary information. A transapical approach is preferred over the transfemoral approach in patients with a severe angulation of the aortic arch, or the presence of atheroma in the aorta. In patients with severe calcifications and/or tortuosity of the femoral vessels, or small vessel diameters (typically <6 to 9 mm), a transfemoral approach is contraindicated, because of the high risk of vascular complications. Finally, contraindications such as the presence of atrial or ventricular thrombi, and a very poor left ventricular ejection fraction should be assessed.
Aortic valve implantation
During the aortic valve implantation procedure, a combination of fluoroscopy/angiography and TOE is typically used.5 Rather than replacing each other, these techniques are complimentary during the aortic valve implantation. Contrast autography can be used for final assessment of the aortic annulus diameter and prosthesis sizing. However, similar to echocardiography, it is limited by its two dimensional nature.
Positioning and final deployment of the prosthesis is performed under fluoroscopy and/or TOE guidance (fig 5, panel A and B). In patients with severely calcified aortic stenosis, fluoroscopy allows easy localisation of the prosthesis in relation to the aortic annulus and leaflets. Conversely, in patients without severe calcifications, TOE may be more helpful for exact prosthesis positioning. Typically, a long axis (130°) transoesophageal view is used.21 Critical assessment of the exact location of the undeployed prosthesis, in relation to the native aortic valve, is important. When the correct positioning is confirmed with fluoroscopy and/or echocardiography, the prosthesis is deployed under rapid right ventricular pacing.

Imaging during a percutaneous implantation procedure of a balloon expandable valve. Panel A demonstrates a long axis three dimensional transoesophageal echocardiography view during balloon inflation. Panel B demonstrates the final deployment of the prosthesis. After the implantation, coronary angiography should be performed to confirm coronary patency (panel C). LAD, left anterior descending artery; RCA, right coronary artery.
Immediately after the stent deployment, valve competence should be assessed. A transoesophageal short axis view is the best view to differentiate between valvular and paravalvular aortic regurgitation. The severity of paravalvular aortic regurgitation can be used as an indicator of procedural success, and can help to decide if balloon (re-) dilatation is necessary. In 32 patients undergoing TOE guided balloon expandable aortic valve implantation, Moss et al noted some degree of aortic regurgitation in 88% of the patients.21 In the majority of the patients (84%) paravalvular aortic regurgitation was present. Thirteen patients underwent subsequent re-dilatation of the prosthesis, with an improvement in aortic regurgitation of more than one grade in seven of the 13 patients. Mild valvular regurgitation typically resolves during the first days after implantation.21
For the assessment of coronary patency, coronary angiography should be performed after prosthesis implantation (fig 5, panel C). Acute coronary occlusion is a serious, but rare, complication. Interestingly, it has been demonstrated that correct positioning of the prosthesis even allows coronary intervention after percutaneous aortic valve implantation.w13
Various complications have been reported after percutaneous aortic valve implantation, mainly related to vascular access and thromboembolic complications. In addition, new atrioventricular block may occur in up to 6% of the patients.w14 In addition to fluoroscopy, TOE may help in the recognition of complications during percutaneous aortic valve implantation. In a study of 11 patients (median logistic EuroScore 36%) undergoing self expanding CoreValve implantation, it was noted that routine TOE enabled the early detection of complications (a thrombus in the left ventricular outflow tract and pericardial effusion).w15
Finally, intracardiac echocardiography and novel three dimensional TOE may be helpful in the guidance of percutaneous aortic valve implantation. Three dimensional TOE may allow a more precise evaluation of the aortic valve, and may improve spatial orientation and prosthesis positioning.w16 However, more studies are needed to understand fully the exact value of these techniques in percutaneous aortic valve implantations.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit = men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Follow-up
In addition to complications and conventional outcome parameters (such as mortality, stroke, major cardiac events), prosthesis function and position should be assessed during follow-up.22 For this purpose, TTE is the most commonly used technique.w17 In most studies, the AVA and mean pressure gradient are used to quantify aortic valve function (table 1). In addition, aortic regurgitation should be assessed.
The exact position of the prosthesis and the relation between the stent and the coronary arteries can be assessed with MSCT. This technique may be preferred over TTE because it is less hampered by artefacts, and has a high spatial resolution. In addition, it allows a more precise evaluation of prosthesis deployment and diameters.w18 Examples of MSCT images after percutaneous aortic valve implantation are shown in fig 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
With the use of multislice computed tomography, the exact location of the prosthesis, and the relation with the coronary ostia, can be assessed. In panels A and B, an example is demonstrated where the prosthesis extends beyond the coronary ostia (white arrows). During the implantation procedure, good patency of the coronary arteries was demonstrated. In panels C and D, an example is demonstrated where the prosthesis is positioned below the coronary ostia (black arrows). LAD, left anterior descending artery; RCA, right coronary artery.
Conclusions
Percutaneous aortic valve implantation is a promising technique for highly symptomatic patients with severe aortic stenosis. Several studies have demonstrated good results for both the balloon expandable and self expanding valves. A critical selection of potential candidates, including clinical evaluation, assessment of surgical risk and feasibility of the procedure, is needed. Several imaging modalities are available for patient selection, procedural assistance, and follow-up.
REFERENCES
- 1.↵
▸ Current ESC guidelines on the management of patients with valvular heart disease, including aortic stenosis.
- 2.↵
▸ This survey provides important information on the characteristics and management of patients with valvular heart disease in Europe. The survey included data of 5001 patients from 92 centres in 25 countries.
- 3.↵
▸ This is the first official statement that provides important recommendations on the patient selection, implantation procedures, and follow-up for percutaneous aortic valve implantation.
- 4.↵
- 5.↵
▸ This is a more general statement on the development of percutaneous valve procedures, including aortic and mitral valve procedures.
- 6.↵
- 7.↵
▸ This is the first report of the percutaneous implantation of a balloon expandable aortic valve in a patient with severe aortic stenosis.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
▸ This is the first report of the implantation of the self-expanding CoreValve prosthesis.
- 16.↵
- 17.↵
▸ This is the largest published study to date using the self expanding CoreValve Revalving system. It involves a multicentre registry following CE mark approval of the device, and demonstrates a high procedural success rate and a low 30 day mortality.
- 18.↵
▸ This is the first report of the valve-in-valve concept in an animal model.
- 19.↵
- 20.↵
▸ This study demonstrates the value of MSCT in planning percutaneous aortic valve implantation procedures. MSCT can provide detailed information on the aortic annulus, and the relation with the coronary ostia, based on a three dimensional reconstructed image.
- 21.↵
- 22.↵
Supplementary materials
Footnotes
Additional references are published online only at http://heart.bmj.com/content/vol95/issue18
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. Dr Victoria Delgado is financially supported by awards from the European Society of Cardiology. Dr Jeroen J Bax receives research grants from Edwards Lifesciences, GE Healthcare, BMS medical imaging, Boston Scientific, Medtronic, Biotronik and St. Jude Medical. The remaining authors have no relationships to disclose.
Provenance and peer review Not commissioned; not externally peer reviewed.