Article Text

Statistics from Altmetric.com
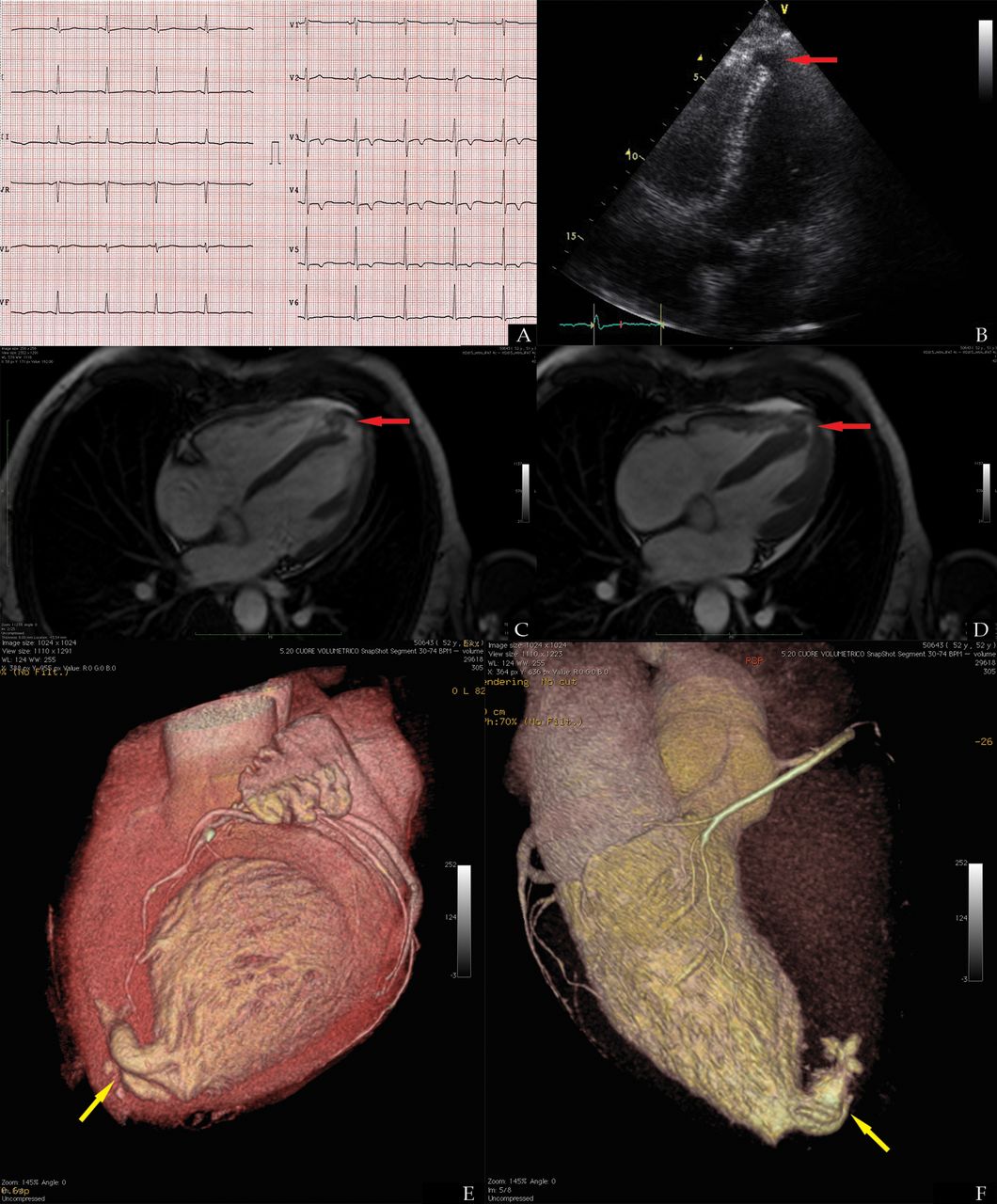
A 52-year-old man lost consciousness while running on a hot day. He had been a professional football player for 15 years. ECG showed sinus rhythm, high R voltages with T inversion fulfilling the criteria for left ventricular (LV) hypertrophy (Figure 1A). This ECG LV hypertrophy pattern had been discovered at the age of 15 interpreted as ‘athlete's heart’. An echocardiographic exam showed normal ventricular volumes, wall thickness and contractility, but a defect in the apical interventricular septum was present (Figure 1B; online supplementary video S1). A cardiac MRI study revealed an ‘outpouching’ of the apical segment of the interventricular septum protruding into the right ventricular apex and surrounded by trabeculations, diagnostic criteria for a muscular LV apical diverticulum (Figure 1C,D; online supplementary video S2). An ECG LV hypertrophy pattern with T waves inversion can be observed in half of LV diverticula; associated coronary arteries anomalies are described too.1 ,2 A CT showed normal coronary arteries and a three-dimensional CT reconstruction revealed a tortuous intracavitary diverticulum structure (Figure 1E,F). Cardiac diverticula are often clinically silent but may be associated with systemic embolism, arrhythmias, heart failure and cardiac rupture. Surgery may be considered in symptomatic patients despite medical therapy or believed at risk of rupture. In our case, medical follow-up without therapy was preferred as no arrhythmia was detected and good contractility of the diverticulum was felt to make thrombus formation unlikely. An MRI study is advised for differentiating diverticula from aneurysms and estimating dimensions and muscular or fibrous walls.
{kind=link}
(A) ECG showing a normal sinus rhythm, left ventricular hypertrophy and inverted T waves in precordial leads. (B) Transthoracic echocardiogram five chambers view, a defect of the apical interventricular septum is seen (red arrowhead). (C) MRI four chamber modified view, diastolic (C) and systolic (D) still image of a cine sequence (Siemens TrueFisp) showing an apical left ventricular diverticulum with normal contractility (red arrowhead). (E) Volume-rendered CT three-dimensional (CT 3-D) reconstruction of the heart seen from an apical view (yellow arrowhead). (F) CT 3D reconstruction from a posterior view after electronic cropping of the right ventricle showing the complexity of the apical diverticulum cavity (yellow arrowhead).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online video 1
- Data supplement 2 - Online video 2
Footnotes
-
Contributors AC is the first author and responsible for the overall content. LF is responsible for the CT scan images, their 3D reconstruction and AP is responsible for the cardiac MRI images; they both helped in the planning and revision of the manuscript.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Data sharing statement Clinical data and supplementary diagnostic images are available for those who may be interested.