Article Text

Statistics from Altmetric.com
Learning objectives
To understand the principles of assessment by type of non-cardiac surgery, the Revised Cardiac Index Risk score, the grade of valve disease and functional capacity.
To understand that adverse events at non-cardiac surgery result from associated coronary disease and the haemodynamic effects of the valve disease.
To understand the precautions necessary during and after non-cardiac surgery and when invasive intervention is indicated in severe aortic stenosis or mitral stenosis.
Introduction
Valve disease is a major concern in patients having non-cardiac surgery. First, it is common (table 1)1–4 particularly in the elderly who may also have other comorbidities. The adult population prevalence of moderate or severe disease is 2.5% and this rises to >13% in people aged ≥75.1 Second, valve disease is often asymptomatic and may be detected for the first time during preoperative assessment for non-cardiac surgery. In the OxVALVE community study,3 moderate or severe valve disease was known in 4.9% people aged >65 and was newly detected by screening in a further 6.4%. Third, valve disease, particularly aortic stenosis (AS), may be associated with coronary disease which contributes to the perioperative risk.5 Fourth, recognised competencies in heart valve disease6 7 are not universal in all disciplines caring for patients having non-cardiac surgery. Finally, the evidence base is small. A combination of these factors leads to anxiety over the presence of valve disease although this is often misplaced.
Prevalence (%) of moderate or severe valve disease
This article discusses the assessment and perioperative management of patients with heart valve disease including replacement valves.
An approach to valve disease
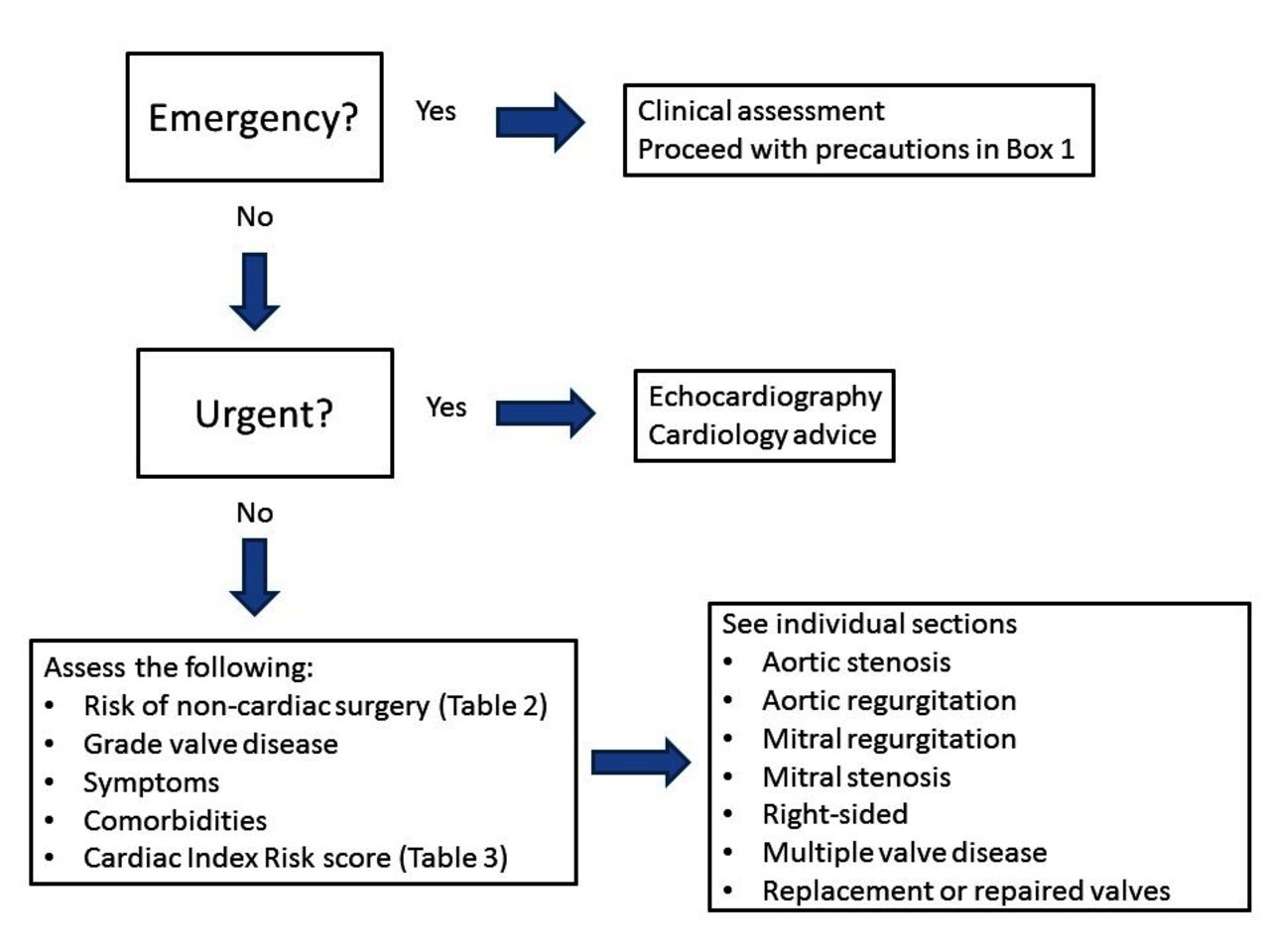
If emergency life-saving surgery is needed, this should proceed immediately (figure 1).8–11 If severe valve disease is known or suspected from the history or the presence of a significant murmur, additional precautions should be taken in perioperative care (box 1).

An approach to valve disease.
Perioperative care of patients with severe valve disease
(A) Preoperative
Recognise the possibility of valve disease from the history and the presence of a significant murmur.
Obtain an echocardiogram unless a study is available (for review by the cardiologist/imager) within 3 months for severe disease or 6 months for previously moderate disease (which might have progressed).
Expert preoperative assessment by imaging specialist, cardiologist with valve competencies and ideally cardiac anaesthetist.
(B) During the operation
For all valve disease
Experienced anaesthetist and surgeon.
Invasive blood pressure monitoring.
Central venous line to give inotrope/constrictors and monitor filling pressures.
Treat hypotension aggressively.
Maintain venous filling pressures.
If pulmonary artery pressure high (mitral stenosis, aortic stenosis, mitral regurgitation) avoid hypoxia, hypercarbia, acidosis).
Treat electrolyte imbalance particularly serum potassium.
Aortic stenosis 44
Avoid venous and arterial dilators (including epidural block unless this can be done without vasodilatation).
Maintain normal or high peripheral resistance.
Correct arrhythmia quickly.
Avoid bradycardia and tachycardia.
Aortic regurgitation
Avoid drugs that slow the heart rate. Keep rate around 90 bpm.
Mnemonic: fast (control heart rate), full (maintain filling), forward (reduce peripheral vascular resistance).
Mitral stenosis
Avoid arterial vasodilators.
Maintain heart rate 50–60 bpm.
Inotropes for right ventricular dysfunction.
Mitral regurgitation
Maintain heart rate 80–100 bpm.
Inotropes if pulmonary artery pressure high.
Mnemonic: fast (control heart rate), full (maintain filling), forward (reduce peripheral vascular resistance).
(C) Postoperatively
High dependency or intensive care nursing.
Avoid fall in preload. Scrupulous attention to fluid balance and oxygenation.
Treat electrolyte imbalance. Maintain serum potassium 4.5–4.9 mmol/L.
Treat hypotension aggressively.
Correct new arrhythmia quickly.
Scrupulous pain relief.
The surgery may be urgent, for example, for a hip fracture or cancer. This should be delayed if feasible for echocardiography and a cardiological opinion. A flow murmur may be found in 20%–30% of the general population12 13 particularly in sick patients with a tachycardia, fever or anaemia. Echocardiography is indicated for any murmur other than an obvious flow murmur confirmed by an experienced clinician and especially if there is a potentially cardiac symptom, (breathlessness, chest pain or altered consciousness). Approximately, one-third of patients with heart failure have associated valve disease14 and atrial fibrillation is also strongly associated with valve disease.3 15 Routine echocardiographic screening in the elderly is not indicated. Although severe AS was shown in 8%16 of elderly patients with a hip fracture, all could have been identified from the presence of a murmur. If valve disease is already known, urgent echocardiography is not usually necessary if there is an echocardiogram within 6 months in a patient with moderate disease or within 3 months with severe disease, but the opinion of a cardiologist with competencies in valve disease should still be sought especially if cardiac symptoms have developed.
The majority of patients in whom a murmur is detected are being assessed for elective non-cardiac surgery. In these the management depends (figure 2) on the type of surgery (table 2), on the grade of valve disease, and the left ventricular (LV) and right-sided compensation to that valve disease.8–11 It also depends on the cardiac risk score (table 3) and on the patient’s functional capacity (figure 3).8–11 There is no need for further assessment in patients having low-risk non-cardiac surgery. Low-risk surgery includes knee (but not hip) replacement. The ability to walk for 7 metabolic equivalents (Mets) without symptoms based on the history is usually taken as sufficient functional capacity for the purposes of elective non-cardiac surgery of intermediate or high risk.9 However, ideally, as for any patient with severe valve disease being assessed routinely in a specialist heart valve clinic, formal exercise testing should be performed to confirm lack of symptoms. Valve disease progresses so there is a ‘shelf life’ for an assessment before non-cardiac surgery with a long waiting time such as cadaveric renal transplantation or hip replacement. Serial assessment should be planned or elective intervention undertaken earlier than generally indicated. The risk of the non-cardiac surgery may be higher than the guideline categories in table 2 if the planned surgery is extensive or a redo or the patient has significant comorbidities. Relatively minor nasal surgery may still be of concern in a patient with asymptomatic severe AS if induced hypotension is required. A multidisciplinary case conference should be considered in these cases.
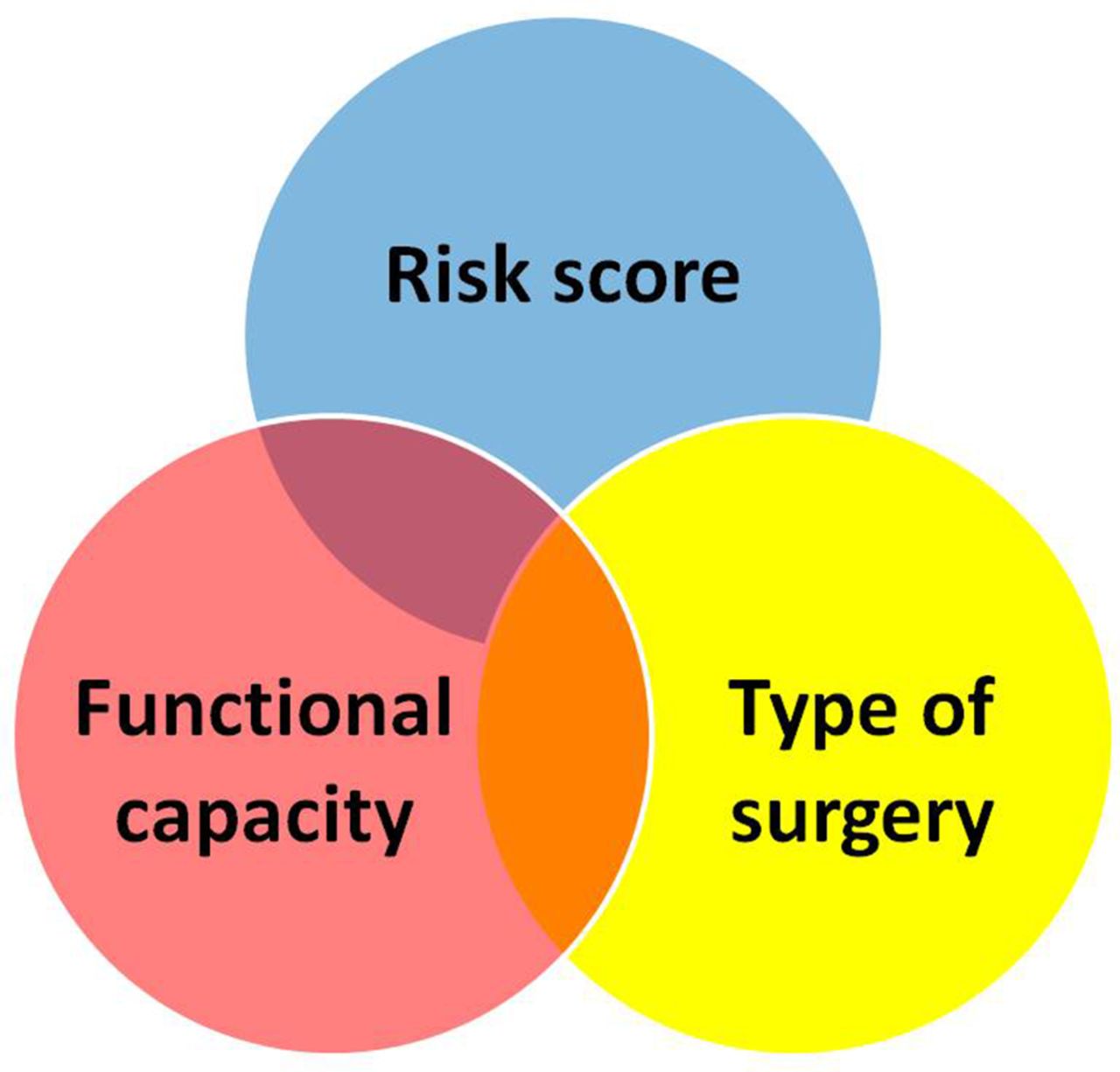
Risk of surgery. This depends on the grade of valve disease and left ventricular and right ventricular compensation, the risk of the non-cardiac surgery, the functional capacity and the cardiac index risk score.

Exercise capacity. Exercise capacity judged from the history is taken as sufficient for non-cardiac surgery if it exceeds at least 4 Mets or ideally 7 Mets. However, it remains preferable to corroborate the history using exercise testing (reproduced from Kristensen et al 9).
Risk of non-cardiac surgery
Revised Cardiac Index Risk score17 18*
The risk in patients with valve disease is determined by the haemodynamic effect of the valve disease and LV compensation and by the risk of coronary events which, as for patients without valve disease, can be assessed by the Cardiac Index Risk score (table 3).17 18 Aortic sclerosis is well known to be a marker of occult coronary disease.19 20 If the Cardiac Index Risk score is ≥2 in a patient having high-risk non-cardiac surgery and with poor (<4 Mets)(figure 3) or unknown exercise capacity (eg, because of limiting peripheral vascular disease or severe hip pain) then a functional test for coronary disease should be considered even in mild valve disease.8 9
Patients should also be assessed for the presence of comorbidities which will affect the risk of invasive intervention for valve disease. In general, if intervention is indicated in its own right for symptoms or LV decompensation, this should be done before elective non-urgent non-cardiac surgery.
Aortic stenosis
AS still tends to be seen as a high-risk condition. The National Confidential Enquiry into Perioperative Deaths in the UK in 200121 showed that approximately one death from inadequately assessed or managed AS occurred each year at every trust in the UK. The report stated, “Any asymptomatic murmur may indicate significant disease”. This may have exaggerated the perceived frequency of the risk from AS since a systolic flow murmur is common before surgery.
In fact the risk from severe AS is not high if it is asymptomatic. Early studies were in small populations including patients with symptoms or impaired LV function and also included emergency as well as elective non-cardiac surgery.22 In patients with asymptomatic severe AS undergoing intermediate-risk or high-risk surgery, 30-day mortality and postoperative myocardial infarction rates are similar to those in control subjects (figure 4).5 20 23 The risk in normal LV ejection fraction (EF) low flow AS appears not to be higher than normal flow AS.20 However, there is a risk of events in moderate as well as severe AS. In one study, the risk of myocardial infarction was 3.5% for severe AS, 2.3% for moderate AS and 1.0% for controls.5 This may have been partly from imperfect grading since patients with moderate AS and events had effective orifice areas (EOAs) close to 1.0 cm2 and LV EF <40%5 but may have been partly because of associated coronary disease.5 Exercise testing is therefore indicated for patients with asymptomatic moderate AS in whom symptoms are revealed in up to 30% compared with 40% in severe AS.24 25 Symptoms and a fall in blood pressure but not ST-segment depression mark high-risk AS.10 24

Outcomes are less good in the presence of symptoms20 with a mortality of 9.4% compared with 3.8% in control subjects (p=0.097) and a rate for all major cardiovascular events of 28.3% compared with 8.5% (p<0.0001).20 Outcomes are also worse with coexistent mitral regurgitation (MR) or tricuspid regurgitation (TR),5 atrial fibrillation,20 impaired LV function (LV EF <40%)5 or coronary disease including a revised cardiac index risk score ≥2.5 20 26 However, the need for emergency non-cardiac surgery is the dominant determinant of risk with a 30-day mortality of 25% in severe AS and 23.8% in control subjects.20
Thus, asymptomatic severe AS is not a contraindication to low-risk or intermediate-risk non-cardiac surgery (figure 5). According to current guidelines8 9 surgical or transcatheter aortic valve replacement (TAVI) is indicated for symptoms or if patients with asymptomatic severe AS are having high-risk non-cardiac surgery and the risk of the cardiac intervention is acceptable. This judgement may be hard but the total risk of the cardiac intervention, the delay until the non-cardiac procedure and then the risk of this surgery soon after a replacement operation has to be discussed. It may be lower risk overall in individual cases to proceed with the non-cardiac surgery. Furthermore severe AS ranges from ‘just above moderate’ to ‘critical’ with a wide variation in natural history and haemodynamic effects. Events at non-cardiac surgery appear unlikely in the presence of normal LV EF, no significant coexistent valve disease, a mean aortic valve gradient <50 mm Hg and EOA 0.8–1.0 cm2.22 If there is symptomatic severe AS and the non-cardiac surgery is urgent, for example, cancer surgery and must be done before surgical or transcatheter intervention can be performed balloon aortic valvotomy can be considered.9 10

Flow chart for managing severe aortic stenosis (AS). Moderate to severe AS is associated with an increased risk of events after non-cardiac surgery possibly because of associated coronary disease. These patients as well as those with severe AS should be considered for formal exercise testing to exclude symptoms (redrawn from Baumgartner et al 10). AVR,aortic valve replacement; BAV, balloon aortic valvotomy;EF, ejection fraction; LV, left ventricular.
Aortic regurgitation
There is no increased risk of events in any grade of non-cardiac surgery even if the aortic regurgitation (AR) is severe provided that the patient is asymptomatic and the LV is compensated (figure 6). Formal exercise testing should be considered to confirm lack of symptoms.
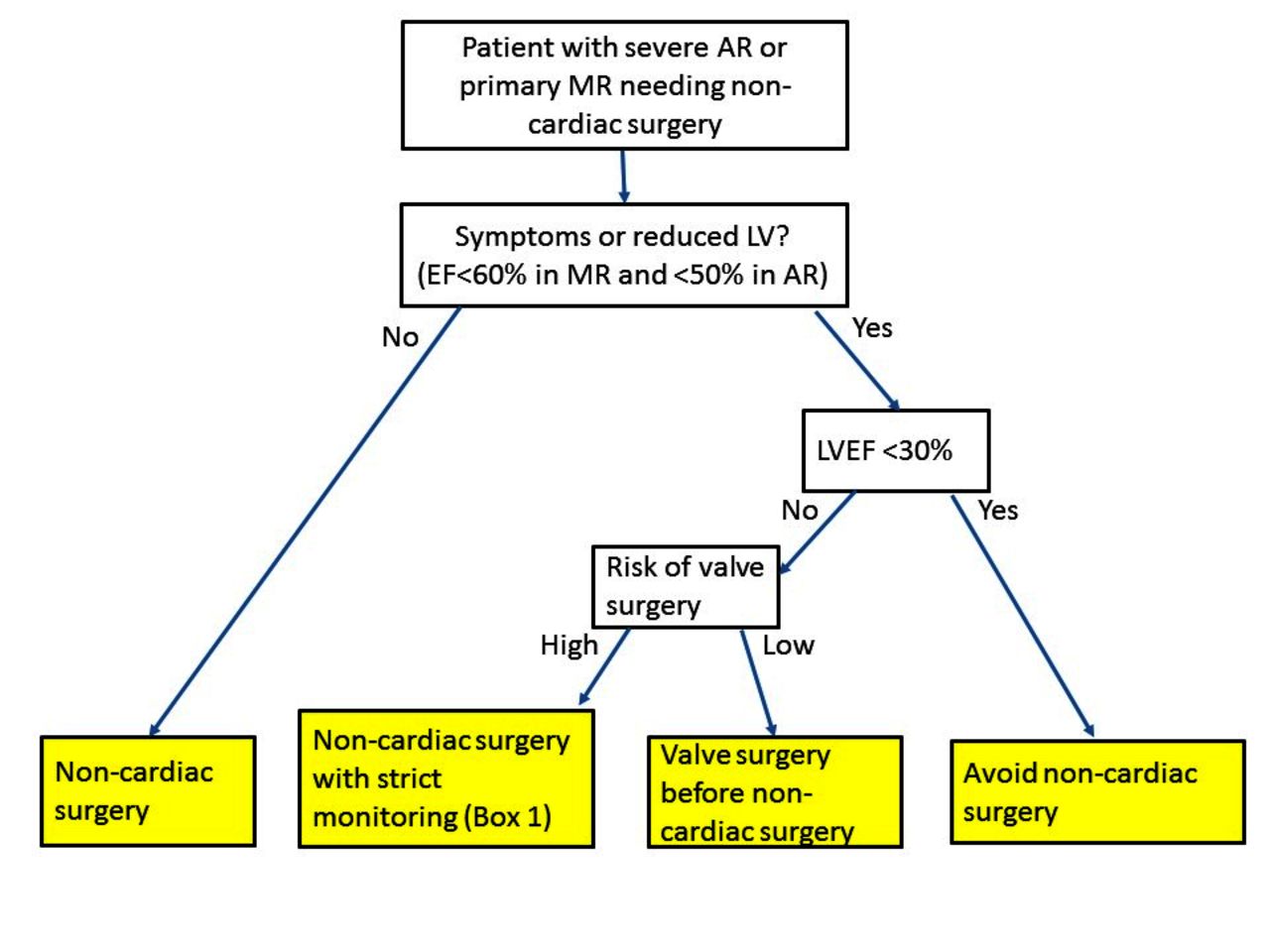
Flow chart for managing severe aortic and primary mitral regurgitation. AR, aortic regurgitation; EF, ejection fraction; LV, left ventricular; MR, mitral regurgitation.
In a small elderly population27 with a mix of moderate to severe and severe AR with variable LV function, the in-hospital death rate was 9% compared with 1.8% for matched controls. Multivariate determinants of death were reduced LV function, high-risk non-cardiac surgery and lack of cardiac medication.
Patients with significant symptoms should have aortic valve surgery if feasible before non-cardiac surgery. If the non-cardiac surgery is relatively urgent in the context of mild symptoms or mild LV dysfunction then in individual cases it may be appropriate to manage medically with diuretic and either an ACE inhibitor or angiotensin II receptor blocker and proceed with non-cardiac surgery.9 10 Beta blockers should be avoided since bradycardia increases the time for regurgitation to occur. Guidelines suggest avoiding non-cardiac surgery if the LV EF is <30%.8 9
Mitral regurgitation
For primary MR, there is no increased risk of events in any grade of non-cardiac surgery (figure 6) even if the regurgitation is severe provided that the patient is asymptomatic and the LV is compensated.9 If the history is uncertain, a formal exercise test should be performed to confirm lack of symptoms. Patients with recognised indications for mitral valve surgery should have this if feasible before non-cardiac surgery. If not feasible perhaps because the non-cardiac surgery is for cancer, this can be undertaken with increased perioperative care (box 1). Beta blockers may reduce regurgitant fraction but no adequate data exist to recommend their routine use in this situation. There is no evidence to recommend ACE inhibitors for severe MR without LV decompensation. However, full heart failure therapy should be started for patients with LV decompensation who are not suitable for valve surgery. Guideline advice is not to proceed with non-cardiac surgery if the LV EF is <30%9 although clearly LV impairment can be severe at a LV EF above this level.
For patients with secondary MR, the risks are affected by LV function and by the presence of coronary disease as well as the haemodynamic effects of MR. Functional testing usually with stress echocardiography should be performed to guide coronary angiography and subsequent coronary intervention. Lai et al 28 reported results for 84 patients with moderate to severe or severe MR detected retrospectively from 87 740 low-risk or intermediate-risk non-cardiac procedures performed between 1999 and 2004. The aetiology of the MR was not reported, but coronary disease was known in 28% and the mean EF for the group was low at a mean 44% (SD 15%). The event rate at surgery was low with 31% having minor hypotension or easily correctable bradycardia. However, 27.4% had pulmonary oedema or required prolonged intubation after surgery and 11.9% died. The main independent predictor of death was preoperative atrial fibrillation while LV EF did not attain statistical significance although 50% who died had an LV EF <35% (range 12%–32%). Bajaj et al 29 also reported a higher than expected incidence of cardiovascular events (30 days death, heart failure, acute myocardial infarction and stroke) occurring in 39.2% with ischaemic MR, compared with only 13.3% with non-ischaemic MR and 16.4% of propensity matched controls.
Patients with functional MR should have full heart failure medication including beta blockers. The decision to undertake non-cardiac surgery has to be taken on an individual basis. The precautions in box 1 are important particularly control of loading conditions since secondary MR is heavily load dependent. As for primary MR, guideline advice is not to proceed with non-cardiac surgery if the LV EF is <30%.9
Mitral stenosis
Mitral stenosis (MS) is uncommon in industrialised countries where the population prevalence is 0.1%–0.3% (table 1) although rheumatic and calcific MS were reported in 10% of a hospital-based series.30 MS is more common in industrially underdeveloped countries with a population prevalence of rheumatic disease of up to 0.8%.31
There is little evidence for the effect of MS on non-cardiac surgery but in pregnancy the maternal mortality in Senegal32 for medically managed decompensated MS is 47% compared with 21% for AR and 0% for replacement heart valves. By contrast in industrialised countries with the availability of balloon valvotomy the maternal mortality from moderate and severe MS is close to zero.33 Morbidity is related to functional class before pregnancy.
The guideline consensus9 10 is that only severe MS with a resting pulmonary artery (PA) systolic pressure >50 mm Hg has a high risk of events during non-cardiac surgery, but there is no primary published evidence for this and assessment should include a careful evaluation of symptoms, exercise capacity and the response of transmitral gradients and estimated PA pressure to high heart rates. Transmitral gradients in moderate and severe MS are particularly flow sensitive so that tachycardia can quickly lead to pulmonary oedema especially in the presence of fluid loading at non-cardiac surgery. Patients with moderate and severe MS should therefore be exercised either informally around the couch or in an adjacent corridor if sedentary or frail or with a formal exercise test if feasible. A high risk of events in the normal natural history of MS is suggested by a mean gradient on exercise >15 mm Hg34 35 or PA systolic pressure >60 mm Hg and no better evidence exists to guide decisions before non-cardiac surgery (figure 7).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
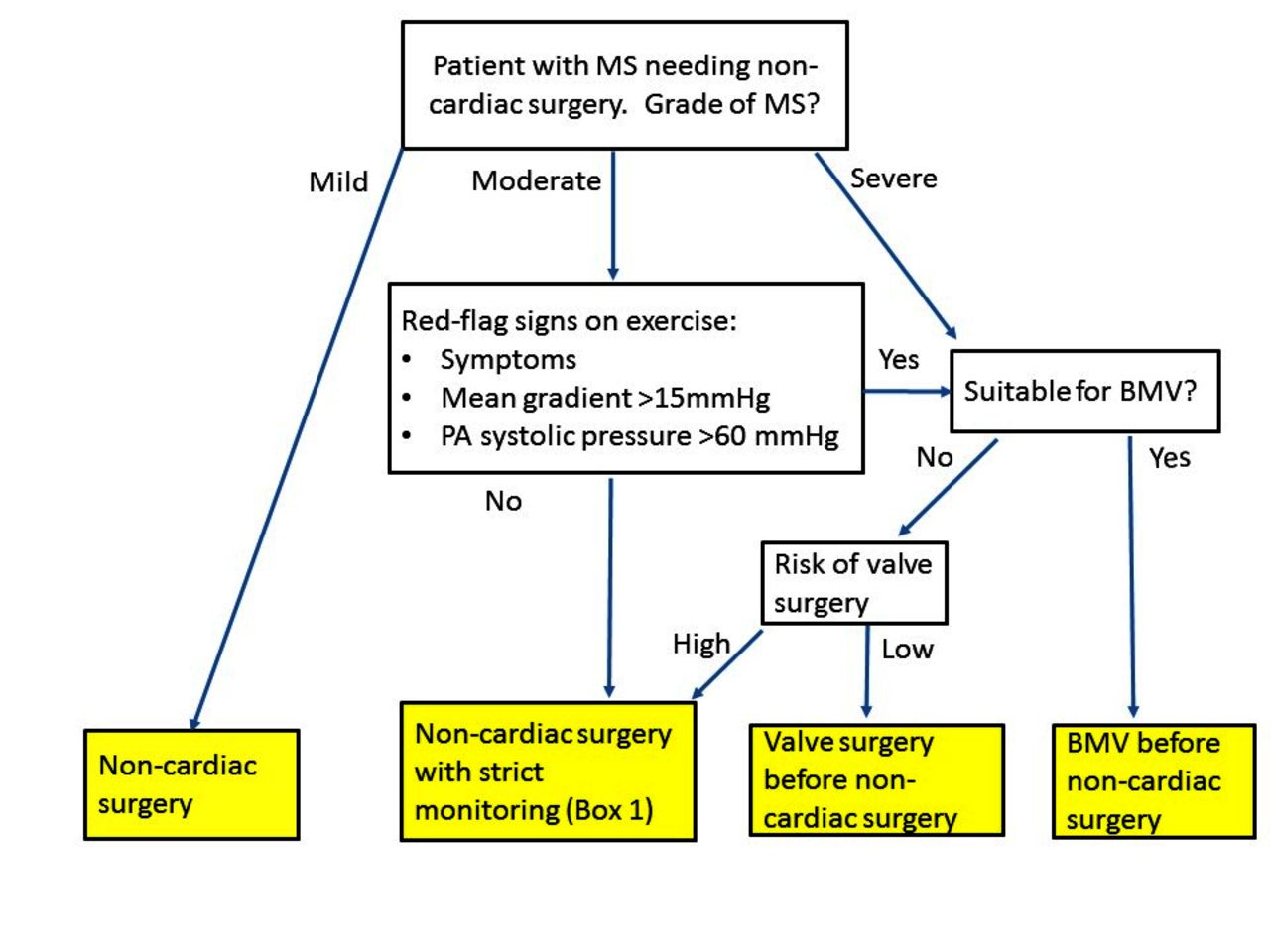
Flow chart for managing moderate and severe mitral stenosis (MS). BMV; balloon mitral valvotomy.
Low-risk non-cardiac surgery can be undertaken in an asymptomatic patient with any grade of MS and patients with mild MS can have any grade of non-cardiac surgery. However, balloon valvotomy should be considered for patients with spontaneous symptoms or those with asymptomatic severe MS or with moderate MS with a mean gradient >15 mm Hg on exercise. If balloon valvotomy is not feasible and either mitral valve replacement is high risk or the non-cardiac surgery is urgent this could be done with scrupulous heart rate control with beta blockers and with diuretics.
Right-sided valve disease
Significant pulmonary valve disease is usually seen as part of more general congenital heart disease and isolated valve disease is not common. The OxVALVE study3 found no pulmonary stenosis and a prevalence of significant pulmonary regurgitation of only 0.3%. No pulmonary valve disease was reported in a large US population.1 There is little information to guide practice but, as for left-sided disease, the expectation is that non-cardiac surgery should be safe if the patient is asymptomatic with good exercise capacity and preserved right ventricular (RV) function. If valve intervention is indicated anyway (eg, severe pulmonary regurgitation, pulmonary stenosis with V max >4.0 m/s)36 then this should be done before intermediate-risk or high-risk non-cardiac surgery.
TR is more common than pulmonary valve disease, seen in 2.7% in the OxVALVE study.3 It is an independent marker of a poor outcome late after surgery for left-sided disease37 as well as in pregnancy32 and it increases the risk of non-cardiac surgery in patients with severe AS.5 Cardiac surgical risk in the presence of severe TR is affected more by RV function than the grade of TR or the PA pressure.38 This is likely to be true also for non-cardiac surgery but little information exists.
Multiple valve disease
Multiple valve disease is common. The OxVALVE community study3 found involvement of two or more valves, usually to a mild degree, in 39% of their population aged >65, but more severe disease occurred in 20% of the Euro Heart Valve hospital-based survey.30 Often there is one dominant valve lesion to dictate the management strategy as discussed in the sections above. However, there may be haemodynamically significant disease of both left-sided valves typically severe AS with moderate or severe MR. In retrospective analyses the risk in patients with severe AS is increased by coexistent significant MR or TR.5 Furthermore if both left-sided valve lesions are moderate, there is the danger of underestimating their combined haemodynamic effect. This may be compounded if there is additional TR with or without RV dysfunction. Little information exists but the general principle is assumed to apply that the risk of non-cardiac surgery is acceptable if the patient is asymptomatic with good exercise capacity and compensated LV and RV function.9
Replacement or repaired valves
Normally functioning valves with compensated left and RV do not pose an increased haemodynamic risk. Patients with significant patient-prosthesis mismatch should be managed with the precautions listed in box 1. Patients with structural degeneration of a biological valve should be managed as for native disease if a further procedure, for example, valve in valve TAVI is not clinically appropriate.
The main concern is the management of anticoagulation in patients with mechanical valves. For minimally invasive procedures (dental extractions, superficial biopsies or other superficial procedures where bleeding can be easily controlled) the International normalised ratio (INR) should be brought down to the minimum end of the range but warfarin should not be stopped.
For other types of surgery, the patient needs to be admitted for transfer to intravenous ultrafiltrated heparin stopping the infusion 4 hours before surgery then restarting it when the risk of bleeding is judged to be low.8 9 The European guidance10 acknowledges that, although off-label, low-molecular weight heparin is used two times per day with the dose adjusted by weight and renal function and anti-Xa levels checked aiming for a level 0.5–1.0 U/mL. However, this approach should not be recommended in place of intravenous heparin.
Antibiotic prophylaxis
European Society of Cardiology (ESC) guidance is that antibiotic prophylaxis should be given to patients with high-risk cardiac conditions having dental procedures at high risk of developing endocarditis.39 UK National Institute for Health and Care Excellence (NICE) guidance to avoid all antibiotic prophylaxis was considered but rejected by the latest ESC committee39 but a subsequent revision of NICE guidance40 allows that antibiotic prophylaxis, while still not routine, may be considered if clinically appropriate. The Montgomery ruling on consent41 means that dentists in the UK are required to inform any patient likely to be interested (ie, those with high-risk cardiac conditions having high-risk dental procedures) of these areas of difference and controversy including the risks of taking or not taking antibiotic prophylaxis.42 The patient should be allowed to make their own decision and the discussion and decision recorded in the patient’s notes.
The most numerous high-risk cardiac conditions are prior endocarditis, replacement valves (including those placed in conduits used for repair of congenital disease) and valve repairs incorporating prosthetic material such as an annuloplasty ring. Other native valve disease in the absence of prior endocarditis are at moderate risk and do not require antibiotic prophylaxis.39
The procedures at high risk of causing endocarditis are those dental procedures associated with breaching the gums: extractions, dental scaling, root canal work, gingival incisions. Prophylaxis with 2 g amoxicillin is recommended in ESC guidance39 although 3 g sachets are available and therefore used instead in UK practice. Clindamycin 600 mg should be used for patients with hypersensitive to penicillins. If gastrointestinal or genitourinary procedures are being performed in the context of infection antibiotics active against enterococci should be given. If superficial procedures associated with skin infection are being performed antibiotics should include cover for staphylococci and beta-haemolytic streptococci.
Conclusions
Heart valve disease is widely recognised as a ‘Cinderella’ subject43 since it is common, but is often cared for by physicians who lack valve competencies.6 There is a recognition that specialist heart valve clinics are now the best-practice setting for care7 44 45 but these are not universal.46 It may be appropriate to refer patients with valve disease to a Heart Valve Centre45 for high-risk non-cardiac surgery.
There is insufficient evidence to guide practice. There were only 5 (3%) recommendations out of a total of 164 based on level A evidence in the 2017 ESC guidance on valve disease10 compared with 88 (35%) of 252 in the 2017 ESC guidelines on ST-elevation myocardial infarction.47
Preoperative assessment is increasingly performed to protocol by nurses and in general there is a lack of clinical experience in interpreting auscultation. Since murmurs are common in preoperative patients who may be anxious this tends to lead to excessive demand on echocardiography services which cannot easily be met. Ways to overcome this could include the use of artificial intelligence which appears capable of assessing murmurs, but more immediately by the use of point-of-care scans as an extension of the clinical examination to triage the need for standard echocardiogram.48
Key messages
Management protocols depend on the type of non-cardiac surgery, the Revised Cardiac Index Risk score, the grade of valve disease, the presence of symptoms and the functional capacity of the patient; however, decisions often have to be finalised individually to acknowledge the urgency or necessity of the non-cardiac surgery, the presence of comorbidities affecting the risk of valve procedures and the views of the patient.
Adverse events at non-cardiac surgery result from associated coronary disease as well as the haemodynamic effects of the valve disease and investigation for coronary disease should be considered in patients with poor or unknown exercise capacity with Revised Cardiac Risk Index score≥2 having high-risk non-cardiac surgery.
Symptomatic severe valve disease usually needs surgery in its own right before non-cardiac surgery.
Asymptomatic severe aortic stenosis should be considered for valve intervention before high-risk non-cardiac surgery unless the additive risk from that intervention is unwarranted (eg, as a result of comorbidities).
Asymptomatic severe mitral stenosis (MS) and moderate MS (with a mean gradient >15 mm Hg after exercise) should have consideration of balloon valvotomy before intermediate-risk and high-risk non-cardiac surgery.
Asymptomatic severe aortic regurgitation and mitral regurgitation with compensated left ventricular function tolerate all non-cardiac surgery without the need for valve intervention.
Imaging and assessment, opinions and care should be provided by sonographers, cardiologists, nurses and anaesthetists with recognised competencies in heart valve disease.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Acknowledgments
The author thanks Dr Madhusudan Puchakayala, cardiac anaesthetist, for his critical appraisal and suggestions.
References
Footnotes
Contributors JC is the sole author.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; externally peer reviewed.