Article Text

Statistics from Altmetric.com
Over the past 20 to 30 years, the epidemiological burden of cardiovascular disease in high-income countries has transformed from a predominance of acute ischaemic events in middle-aged men to chronic forms of heart disease equally affecting both sexes. The first wave of epidemiological change saw the emergence of heart failure (HF) as a substantive public health issue.1 Beyond pharmacological agents and devices, a large body of evidence now supports the application of predominantly nurse-led, multidisciplinary management programmes to address high levels of morbidity and mortality in that patient population; with home-based models of care seemingly more effective than other modes in delivering what are essentially the same components of care.2 The second wave of epidemiological change (reflecting subtle but important differences in the natural history of HF and atrial fibrillation (AF)) saw the emergence of AF as a compounding burden of disease within our ageing populations.3 Often characterised as a ‘one in a hundred’ condition, contemporary epidemiological reports show that the incidence of AF (in all its forms) is increasing and its population prevalence ranges from 2.3%–3.4% with a marked gradient in cases according to age.3 It is on this basis that 10%–20% of individuals aged >65 years develop AF with a lifetime risk of one in four. Primary care contacts and hospitalisations attributable to AF (both as a primary and secondary cause) are on the rise and its individual to societal burden is substantive.3 A critical feature of this burden is the nexus between AF and other costly and disabling conditions; up to 50% of individuals with HF develop AF and its presence confers a threefold to fivefold increased risk of ischaemic stroke.3 And yet, by itself AF is not a benign condition. Data from longitudinal population cohort studies show that, in the longer term, AF is independently associated with a 1.5-fold to 2.0-fold increased risk of death.3 However, its treatment and management is complicated by the need to navigate the fine line between benefit and risk of therapeutic agents designed to stabilise an inherently fast and chaotic heart rate (either through rhythm or rate control) and reduce the risk of thrombotic events without provoking a bleeding event.4
In recognition of the increasing and complex burden posed by AF, it has been proposed that a more individualised approach to its management (with a strong component of patient-centred care and outcomes) should be applied.5 In essence, this would match the substantive body of evidence supporting the application of multidisciplinary, HF management programmes1 that already incorporate positive outcomes from a large component of the patient population with combined HF and AF. To date, only two randomised controlled trials of integrated AF management, but targeting different ends of the AF spectrum, have been reported.4 6 The first trial examined the impact of a nurse-led, outpatient programme of management of patients (mean age 67 years, 41% women) with mostly paroxysmal AF on the coprimary endpoint of cardiovascular hospitalisation and cardiovascular mortality.6 The second trial examined the impact of a home-based, nurse-led programme of postdischarge management on days alive and out-of-hospital in older patients (mean age 72 years, 48% women) hospitalised with a chronic form of AF.4 Both trials achieved their respective primary endpoints. Other non-randomised studies have also reported positive findings from an integrated management approach.7 As with the early phases of research focusing on HF management, currently there is a strong focus on managing younger and less complicated individuals with AF via an outpatient model of care.
Regardless of the theoretical benefits of applying integrated management of AF,5 the evidence to support its application (particularly across the full spectrum of cases) remains in its infancy. For example, while both randomised trials to date have suggested survival benefits associated with integrated AF management, they were underpowered to address this important and persuasive endpoint. It is on this basis that Gallagher and colleagues analysed data from these two randomised trials and added outcome data from a less rigorous, non-randomised trial.7 Notwithstanding the fact that study findings rely on outcomes from only 1383 patients, it was determined that integrated management confers a significant reduction in the risk of all-cause mortality (OR 0.51 relative to standard management) and cardiovascular hospitalisation (OR 0.58) but not AF-related hospitalisation and cerebrovascular events.7 Two critical points are worthy of comment: First, the addition of outcomes from a non-randomised trial and early randomised trials will undoubtedly inflate the effect size reported; the likelihood of more modest findings with greater trial data being generated is highly likely. Second, at this stage there is little sign that integrated management has ‘disease-specific’ effects on AF. Indeed, based on available evidence, one might argue that these data merely support the extension of current disease management programmes (particularly HF programmes) to include all patients affected by AF.8
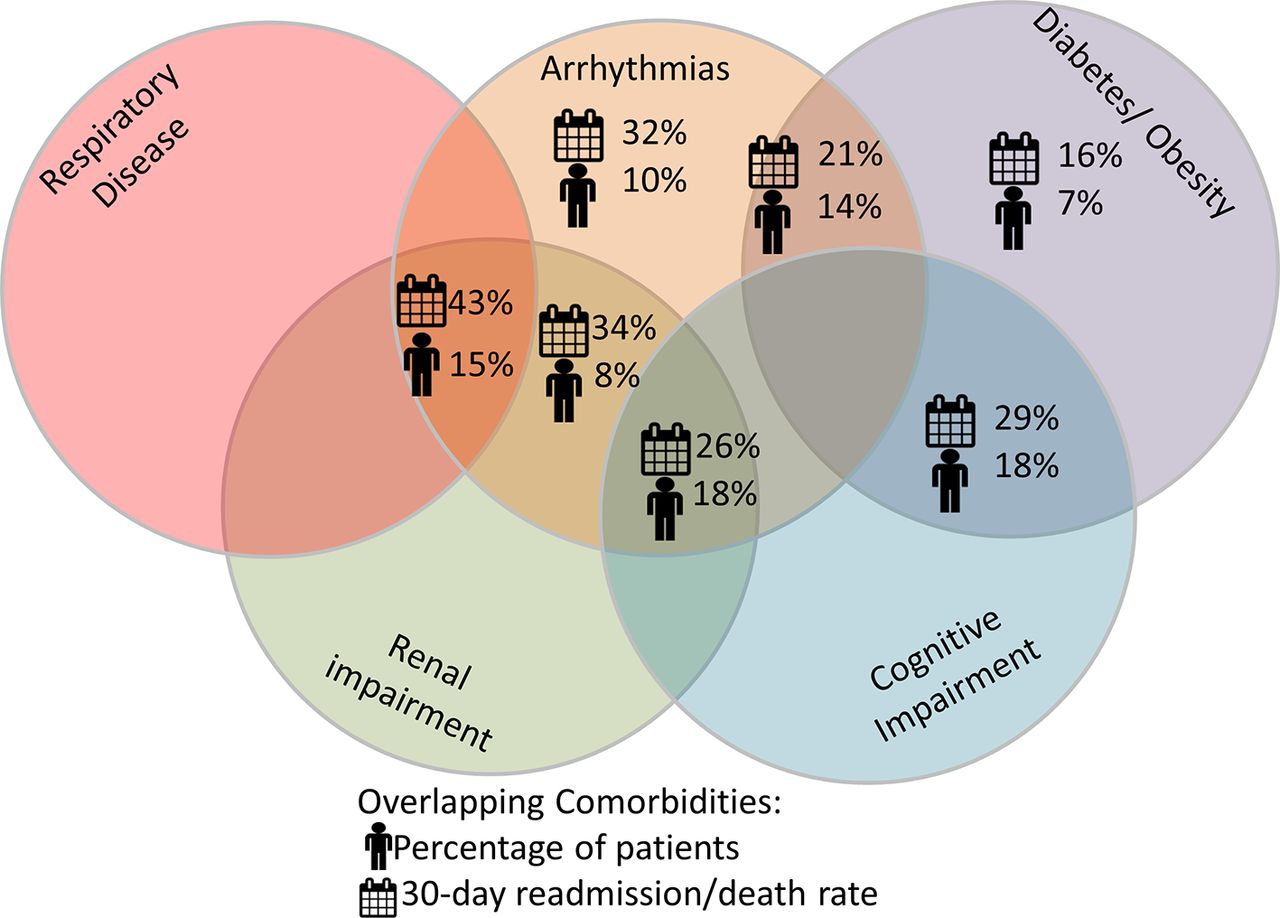
Despite the clearly positive findings reported by Gallagher and colleagues in their meta-analysis, therefore, it is probably too early to advocate the systematic application of integrated management programmes for AF. This is particularly true when considering the lessons learnt from the development of evidence-based HF management programmes. A key discussion point in the optimal management of HF is an apparent ‘ceiling effect’ associated with the application of increasingly more intensive, sophisticated and indeed costly monitoring and management techniques. In essence, applying ‘more’ has not delivered additional gains in HF-related morbidity and mortality.1 One could probably argue, in this context, that a ‘less is more’ approach is probably cost-effective; particularly when one considers recent data that suggest otherwise effective home-based management confers an increased risk of mortality in those patients with chronic heart disease at the higher end of the clinical complexity/multimorbidity spectrum.8 When considering that the largest portion of the patient population with AF is older and more clinically complex,3 this represents a problem that requires adequately powered, randomised controlled trials to formally test the hypothesis that these ‘real-world’ patients can—(a) be safely and effectively managed and (b) truly derive suggested survival benefits from integrated AF management. As shown in figure 1 (an original analysis of 30-day outcomes in >800 patients participating in a recently completed HF management trial), the presence of AF with different combination of multimorbidity (including concurrent renal impairment, respiratory disease and cognitive impairment) confers markedly different health outcomes.

{kind=link}
Impact of AF on 30-day outcomes when combined with other common comorbid conditions in patients hospitalised with HF. AF, atrial fibrillation; HF, heart failure.
To bring ‘order’ to this chaotic rhythm disorder via integrated management, therefore, there is still much to be done; particularly in respect to cost-effectively dealing what is likely to be an increasingly older and more clinically complex patient population in whom the margin of error (in terms of benefits vs risk) is likely to become narrower. However, initial outcomes from integrated programmes of care, as reflected in the meta-analysis published by Gallagher and colleagues,7 represent a promising start.
Footnotes
Funding SS is supported by the National Health and Medical Research Council of Australia (APP1041796).
Competing interests SS was the Principal Investigator of the SAFETY Trial.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Arrhythmias and sudden death