Article Text

Statistics from Altmetric.com
Heart failure is a syndrome resulting from a structural or functional cardiac disorder. For a diagnosis of heart failure to be made, there should be symptoms or signs, such as breathlessness, effort intolerance or fluid retention, together with objective evidence of cardiac dysfunction.
Heart failure is an increasingly important chronic disease syndrome, associated with poor prognosis, poor quality of life for patients, and high healthcare costs.1 w1 In the general population, where all grades of heart failure are represented, 5 year mortality is around 42%2; however, where the diagnosis is established during a hospital admission, 5 year mortality is between 50–75%,3 w2 although the prognosis has improved in the past 10 years.
Prevalence and incidence of heart failure
Studies including objective assessment of left ventricular (LV) function, usually echocardiography, indicate a prevalence of left ventricular systolic dysfunction (LVSD) of 2.9% in patients under 754 and up to 7.5% in 75–84 year olds.w3 In the largest recent prospective evaluation of heart failure in the community, definite heart failure was found in 2.3% (95% confidence interval (CI) 1.9% to 2.8%) of the population, with left ventricular ejection fraction (LVEF) <40% in 41% of cases. However, if the LVEF cut-off was set at under 50% rather than 40%, now advocated in some guidelines, 3.1% (95% CI 2.6% to 3.7%) of people aged 45 or over were defined as having heart failure.5
Estimates on heart failure incidence are less available, and vary from 0.9–2.26 per 1000 females (age 45–74) per year and 1.6–4.6 men per 1000 population (age 45–74) per year. Incidence rises rapidly in the elderly, with 1% of men per year developing heart failure after 75 and almost 2% per year in the over 85s.
The typical primary care physician, caring for 2000 patients, is likely to have 40–50 patients with heart failure (more if the population is elderly), and to have five or so new cases of heart failure diagnosed each year, with the diagnosis being suspected in perhaps three times as many. The syndrome is, therefore, relatively common but not so frequent that the individual practitioner will become expert in diagnosis. Clear guidance is needed on which clinical features and combination of investigations is best to rule out or rule in heart failure in patients with new symptoms.
Burden of heart failure on healthcare systems
Chronic heart failure remains one of the most costly conditions to manage: the syndrome is common, it frequently results in hospital admission, admissions are long, and re-admission is frequent, particularly where chronic disease management programmes are not running (nearly 25% of patients are readmitted within 12 weeks of discharge).7 As a consequence, heart failure accounts for around 2% of total healthcare expenditure in most developed countries.
Good diagnosis is the cornerstone of good management
There is a large evidence base for treatments that improve morbidity, global quality of life, and mortality in all grades of heart failure due to LVSD,8 9 and can delay LVSD progression to symptomatic heart failure.w4 Despite this extensive evidence, heart failure remains suboptimally diagnosed and treated in many countries.w5 An essential element for treatment success is the reliable and precise diagnosis of heart failure.
Diagnostic issues in heart failure
The evaluation of patients with suspected heart failure entails determining more than just whether the syndrome is present or not. It is important to identify the underlying cardiac pathologies, exacerbating or precipitating factors, and the whole body's response to the cardiac dysfunction—including particularly renal function. Guidelines for the evaluation and management of heart failure have been published by professional societies in North America (American College of Cardiology/American Heart Association (ACC/AHA)10 and Consensus Recommendationsw6) and Europe (European Society of Cardiology).11 The latter state that the diagnosis of heart failure is justified when there are typical signs and symptoms of heart failure and myocardial dysfunction, confirmed by the objective evidence of cardiac dysfunction at rest. In the case of diagnostic uncertainty, a clinical response to treatment directed at heart failure is helpful in establishing the diagnosis (box 1). Simple and reliable diagnostic procedures are very important for primary care physicians, who are responsible for the early diagnosis of heart failure and implementation of adequate treatment in most healthcare systems.
Box 1 Definition of heart failure in the current European Society of Cardiology guidelines for the diagnosis and management of heart failure11
Heart failure is a syndrome in which patients have the following features:
Symptoms typical of heart failure (breathlessness at rest or on exertion, fatigue, tiredness, ankle swelling)
AND
Signs typical of heart failure (tachycardia, tachypnoea, pulmonary rales, pleural effusion, raised jugular venous pressure, peripheral oedema, hepatomegaly)
AND
Objective evidence of a structural or functional abnormality of the heart at rest (cardiomegaly, third heart sound, cardiac murmur, abnormality on the echocardiogram, raised natriuretic peptide concentration)
Current NICE guidance on diagnosing heart failure
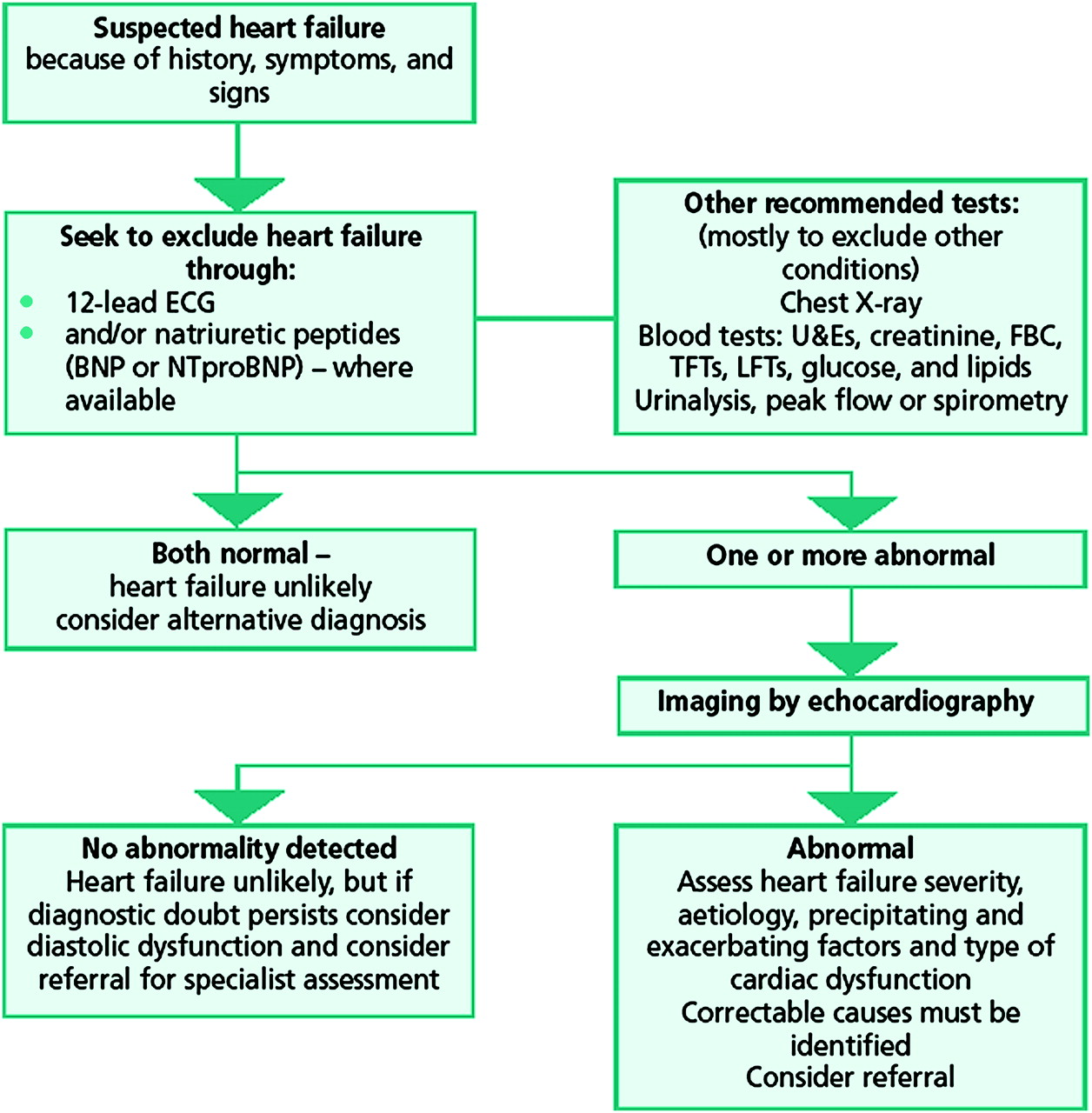
The National Institute for Health and Clinical Excellence (NICE) guideline on chronic heart failure for primary and secondary care in England recommends that patients with suspected heart failure should have an electrocardiograph (ECG) and/or B-type natriuretic peptide (BNP or N terminal pro-BNP (NT-proBNP)) assay performed.12 If both are normal, then heart failure is unlikely, and an alternative diagnosis to explain the symptoms should be considered. If either is abnormal, then the patient should have an echocardiogram, or other imaging test, to confirm underlying cardiac dysfunction (figure 1). This guidance was based on the high sensitivity of both plasma BNP and the ECG, and the result of a health economic analysis that demonstrated that the cost per life year gained through echocardiography is dependent upon the proportion of patients referred for echocardiography in whom the diagnosis of heart failure is confirmed.

{kind=link}
Diagnostic algorithm recommended for use in primary care by the National Institute for Health and Clinical Excellence in England, 2003.12 BNP, B-type natriuretic peptide; FBC, full blood count; LFTs, liver function tests; NTproBNP, N terminal pro-BNP; TFTs, thyroid function tests; U&Es, urea and electrolytes.
However, the current diagnosis of heart failure in primary care is often inaccurate. In one recent UK study, only 34% of patients with an existing clinical label of heart failure in routine general practice records had this diagnosis confirmed at echocardiography and review.13
There have been seven recent systematic reviews relevant to the diagnosis of heart failure in primary care. Three covered all symptoms, signs and diagnostic tests,12 14 w7 three concerned BNP alone,15 w8 w9 and one was a review of the accuracy of the 12 lead ECG.16
Symptoms and signs
Individual symptoms (such as breathlessness, fatigue, exercise intolerance and fluid retention) and signs (such as resting tachycardia, raised jugular venous pressure (JVP), displaced apex beat, third heart sound) are generally weak predictors of heart failure, with poor reliability and little agreement between clinicians on their presence or absence, even among specialists.
In a recent systematic review, a number of symptoms were reasonably specific, including a history of myocardial infarction (89% specificity), orthopnoea (89%), cardiomegaly (85%), added heart sounds (99%), lung crepitations (81%), and hepatomegaly (97%) (table 1). However, in primary care, the most useful symptoms/signs in diagnosis have high sensitivity, since this might enable the clinician to rule out heart failure if the symptom/sign was absent, without the need to refer for further investigation. Dyspnoea is the only clinical feature that comes close to this ideal with a sensitivity of 87%. In practice this symptom is present in the majority of patients in whom heart failure is suspected, with a frequency as high as 95% in one of the datasets. Nevertheless, a sensitivity of 87% is not high enough on its own to rule out heart failure if dyspnoea is absent.
Overall accuracy of clinical features of heart failure
Investigations
Both ECG16 w10 w11 and BNP15 w7 w8 have high sensitivity for heart failure, and so are good tests at ruling out the diagnosis (table 2). UK based studies restricted to use of ECG in primary care, however, give a more mixed picture on the value of ECG, with sensitivity in one study as low as 73%.16 These differences may relate to both differences in population characteristics, and to the skill of the practitioner interpreting the ECG. Similarly, while the chest x-ray may show evidence of heart failure (eg, cardiomegaly, pulmonary vascular congestion), it is not a good independent predictor, and is of most value in identifying alternative causes of symptoms such as lung disease or pleural effusion.
Overall accuracy of investigations for heart failure
In a review of four studies that evaluated the diagnostic accuracy of the resting ECG in the specific context of referral from primary care to echocardiographic services, sensitivity of the ECG varied from 73–91%, and the authors concluded that the ECG was an inadequate screening tool.16 A review of the diagnostic accuracy of natriuretic peptides and ECG in the diagnosis of LVSD found similar diagnostic accuracy between ECG, BNP and NT-proBNP and no value from combining BNP with ECG.17 A recent systematic review confirmed that adding the ECG to clinical features plus the plasma BNP result did not improve the accuracy of diagnosis.14
It is likely that BNP is a more accurate test for heart failure than it is for LVSD. Indeed, a recent systematic review of BNP studies concluded that while BNP is useful for excluding heart failure, it is more limited for ruling out systolic dysfunction, with an area under the curve (AUC) of 0.93 for heart failure but only 0.75 for systolic dysfunction.18 There is no evidence of any significant differences in test performance between BNP and NT-proBNP.17 18 Other recent reviews of BNP have confirmed its value as a ‘rule out’ test for heart failure.w12–w14
Echocardiography is the most readily available ‘reference standard’ investigation for LVSD and valve disease. Assessment of diastolic dysfunction can also be made on echocardiography,19 but the interpretation of the findings may be difficult, particularly in the elderly and in patients with atrial fibrillation (up to 30% of new cases of heart failure in most series). In practice today, ‘normal ejection fraction’ (‘preserved systolic function’, ‘diastolic’ or ‘non-systolic’) heart failure often remains a diagnosis of exclusion. Echocardiography after a plasma BNP test has been performed is an attractive option, particularly if the supply of echocardiography is limited or access is slow, though appropriate cut points for BNP (or NT-proBNP) are then needed.
Role of clinical decision rules in the work up of patients with suspected heart failure
There are several well developed heart failure diagnostic tools which combine the results of different symptoms/signs and investigations. Mosterd et al applied criteria from six established heart failure scores including Framingham, Walma, and Boston to a sample of 54 participants in the population based Rotterdam study.20 Most showed high utility to detect definite heart failure with areas under the receiver operated characteristic (ROC) curve (AUC) ranging between 0.89–0.96. However, use of these would be impractical in routine primary care because of the substantial number of variables in several scores; and also because many of the clinical signs have considerable inter-observer variation even among specialists (raised jugular venous pressure (JVP), third heart sound, hepatojugular reflux).w15 w16 Furthermore, four of the scores include specific chest x-ray parameters difficult to apply in general practice.
A recent meta-analysis using individual patient data identified a simple new diagnostic score. This rule suggests that in a patient presenting with new symptoms such as breathlessness in whom heart failure is suspected, if the patient has any one of (a) history of myocardial infarction or (b) basal crepitations or (c) is a male with ankle oedema (so called MICE score), then it is appropriate to refer straight for echocardiography as the probability of heart failure is high. Otherwise, a plasma BNP test should be performed, and referral to echocardio-graphy should be organised depending on the concentration of plasma BNP (box 2).14
Box 2 Simple clinical decision rule (MICE) developed in a UK Health Technology Assessment for the diagnosis of heart failure in primary care14
In a patient presenting with symptoms in whom heart failure is suspected, refer straight to echocardiography if the patient has any one of:
history of myocardial infarction, or
basal crepitations, or
male with ankle oedema
Otherwise, carry out a BNP test, and refer for echocardiography depending on the results of the BNP:
Female without ankle oedema—refer for echocardiography if BNP >210–360 pg/ml depending upon local availability of echocardiography (or NT-proBNP >620–1060 pg/ml)
Male without ankle oedema—refer for echocardiography if BNP >130–220 pg/ml (or NT-proBNP >390–660 pg/ml)
Female with ankle oedema—refer for echocardiography if BNP >100–180 pg/ml (or NT-proBNP>190–520 pg/ml)
BNP, B type natriuretic peptide; NT-proBNP, N terminal pro B type natriuretic peptide.
Limitations of the evidence base
There is no single ideal reference standard for heart failure, since there is no single cardiac disorder that accounts for the syndrome. The underlying cardiac disorders can be classified in different ways. The standard approach is to divide heart failure into low ejection fraction and normal ejection fraction heart failure, if significant valve disease has been excluded as the primary cause of the heart failure. Echocardiography is a suitable reference standard for low ejection fraction heart failure, but is not as robust for normal ejection fraction heart failure. The definitive tests to diagnose normal ejection fraction heart failure (pressure–volume measurements at cardiac catheterisation) are often not carried out, so the diagnosis usually relies upon clinical judgement and supportive evidence.
Studies that have tested the value of the ECG in the diagnosis of heart failure have used different criteria with which to define abnormality, and there has been variation in the experience and expertise of the person reading the ECG. Many general practitioners are unable to interpret ECGs accurately.
For natriuretic peptides, most of the existing research has been done on secondary care populations, or in the context of screening studies that identify prevalent cases of heart failure, or include patients with existing diagnoses of heart failure. This may introduce significant spectrum bias and affect whether the cut-off values are reliable for the target population, namely symptomatic patients presenting in primary care.
Conclusions
Heart failure is a clinical syndrome that may be difficult for a primary care physician to diagnose accurately, particularly if the symptoms develop slowly and are not so severe as to warrant immediate hospitalisation. Access to tests that can help rule out heart failure (such as plasma BNP or NT-proBNP) when combined with clinical assessment can be very useful to aid the physician's investigation pathway. Patients likely to have heart failure after such initial assessment should undergo echocardiography, with expert interpretation, to help confirm the diagnosis and to determine the underlying cardiac pathophysiology. More detailed diagnostic work-up may also be required to fully characterise the syndrome and determine the appropriate management plan.
Diagnosis of heart failure in primary care: key points
Heart failure is difficult to diagnose in primary care.
Early diagnosis can favourably alter prognosis and mortality.
A number of symptoms and signs have some diagnostic value in the clinical assessment of a patient with suspected heart failure. Dyspnoea is the symptom with the highest sensitivity, but it is not sufficiently high that heart failure can be ruled out in its absence.
ECG, BNP and NT-proBNP all have high sensitivity for heart failure.
Head-to-head studies and systematic reviews suggest that BNP or NT-proBNP is a more accurate investigation than ECG for the diagnosis of heart failure.
There is no evidence that performing both BNP and ECG improves the diagnosis of heart failure.
There is no evidence of any significant difference in accuracy between different BNP assays.
A simple clinical score based upon gender, history of myocardial infarction, presence of oedema, and presence of basal lung crepitations may help a physician discriminate between people with suspected heart failure who should be referred straight for echocardiography, and people for whom the diagnosis is less likely and should be confirmed by a BNP test before referral.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
- ↵
- ↵
Useful recent mortality data that encompass outcomes in all grades (mild to severe) of heart failure in a prior screened UK population.
- ↵
- ↵
- ↵
The largest of the UK heart failure cohorts identified by random population screening.
- ↵
The best estimates on the current incidence of heart failure in the UK.
- ↵
- ↵
The pooled data for the effectiveness of ACE inhibitors in heart failure.
- ↵
Pooled data on the effectiveness of β-blockers in heart failure.
- ↵
The current main US guidelines for diagnosis and management of heart failure.
- ↵
The most recent ESC guidance on the diagnosis of heart failure.
- ↵
The current NICE heart failure guidelines on diagnosis and management, though the revised update is due sometime in 2010.
- ↵
- ↵
The most recent systematic review on the diagnostic options for heart failure which includes an individual patient data meta-analysis on the utility of BNP testing.
- ↵
- ↵
- ↵
- ↵
- ↵
Consensus guidelines on the diagnosis of preserved systolic function heart failure.
- ↵
Supplementary materials
Web Only Data hrt.2007.139402
Files in this Data Supplement:
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data Supplement - Manuscript file of format pdf
Footnotes
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. FDRH has received research funding from Roche Diagnostics, and occasional speaker fees and symposia expenses from Roche and Bayer Diagnostics. JM chairs the NICE Heart Failure Guidelines committee. MC has provided consultancy advice to, and received occasional speaking fees from, Stirling Medical and Roche Diagnostics. No author has stock or shares in any device or assay company.
Provenance and peer review Commissioned; not externally peer reviewed.