Article Text

Statistics from Altmetric.com
Learning objectives
Familiarise the reader with the various valve lesions encountered in congenital heart disease and the pathophysiology of such lesions.
Recognise the commercially available transcatheter valves in the market that can be used in congenital heart disease.
Achieve a basic understanding of future directions in this field.
Introduction
Survival into adulthood for patients with congenital heart disease (CHD) is expected in those that have access to specialty care. Many of them will need multiple valve surgeries over their lifetime, which increases their risk of morbidity and mortality.1 The advances in interventional cardiology and the introduction of the Melody valve, a balloon expandable pulmonary valve2 in 2000 have radically altered the management options for these patients by reducing the need for redo surgical interventions.3 We herein discuss the existing and future catheter-based valve replacement and repair options for adult CHD.
Pulmonary valve
Pulmonary valve disorders in CHD can either be primary or postoperative. Primary pulmonary valve dysfunction may be isolated, as in congenital pulmonary stenosis (PS), or may be a part of a more complex coalescence of lesions as seen in tetralogy of Fallot, wherein pulmonary valvular, subvalvular and/or supravalvular stenosis and a ventricular septal defect (VSD) coexist. Surgical procedures that relieve pulmonic stenosis but result in chronic pulmonary regurgitation (PR) are more often performed over surgical valve or conduit placement in infancy or early childhood. Thereafter, surgical interventions usually consist of pulmonary valve replacement (PVR) with either bioprosthetic valves or valved conduits. Mechanical pulmonic valve replacement has a low incidence of valve deterioration, need for reoperation and valve thrombosis if used with appropriate systemic anticoagulation4; however, they are not widely used due to various limitations including contraindications to systemic anticoagulation, future need for transcatheter interventions of the pulmonary arterial branches, and somatic outgrowth in infants and children. Bioprosthetic valves and conduits (aortic or pulmonic homografts, Dacron conduits with bioprosthetic valves, Contegra jugular venous valve conduits (Medtronic, Minneapolis, Minnesota, USA)) invariably develop progressive valve dysfunction within 10–20 years following implantation.5
The timing of PVR in PR and/or PS is controversial. Studies evaluating the timing of PVR in patients with severe chronic PR have suggested that normalisation of right ventricular (RV) volume will not occur if severe dilation has already ensued (indexed RV end-diastolic volume >150 mL/m2 or indexed RV end-systolic volume >80 mL/m2).6–8 Furthermore, it is likely that earlier PVR could result in improved exercise tolerance especially in patients with predominant PS.9 10 While there is little evidence that such an approach results in improved clinical outcomes such as decreased mortality, some experts argue that all patients with RV outflow dysfunction (PR, PS or both) should undergo PVR prior to the development of RV dilation or dysfunction.9 The introduction of transcatheter valve therapies is lowering the threshold for PVR, however, this approach must be weighed against the potential for infective endocarditis (IE), procedural risks and decrease in internal diameter of the conduits secondary to multiple transcatheter valve implants.11
Transcatheter PVR (TPVR) can alleviate RV outflow tract (RVOT) conduit dysfunction whether due to stenosis or regurgitation or both. The Melody valve was the first commercially available valve used for this indication and is widely used for the treatment of dysfunctional RV to pulmonary artery (RV-PA) conduits, bioprosthetic valves and dysfunctional native RVOT, with the latter being an off-label use. The valve comes in 18, 20 and 22 mm inner diameter size range, depending on the deployment balloon-in-balloon size, it can also be maximally expanded using a 24 mm balloon,12 which is an off-label use, giving an inner diameter of 24 mm if deployed at nominal pressure (2–3 atm) or an inner diameter of 25 mm if deployed at high pressure (>4 atm). The Melody valve’s outer diameter is approximately 2 mm larger than the inner diameter. The Melody Ensemble delivery system is 22-French in size, and while it is recommended for patients weighing >20 kg, several implantations have been successful in those weighing less.13 The Melody valve can also be deployed using a hybrid surgical approach, circumventing the use of small sized vessels in young children. Melody valve implantation in native RVOT due to either stenosis or regurgitation has been shown to be feasible with prestenting,14 and for those with large RVOT, multiple stenting in Russian-doll style or jailing a branch PA could create a suitable landing zone for the transcatheter valve.15
The other commercially available approved TPVR platform in the USA is the bovine bioprosthetic Sapien XT (Edwards Lifesciences, Irvine, California, USA), it is delivered via a 16–20 French systems and ranges in size from 20 to 29 mm outer diameter deployed with a predetermined volume in the delivery balloon. The third generation of the Sapien valves, Sapien 3, already used commercially in the aortic position, is currently in an ongoing clinical trial evaluating its effectiveness for TPVR (COMPASSION S3 Clinical Trial NCT02744677), and is actively being used by multiple centres for off-label implantation in the pulmonary position, in conduits, bioprosthetic valves and native RVOT (figure 1). The larger diameter Sapien valves (26 and 29 mm outer diameter) allow for implantation in large dysfunctional native RVOTs and conduits than cannot be treated with the Melody valve.

Transcatheter pulmonary valve replacement in native right ventricular outflow tract (RVOT) using a Sapien 3. (A) RVOT angiogram in an anterioposterior projection demonstrating a dilated RVOT and branch pulmonary arteries (PAs) in a patient with repaired tetralogy of Fallot status post pulmonary valvotomy. (B) Lateral view of dual balloon sizing of the PA with simultaneous aortic root angiogram showing no evidence of coronary or aortic compression. (C) RVOT angiogram in a lateral projection following Sapien 3 valve deployment. (D) Final PA angiogram showing no residual pulmonary regurgitation or perivalvular regurgitation post-Sapien valve deployment.
Additionally, TPVR has been performed successfully within failed bioprosthetic valves using either the Melody or Sapien valve with excellent outcomes.16
The treatment of large diameter (>30 mm) native RVOTs require either narrowing of the RVOT17 or new larger valve platforms. The Venus P valve (Venus Medtech, China) and the Harmony valve (Medtronic, Minneapolis, Minnesota, USA) are self-expanding covered hourglass-shaped RVOT reducer platforms with the valve in the central waist. The Venus P valve has been safely implanted and early data have demonstrated improvement in haemodynamics and RV volume, while the early feasibility studies of the Harmony valve showed improved haemodynamics, and only mild PR 1 year after implantation.18 19 The Harmony valve is currently in phase III multicentre clinical trial in the USA (The Medtronic Harmony TPV Clinical Trial NCT02979587).
The majority of published data pertains to the TPVR with the Melody valve. Short-term and intermediate outcomes of the Melody valve have shown valve durability, significant haemodynamic and clinical improvements, and a 5-year freedom from reintervention of 76%,20–22 the improvement in functional capacity is more evident in patients with pulmonary valve/conduit stenosis versus those with only regurgitant lesions.10 Studies on long-term outcomes are still needed to evaluate valve durability and freedom from reintervention over greater than 5 years, including both Melody and Sapien valves.
Stent fracture and endocarditis have been the principal causes for reintervention.23 The Melody valve stent fracture often occurs in patients with conduits or native RVOT dysfunction and is likely due to repetitive stress on the platinum iridium frame. The rate of stent fracture in the literature has ranged from 5% to 25% of implants, however, the majority are type I stent fracture without loss of stent integrity, which are of little clinical significance and rarely necessitate intervention, while type II (stent fracture with loss of stent integrity) and type III (stent fracture with embolisation of stent fragments) usually require intervention. Prestenting before Melody valve placement has significantly reduced the rate of clinically significant stent fracture24 (figure 2). Transcatheter valve-in-valve implantation is often used as a successful treatment concept for Melody valve stent fracture. Stent frame fracture is rare with Sapien TPVR even in the absence of prestenting, this is likely due to the more durable cobalt–chromium stent platform.

Transcatheter pulmonary valve replacement in right ventricular to pulmonary artery (RV-PA) conduit using a Melody valve with prestenting. (A) PA angiogram in an anterioposterior cranial projection demonstrating severe pulmonary regurgitation (PR) in a patient with pulmonary atresia status post RV-PA homograft placement and unifocalisation. (B) Lateral projection of the PA angiogram shown in (A) demonstrating severe PR and mild narrowing of the distal homograft. (C) PA angiogram in an AP cranial projection following prestenting with multiple stents including a covered Cheatham Palmaz stent and Melody valve placement. (D) Lateral projection of the PA angiogram shown in C demonstrating resolution of the PR.
There is a growing body of literature describing IE in TPVR. The incidence of IE in the literature ranges from 3% to 25%, and has been reported as early as 1 month, and up to 4.7 years postprocedure, with most cases of IE due to staphylococcal and streptococcal species, and approximately 13% requiring reintervention.25–29 Factors that may be associated with increased risk of IE include male gender, lack of use of spontaneous bacterial endocarditis (SBE) prophylaxis with dental procedures, instrumentation without antibiotic prophylaxis, poor dental health, nail biting, prior episodes of endocarditis, elevated peak gradient across the RVOT and surgical conduits (vs native RVOT), multiple stents, and abrupt discontinuation of antiplatelet therapy. The latter is postulated to be due to tropism of bacteria to thrombus, and while one study did not note an association, there has been some literature regarding the use of Aspirin as prophylaxis for endocarditis.30 31 Some studies have proposed that bovine jugular veins, such as the Melody valve and the Contegra valved conduit have an inherently increased risk of endocarditis due to greater bacterial adhesion.27 The strict adherence to SBE prophylaxis, antiplatelet therapy and close monitoring is imperative for prevention. Sapien TPVR IE does occur, however, because Sapien TPVR has not been performed as long as Melody TPVR, data are lacking on the long-term risk of IE in Sapien TPVR.32
Other complications such as PA or conduit dissection or rupture are life threatening but rare, and can be treated with covered stent placement. There is a 5%–6% risk of coronary artery compression noted on balloon compression testing of the RVOT/conduit, which precludes these patients from undergoing TPVR in most cases.33 34 The standard practice is to test for coronary compression using a balloon the same size as the largest stent or valve intended for use in the conduit/RVOT. Aortic compression may also occur in native RVOT interventions, but is an infrequent complication.35 While valve embolisation is a rare complication, it can usually be averted with adequate preprocedural planning and RVOT sizing. If the valve does embolise and cannot be safely deployed in a distal PA branch or vena cava, surgical removal may be necessary.
Tricuspid valve
Primary tricuspid valve dysfunction in patients with CHD is often associated with Ebstein’s anomaly or congenital dysplasia, which may result in chronic severe tricuspid regurgitation (TR). Tricuspid valve regurgitation may occur secondary to RV volume or pressure overload due to progressive RV and tricuspid annular dilation. While it is common for patients with RVOT dysfunction to develop secondary TR, it may improve post-PVR/TPVR.36 TR is often well tolerated, yet, much like PR, clinical sequelae will eventually emerge. Surgical repair for tricuspid valve dysfunction include the placement of annular bands or rings as well as more complex operations to relocate or augment the tricuspid valve leaflets, as in Ebstein’s anomaly. If surgical valve replacement is warranted, bioprosthetic valves are preferred due to concerns over increased risk of mechanical tricuspid valve thrombosis. Most bioprostheses require replacement within a decade as they often become dysfunctional over time due to leaflet thickening and dysfunction with laminar thrombi often evident on pathological samples.37 Indications for intervention include regurgitation or stenosis with right heart failure symptoms, as well as arrhythmias.
Transcatheter tricuspid valve replacement (TTVR) is feasible and there is growing evidence for the use of the Melody and Sapien valves in both rings and failing tricuspid valve bioprostheses (figure 3). The procedural success rate is high and short-term haemodynamic benefits are evident, but there remains a paucity of intermediate and long-term data. Perivalvular regurgitation is common when TTVR is performed in surgical bands and rings, but is mild in most cases and can frequently be managed with a variety of transcatheter occlusion devices.38–41 There are reports of successful TTVR in high-surgical risk patients with tricuspid atresia who have undergone right atrial to RV valved/non-valved connection (Bjork Fontan).39

Transcatheter systemic tricuspid valve-in-ring replacement via transapical approach using a Sapien XT valve. (A) Axial CT angiogram image of the systemic tricuspid valve ring and the hypertrophied systemic right ventricle in a patient with D-transposition of the great arteries status post-Mustard repair (atrial switch) with severe systemic tricuspid regurgitation (TR). (B) Three-dimensional print of the systemic right ventricular (RV) and tricuspid annular ring with bench testing with a Sapien 3 transcatheter valve. (C) Systemic RV angiogram in an Right Anterior Oblique (RAO) projection demonstrating severe systemic TR and the indwelling tricuspid valve ring. (D) Systemic RV angiogram in an RAO projection following Sapien XT valve placement within the indwelling ring demonstrating resolution of the severe systemic TR. sRA, systemic right atrium; sRV, systemic right ventricle.
There are a number of off-label and investigational devices being used for transcatheter tricuspid valve repair that are not yet widely used in the congenital population.
Single ventricle with Fontan
There are case reports of implanting a Melody valve in failing Fontan patients as a method for palliation, in an attempt to improve forward flow and thus cardiac output, as well as decrease venous congestion. Of the four cases in which this procedure was performed, one patient died from ventricular fibrillation, potentially due to adrenal insufficiency unrelated to the procedure, two cases showed Melody valve malfunction and one case showed resolution of protein losing enteropathy (PLE) with good function of the Melody valve on subsequent follow-up.42 Further research is needed in this field especially as the lack of pulsatility in the Fontan conduit can lead to early valve dysfunction as noted in these case reports.
Aortic valve
Aortic stenosis (AS) or aortic regurgitation (AR) in CHD is due to either a primary valvular lesion or from secondary dysfunction. For AS, the clinical spectrum varies from isolated congenital AS, typically due to bicuspid pathology, to more complex multilevel abnormalities such as hypoplastic left heart syndrome where severe AS occurs in concert with aortic hypoplasia and mitral hypoplasia or atresia. AR often occurs along with AS in patients with bicuspid aortic valve but can also occur secondary to aortic root dilation, aortic valve prolapse or as a consequence of leaflet damage as seen from sub-AS, membranous VSD or IE. Both AS and AR can occur following aortic valve repair or replacement with bioprostheses, homografts or pulmonary autografts as in the Ross or arterial switch operations.
Transcatheter aortic valve replacement (TAVR) has become a widely used alternative to surgical aortic valve replacement predominantly in patients with calcific aortic valve stenosis at moderate to high surgical risk, with overall good outcomes. Potential complications of TAVR include perivalvular leak, conduction abnormalities, thromboembolism, valve embolisation, aortic root rupture, coronary occlusion and iliac artery rupture.43 TAVR in AS due to bicuspid aortic valve has been shown to be feasible and effective with favourable valve performance, and similar outcomes as TAVR in trileaflet AS, and while some studies demonstrated a higher rate of PVL compared with TAVR in trileaflet AS, the newer generation valves, such as the Sapien 3 and the Lotus valve show lower rates of perivalvular leak (PVL).44 45 In our experience, TAVR in patients with other forms of CHD is feasible, such as a patient with D -transposition of the great arteries status postarterial switch and valve sparing aortic root repair with recurrent AR (figure 4).

Transcatheter aortic valve replacement using a Sapien 3 valve. (A) Transoesophageal echocardiogram and colour Doppler demonstrating severe aortic regurgitation (AR) in a patient with D -transposition of the great arteries status postarterial switch and prior valve sparing aortic root repair with a 22 mm hemashield graft. (B) Aortic root angiogram demonstrating severe AR, also note reimplanted coronary arteries distant from the aortic valve (black arrow). (C) Sapien 3 (26 mm) positioned across the aortic valve with simultaneous aortic root angiography. (D) Left ventricular angiogram in a Right Anterior Oblique (RAO) projection status postdeployment of the Sapien 3 across the aortic valve.
A large number of newer generation valve platforms are in preclinical or early clinical testing for treatment of AR, congenital aortic valve disease such as bicuspid or unicuspid valves are excluded from these early trials. These newer technologies aim to provide improved valve function, higher effective orifice areas, lower rates of PVL, superior deliverability and easier positioning and repositioning. These include the Centera valve (Edwards Lifesciences) and the Lotus Valve (Boston Scientific, Valencia, California, USA). Other valve systems are also equipped with anchoring techniques allowing more precise deployment and stability in primary AR, they include the Engager Valve, JenaValve (JenaValve, Irvine, California, USA), Accurate valve (Symetis/Boston Scientific, Marlborough, Massachusetts, USA), Portico valve (St. Jude Medical, Saint Paul, Minnesota, USA) and the Helio docking system for the Sapien XT/S3 valve (table 1). These platforms will expand the transcatheter valve replacement technology to patients with predominant AR without AS or annular calcifications, and their use in the CHD population is yet to be established.
Transcatheter valves
Mitral valve
Congenital mitral valve abnormalities may result in regurgitation, stenosis or occasionally both. Congenital mitral stenosis (MS) may occur at the suprannular, annular, valvular or subvalvular level such as in cor triatriatum, supramitral ring, double-orifice mitral valve, parachute mitral valve or hammock mitral valve. MS may be an isolated lesion or occur in association with other left heart lesions, the latter being more common. Abnormalities of any portion of the mitral valve apparatus can lead to mitral regurgitation (MR). Residual anterior mitral leaflet clefts following surgical repair of endocardial cushion defects often results in significant MR. Myxomatous mitral valve degeneration due to connective tissue disease can also lead to MR via prolapse or chordal rupture. Malcoaptation of the mitral leaflets results from progressive annular dilation with resultant ‘functional’ MR due to ventricular enlargement and cardiomyopathy.
Surgical interventions for MR include a variety of repair techniques which may include the placement of a surgical ring or mitral valve replacement with mechanical, or bioprosthetic valves. Bioprosthetic valves require replacement due to progressive dysfunction within 10–15 years from implant.46 The field of transcatheter interventions of the mitral valve is still in its infancy and there are many still in the preclinical or early clinical phase.
The MitraClip is a 4 mm cobalt chromium, polyester-covered clip that grasps the valve leaflets leading to the creation of a double orifice, mimicking the surgical ‘Alfieri stitch’. It is indicated for treatment of symptomatic severe primary MR in patients with suitable anatomy at prohibitive risk for surgery. It can be of use in the treatment of myxomatous and functional MR in patients with CHD (figure 5).

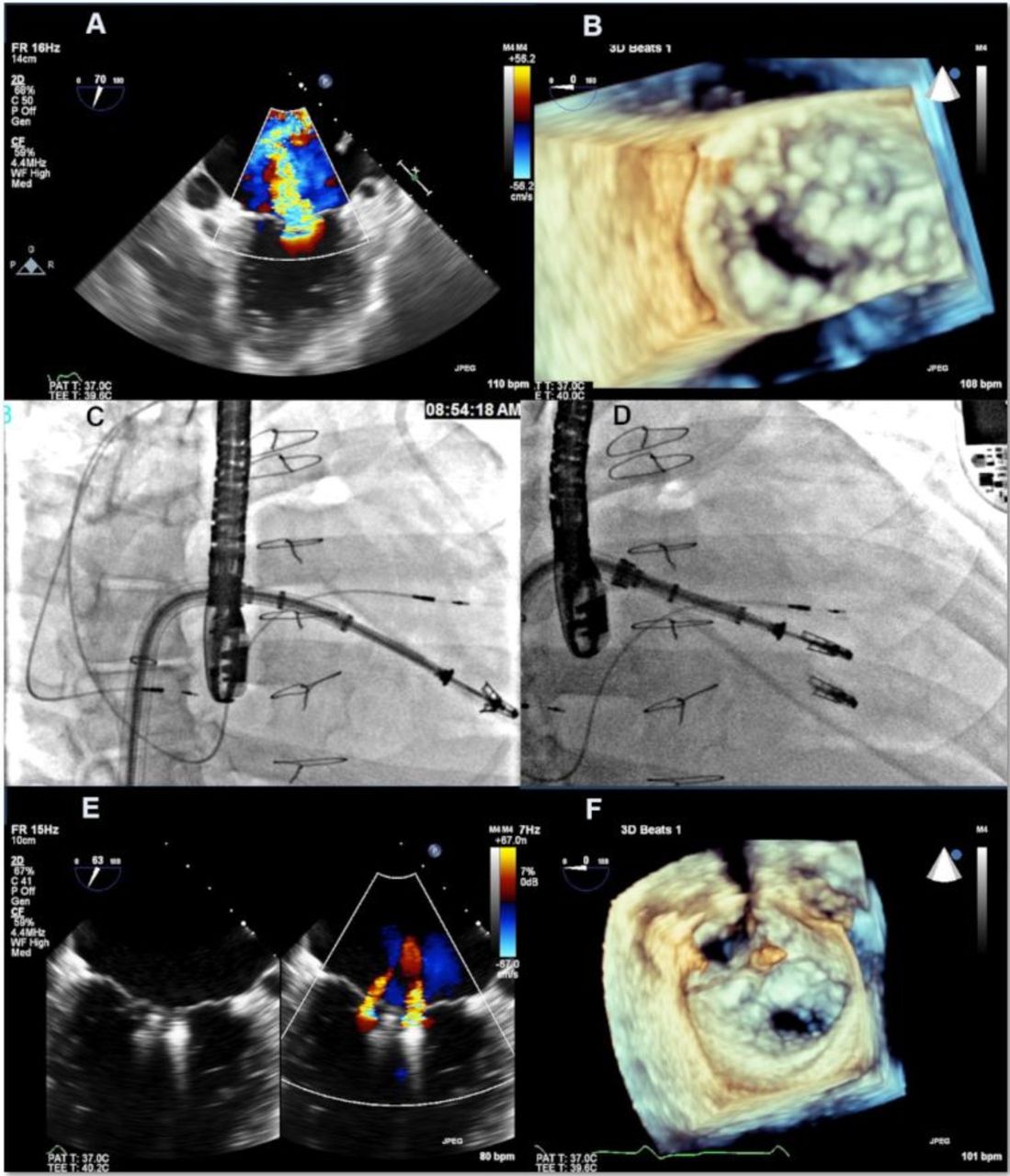
Transcatheter MitraClip repair of the mitral valve. (A) TEE view with colour Doppler of the mitral valve in a 39-year-old woman with tricuspid atresia s/p right atrium-RVOT Fontan demonstrating severe central with myxomatous mitral leaflets and dilated LV with poor leaflet coaptation. (B) 3D TEE view in systole demonstrating malcoaptation of the mitral valve. (C) MitraClip delivery system advanced across Fontan baffle. (D) Second MitraClip deployment. (E) TEE image with colour Doppler comparison following MitraClip deployment demonstrating reduction in MR from severe to mild. (F) 3D TEE view following MitraClip deployment demonstrating the creation of a double orifice mitral valve. LV, left ventricular; MR, mitral regurgitation; RVOT, right ventricular outflow tract; TEE, transoesophageal echocardiogram.
Other novel devices being developed for transcatheter mitral valve repair as well as transcatheter mitral valve replacement are still in the preclinical or early clinical phase. Most procedures performed are in the valve-in-valve and valve-in-ring population47 and in those with calcified mitral annuli to allow for anchoring. The valves that have been used most widely are the Melody and Sapien valves (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
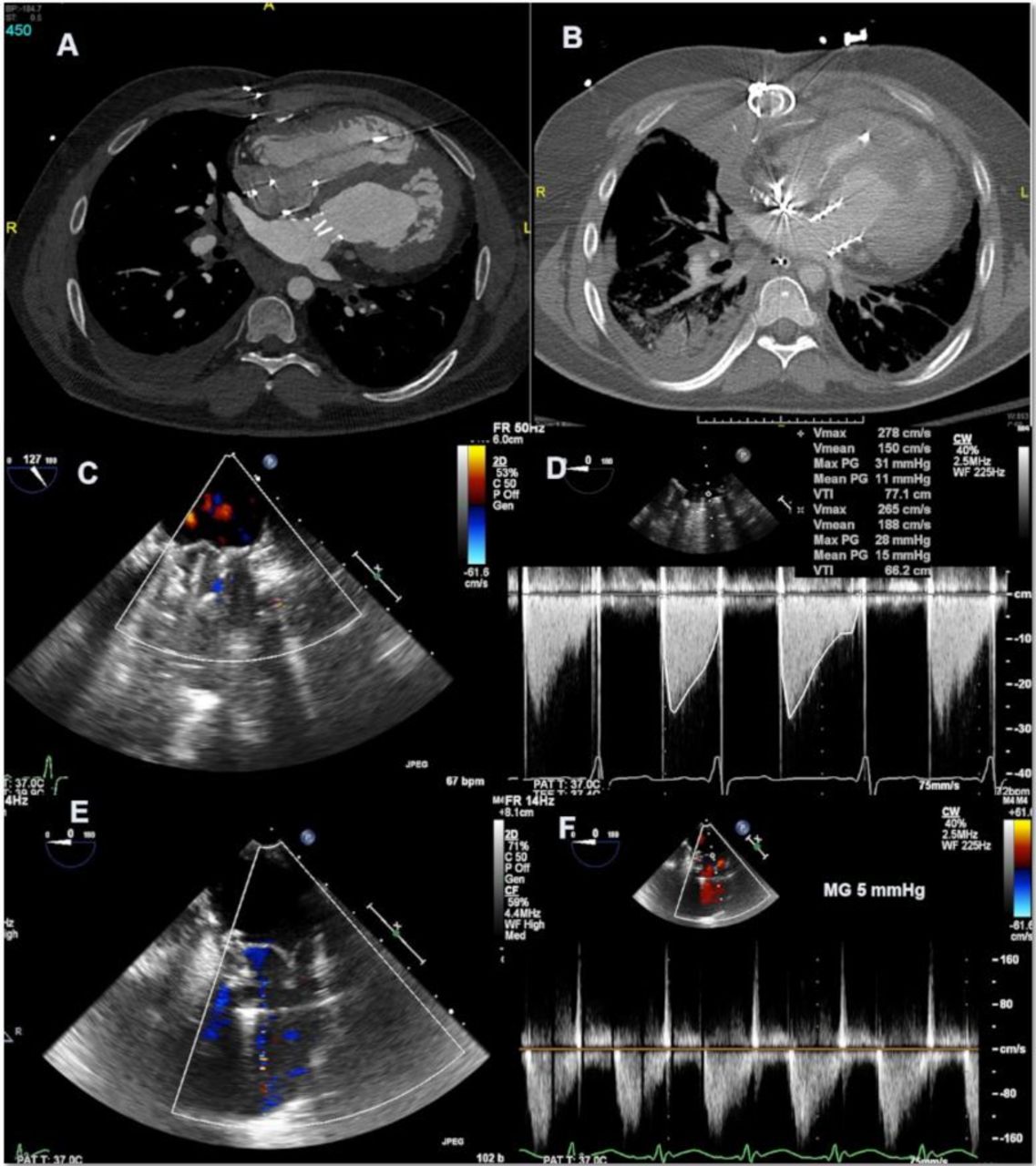
Transcatheter mitral valve replacement in a hybrid procedure using a Sapien 3 valve. (A) Axial ECG-gated CT angiogram (CTA) demonstrating a mechanical mitral prosthesis in a patient with Shone’s complex. (B) Axial CTA postsurgical removal of the mechanical mitral valve and hybrid deployment of a Sapien 3 valve (26 mm) in the mitral position. (C) Transoesophageal echocardiogram (TEE) with colour Doppler of the mechanical mitral valve. (D) Continuous wave (CW) Doppler across the mechanical mitral prosthesis demonstrating diastolic flow acceleration with a mean gradient of 15 mm Hg consistent with severe mitral stenosis due to patient–prosthesis mismatch. (E) TEE with colour Doppler image of the Sapien valve in systole demonstrating no mitral regurgitation. (F) CW Doppler across the Sapien valve with a mean gradient of 5 mm Hg.
Other transcatheter valve uses
Hybrid procedures involve the use of trancatheter valve technology in combination with surgical entry into the chest in an attempt to minimise surgical morbidity by avoiding or minimising cardiopulmonary bypass or by avoiding a redo sternotomy. Examples include performing a surgical PA plication then deploying a transcatheter valve via a subxiphoid incision and ventriculotomy, or surgically removing a prosthetic mitral valve and direct implantation of the transcatheter valve under direct visualisation on cardiopulmonary bypass. Furthermore, the Melody valve has been modified and surgically placed in all four valvular positions as an expandable valve in infants and children allowing for future balloon dilations and by that accommodating somatic outgrowth, hopefully reducing the number of future surgeries.48 49
Importantly, while transcatheter valve implantation in CHD is reducing the need for surgical intervention, with its associated morbidities, as well as getting women through childbearing age without the need for systemic anticoagulation as would be necessary with mechanical valves, the trade-off is the concern for valve durability, and the need for reintervention relative to the surgical valves, especially as these valves are being implanted at a much younger age in patients with CHD. Furthermore there is the risk of IE, and the likelihood of a progressively smaller effective orifice area with multiple valve-in-valve implantations. There is still an overall paucity of data on valve durability, however, a recent systematic review of 8914 patients (>18 years old) who underwent TAVR had a rate of structural valve deterioration of approximately 7% at 5 years, however, the mean age of these patients was in the 80s, and Melody valve was not included, and there remains the question of whether structural deterioration rates of trancatheter valves differ in the paediatric, young adults and elderly populations.50
Summary and conclusion
Transcatheter valve replacement in patients with pulmonic conduit or bioprosthetic valve dysfunction has become the new standard of care. These minimally invasive techniques have allowed for a reduction in the number of cardiac surgeries needed over the lifetime of the patient with CHD. There is immense potential for advances in technology with increasing application to lesions previously only surgically treated such as PR in native RVOT, primary AR, and native MR and TR. An interdisciplinary team approach, with incorporation of hybrid procedures when necessary in addition to preprocedural planning with the use of multiple imaging modalities is integral to procedural success. Longer follow-up data are needed to determine the longevity of the available transcatheter valve platforms when compared with surgical valves.
Key messages
Transcatheter valve replacement is feasible in all four positions in the congenital heart disease patient population; however, most are carried out in the pulmonary position.
Hybrid procedures expand the use of transcatheter valves and reduce surgical morbidity in select patients.
Newer generation valves will expand the use of transcatheter valve replacement to native right ventricular outflow tract , native mitral valve, tricuspid valve and primary aortic regurgitation.
Tricuspid and mitral valve-in-valve and valve-in-ring are associated with favourable short-term haemodynamic results.
Long-term outcome studies are needed to assess longevity relative to surgical valves.
Native tricuspid and mitral valve percutaneous repair is feasible using commercially available technology.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
References
Footnotes
Contributors All authors listed have contributed sufficiently to the project.
Funding This research received no specific grant from any funding agency in the public,commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Commissioned; externally peer reviewed.
Author note References which include a * have been selected as key references for this paper.