Article Text

Statistics from Altmetric.com
- aortic and arterial disease
- cardiac risk factors and prevention
- coronary artery disease
- translational cardiovascular science
Learning objectives
Noninvasive assessments of peripheral arterial function and their relevance to cardiovascular disease and their role in risk stratification.
Principles of arterial stiffness and endothelial function measurements.
Applications in some epidemiological and interventional studies to date.
Introduction
Cardiovascular (CV) disease remains the leading cause of deaths worldwide, accounting for 32% of global deaths.1 CV mortality reduction is a key focus of the United Nations Healthy Strategy2 but in order to achieve this, there is a need to improve risk stratification.3 4 Nearly half of all CV deaths are attributable to coronary artery disease (CAD).1 Current risk stratification for suspected CAD uses a pretest probability (PTP) based on the nature of chest pain, gender and age to decide on the subsequent intervention. In those with low PTP for CAD, the Framingham Risk Score (FRS)5 discriminates the risk of CV events well for subsequent primary prevention.6 Individuals with a high PTP can reach a diagnosis of CAD and proceed to optimal medical therapy or invasive coronary angiography depending on symptom severity.5 There is a large group of individuals with intermediate PTP who proceed to further investigations with coronary imaging or stress testing5; however, a positive stress test only identifies less than half7 8 while coronary imaging defines less than a third of those who subsequently develop a CV event.5 7 Therefore, risk stratification with additional assessments may be beneficial. Measures of arterial stiffness and endothelial function provide global measures of arterial health. In this review, we focus on arterial stiffness measured by pulse wave velocity (PWV), arterial wave reflections by augmentation index (AIx) and endothelial function measured by either flow-mediated dilatation (FMD), forearm blood flow or digital reactive hyperaemia.
Arterial stiffness and wave reflections
Pulse wave velocity
The aorta is the principal elastic artery which distends circumferentially during cardiac systole to reduce the pressure generated and recoils in diastole to maintain the perfusion pressure within the arterial system for continuous exchange of nutrients and metabolic waste at a tissue level. This Windkessel effect of the aorta also reduces pressure variation between consecutive cardiac cycles to protect end-organs from pressure damage. Aortic PWV is considered the ‘gold standard’ measurement for arterial stiffness.9 The higher the PWV, that is, the higher the speed of the forward travelling pressure wave and the stiffer the aorta. Aortic stiffening leads to an increase in systolic blood pressure (BP) and a fall in diastolic BP, therefore widening the pulse pressure. This increases the left ventricular afterload and oxygen demand while decreasing coronary blood flow. Increased pulse pressure also increases the risk of stroke and damages capillaries, potentially leading to organ damage.
Description of technique
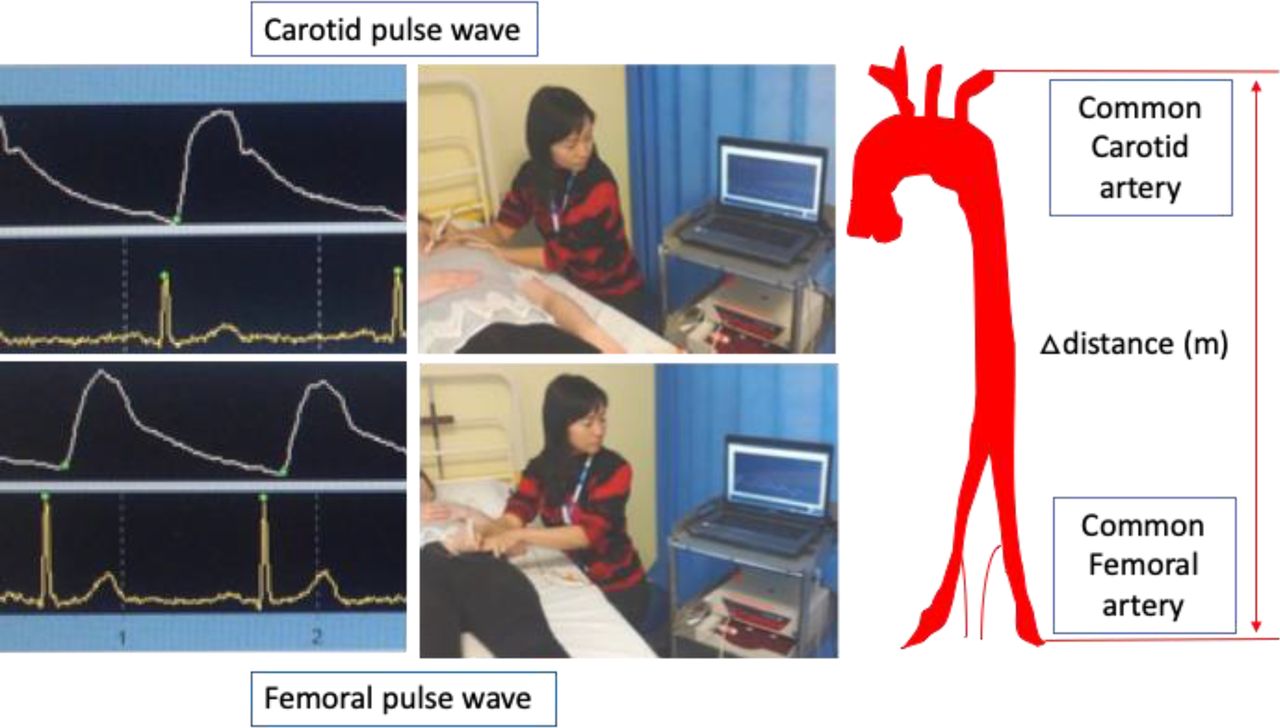
PWV is a measure of regional arterial stiffness and can be simply calculated by measuring the time taken for a pressure wave to travel through a known length of the artery. Carotid-femoral PWV (interchangeably known as aortic PWV), which is the direct measure of arterial stiffness, measures the speed of the pulse wave to travel from the common carotid artery to the ipsilateral common femoral artery.9 The anatomical landmarks for the carotid-femoral PWV are easily defined without any major difficulties in most subjects (figure 1). The distance can be derived simply from surface distance, measured using a ruler, tape measure or metal calliper (the latter accommodates central obesity), although the site of measurement should be standardised. The transit time for the ‘foot’ of the pulse wave, defined as the end of diastole, can be measured using a number of devices.10 There is no consensus for the most valid device, although standardisation of arterial stiffness measurements should be adhered to.9 All measurements of PWV should be analysed statistically correcting for mean arterial pressure (MAP) and heart rate. MAP is the vessel distending pressure, which exerts a positive and a nonlinear effect on the PWV11while heart rate exerts a positive effect at a higher MAP.12

Pulse wave velocity using the Sphygmocor applanation tonometry system. Waveforms are obtained from the carotid and femoral sites independently in quick succession.
Evidence of use from cross-sectional and epidemiological studies
Previously, an absolute aortic PWV threshold of 12 m/s was used to predict CV events, but this has since been revised to 10 m/s.13 It is important to recognise, however, that a single threshold is best avoided given age-related changes in PWV. Instead, multiple readings should be undertaken and two values within 1 m/s are more likely to represent the true value. High aortic PWV has been shown, in two meta-analyses, to be associated with increased risk of CV events,14 15 independent of conventional risk factors of the FRS,15 with the caveat of study heterogeneity.16 In longitudinal studies, aortic PWV predicted CV mortality in the general population and in subjects with hypertension, diabetes mellitus (DM), glucose intolerance and chronic kidney disease.17–24 Nonpharmacological interventions, such as moderate-to-high exercise levels reduced progression of PWV compared with a sedentary lifestyle.25 In a cross-sectional study, PWV also correlated with left ventricular hypertrophy.26
Use in interventional trials
Arterial stiffness is probably determined by a combination of dynamic and structural components. The former is represented, in part, by endothelium-derived vasoactive substances, including nitric oxide (NO), which acts on vascular smooth muscle cells (VSMCs) and ultimately influences vascular tone. The structural element is represented by extracellular matrix components which provide structural support in the arterial media.27 Failure to lower aortic PWV independently predicts CV mortality and may be associated with structural changes, such as arterial medial calcification seen in the general population, isolated systolic hypertension, end-stage renal disease and DM.28–30 Aortic PWV can be lowered with antihypertensive drugs, oral antidiabetic drugs, corticosteroids,31 cholesterol-lowering agents,32 as well as advanced glycation end-products cross-link breakers33 and endothelin-A receptor antagonists31 as well as weight loss34 through a number of mechanisms. Aortic PWV is well established as an intermediate end-point for fatal and nonfatal CV events.9
Clinical application
Several international guidelines recommend the addition of aortic PWV in the assessment of vascular end-organ damage as part of the management for hypertension.35 36 Other guidelines recognise aortic PWV as a useful biomarker to improve risk prediction for individuals close to decisional thresholds but does not yet recommend its use to improve risk assessment in the general population.37
Pressure wave reflection
The arterial pressure waveform is a composite measure of the forward travelling wave, resulting from cardiac systole, and the reflected waveform from bifurcation sites where arterial diameter changes. AIx provides information on wave reflection characteristics, in contrast to aortic PWV, which measures speed of forward travelling wave in the measured arterial segment.9 The greater the impedance, the greater the speed of the forward travel wave (as measured by aortic PWV) and the earlier the reflected wave superimposes on the forward wave. The amplitude of the augmented wave is expressed as a ratio to the pulse pressure (difference between systolic and diastolic pressures) as the AIx (figure 2). AIx is dependent on age, gender, height and heart rate, and these should be adjusted for in the analyses.38 AIx, corrected for a standard heart rate of 75 beats per minute, AIx@75, is a commonly used measure.39 AIx provides dynamic information on the load of the left ventricle and aorta and is influenced by endothelial function.40

Pulse wave analysis using the Sphygmocor applanation tonometry system. Radial waveforms are collected as well as peripheral blood pressure allowing the estimation of various central parameters derived from the arterial waveform.
Description of technique
The AIx should ideally be measured in the ascending aorta to accurately reflect the cardiac afterload. However, it is difficult to make direct noninvasive measurements of the aorta; therefore, a validated transfer function is used to derive the central waveform from a peripheral waveform, usually the radial or brachial artery.41 The most common method for measurement is using applanation tonometry where the AIx is calculated from the peripheral waveform for example, SphygmoCor (AtCor Medical, Sydney, Australia) (figure 2). This also provides other measures of wave reflection such as the reflection magnitude.42 It is vital to perform BP measurements prior to any measurement of AIx which is derived from the central pulse pressure, heart rate, augmentation pressure and BP. Oscillometric devices including the Vicorder (Skidmore Medical, Bristol, UK) and Arteriograph (Tensiomed, Budapest, Hungary) can also be used. Vicorder uses a cuff-based approach around the upper arm and fluid distension to derive the AIx from the brachial waveform using a transfer function akin to SphygmoCor. The two devices correlate significantly; however, Vicorder can underestimate arterial stiffness measures compared with SphygmoCor. The Arteriograph calculates the brachial AIx from the augmentation pressure and pulse pressure and has been validated against invasive methods.43
Evidence of use from cross-sectional and epidemiological studies
AIx is dependent on age, gender, height and heart rate44 and provides both dynamic and additional information to aortic PWV. In a meta-analysis of five longitudinal studies comprising 1326 subjects with established CV disease, an absolute increase in AIx by 10% increased the CV event risk by 31.8%, although there was significant study heterogeneity.45 Longitudinal studies suggest that progression of AIx with ‘normal’ ageing is not linear. Based on the Anglo-Cardiff Collaborative Trial, which examined the pattern of AIx of 4001 individuals from the general population, AIx showed prominent changes in those aged under 50 years, whereas aortic PWV showed prominent changes with age in those over 50 years.46 AIx is elevated in patients with atherosclerosis compared with health controls while aortic PWV remained within normal ranges and did not differ between the groups.47 Aortic wave reflections may offer an early indicator of atherosclerosis compared with PWV which may have prognostic value for CV events in patients with atherosclerosis. AIx and reflection magnitude42 are two such measures which have shown independent predictive ability for CV outcomes in large-scale studies. In other cross-sectional studies, AIx correlated with smoking status48 and inflammation.49
Evidence from interventional trials
A meta-analysis of 58 studies which included 3716 subjects showed overall reduction in AIx from baseline with a variety of antihypertensive treatments.50 In subgroup analyses, ACE inhibitor, angiotensin receptor blockers, calcium channel blockers, diuretics and renin–angiotensin system inhibitors significantly reduced AIx, whereas beta-blockers, alpha-blockers, nicorandil and moxonidine did not significantly reduce AIx.50 In the CAFE substudy of the ASCOT trial, comprising 2073 individuals, AIx showed a differential response favouring amlodipine-based treatment compared with beta-blocker-based treatments, despite similar improvements in peripheral BP.w51 Aortic PWV did not differ significantly between the groups.w51 Other interventional trials have shown an improvement in AIx with cholesterol-lowering agents,w52 oral antidiabetic drugs such as pioglitazonew53 and empagliflozin w54, and exercise intervention.w55
Clinical application
Pulse wave analysis has been recommended by expert consensus,9 along with arterial stiffness measurements for the evaluation of CV risk in patients. The widespread clinical use of pulse wave analysis is not apparent yet, but knowledge of central pressures may be used in addition to brachial readings to provide extra information for individual patients.w56 The SphygmoCor device provides other outputs and their interpretation that are provided in table 1.
Outputs from Sphygmocor and their interpretation
Endothelial function
The aorta branches into muscular arteries which further divides into resistance arteries and terminates in arterioles from which capillaries arise. In resistance arteries, vascular smooth muscle tone is regulated locally, predominantly in resistance arteries to further modulate organ blood flow.w57 Endothelial function refers to the functional vasodilatory response of the endothelium to NO. In the normal physiological state, the arterial endothelium is maintained in a vasodilatory, antithrombotic and anti-inflammatory state, predominantly driven by NO in response to laminar blood flow.w58 Different methods exist to measure endothelial function in arteries of different calibre, including FMD which measures conduit artery endothelial function, and the forearm blood flow responds to challenge agents, which measures resistance artery endothelial function. The latter is widely considered as the ‘gold standard’ measure. w59 Impaired coronary endothelial function, as detected by invasive coronary response to acetylcholine, is a sensitive marker of early atherosclerosis and predicts the development of treatable lesions and future CV events,w60, w61 but is largely impractical outside the cardiac catheter laboratory. Endothelial dysfunction is a systemic phenomenon and can be assessed when challenged with acetylcholine in peripheral arteries such as the brachial or resistance arteries.
Flow-mediated dilatation
Description of technique
FMD measures endothelium-dependent responses to reactive hyperaemia. The shear stress from the increased blood flow leads to the opening of calcium channels resulting in calcium influx. Intracellular calcium activates endothelial NO synthase, which converts L-arginine to NO in a two-step oxidation reaction. NO then diffuses through the endothelium and VSMCs and activates soluble guanylyl cyclase, which catalyses conversion of guanosine triphosphate to cyclic guanosine monophosphate, leading to a relaxation of VSMCs and hence vasodilatation.w56 The procedure is conducted in the supine position (figure 3). A baseline longitudinal image of the brachial artery is obtained using a high-frequency linear ultrasound probe held on a stereotactic probe holder. A sphygmomanometer cuff is placed 1–2 cm distal to the elbow crease and inflated to suprasystolic pressure for a standardised time. The continuous measurement captures baseline, occlusion and hyperaemic maximal arterial diameter following cuff release. After the diameter return to baseline, the process is repeated with sublingual glyceryl trinitrate tablet or spray, to test endothelium-independent function. Expert consensus guidelines aim to standardise the methodologyw62, w63 as a meta-analysis of 48 studies with 1537 individuals demonstrated that measurement error is independently and inversely correlated with adherence to methodology guidelines.w64

Flow mediated dilatation of the brachial artery.
Evidence of use from cross-sectional and epidemiological studies
In a meta-analysis of 35 studies including 17 280 participants, FMD independently predicted CV events in both unadjusted and adjusted analyses.w65 However, between-study heterogeneity and publication bias exist. The noninvasive nature of FMD means it can be applied at a population level, to provide a surrogate of endothelial function, which has been validated in population-based studies. Serial assessments are preferable to a single measure to improve risk stratification. Impaired FMD at 3 months following an acute coronary syndrome independently predicts cardiac death and a recurrent cardiac events.w66 However, there may be limitations to its applicability. In a meta-regression of 211 studies with 11 984 individuals, FMD correlated with incident CAD in the low-risk FRS group only.w67
Evidence from interventional trials
FMD improved following: exercise training,w68 statin therapy initiated early after an acute coronary syndrome,w69 L-arginine in hypercholesterolaemia subjects and in smokers,w70 and antiretroviral therapy.w71 However, in patients with diabetes, both L-argininew70 and enalaprilw72 failed to show improvement in FMD which would seem unusual. Novel agents such as dalcetrapib also failed to improve FMD in patients with CADw73 which later went on to demonstrate a lack of efficacy in terms of hard end-points. Therefore, noninvasive FMD can be used to assess CV outcomes in interventional trials for licensed and novel agents, although its application may be limited in patients with diabetes.
Clinical application
Expert consensus guidelines have been produced for the application of FMD; however, this currently remains a research tool.w62 FMD has the potential as a screening tool in the general population but has not yet been recommended in clinical guidelines as part of CV risk assessment.
Venous occlusion plethysmography
Description of technique
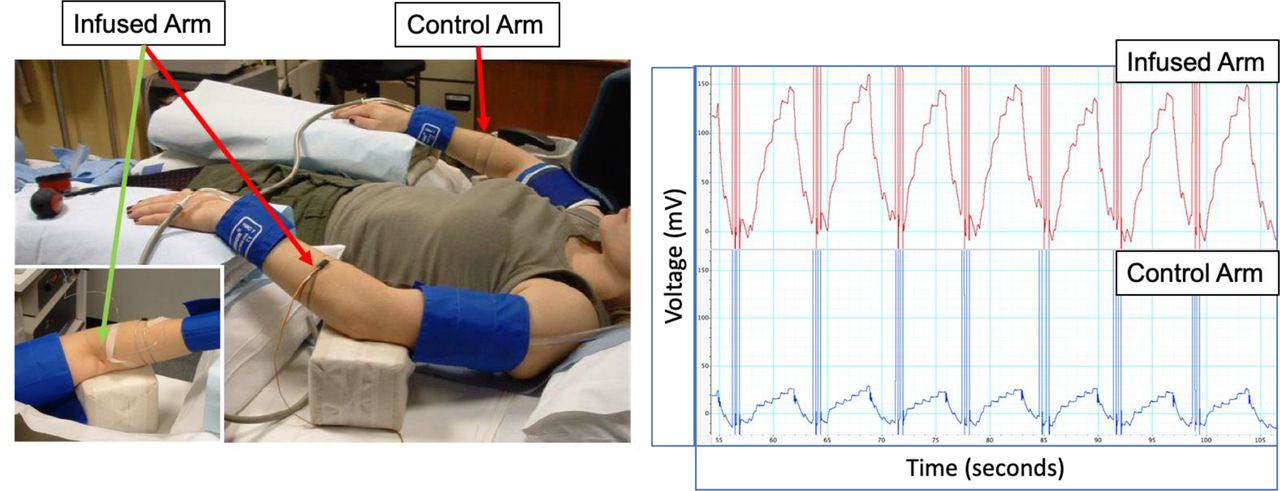
Forearm blood flow can be measured using a technique called forearm (or venous occlusion) plethysmography.w59 The principle of this technique relies on cuffs being intermittently inflated around the upper arms in order to allow arterial flow into the forearm but preventing the venous return. When the arterial inflow into the forearm is uninterrupted, the increase in volume is proportional to the arterial inflow until the venous pressure reaches occluding pressures.w74 Cuffs are inflated to suprasystolic pressures around each wrist to exclude the hands from the circulation. An intra-arterial needle delivers vasoactive substances to the ‘infused arm’ and elicits a forearm blood flow response with limited systemic effect, allowing the contralateral arm to serve as a ‘control arm’. It also allows for the definition of vasoactive properties of novel compounds to be defined in humans, akin to an in vivo organ bath experiment (figure 4).w59

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forearm blood flow using the venous occlusion plethysmography technique, allowing for infusions to be delivered via a fine 27G needle in the brachial artery.
Evidence of use from cross-sectional and epidemiological studies
Forearm plethysmography typically requires only a small number of subjects to detect differences due to its sensitivity. Therefore, it can readily be employed in studies to test pathophysiology and dissect underlying mechanisms which may be useful in the identification of novel targets for future interrogation.w75 Endothelial dysfunction as measured by impaired forearm blood flow responses to acetylcholine correlates well with the FRS,w76 hypertension,w77 hypercholesterolaemiaw78 and DM status,w79 and independently predicts CV events in the general population and in hypertensive individuals.w80, w81 Forearm blood flow was shown to be better than FMD or radial tonometry as a predictor of CV events in a large, prospective study comparing the three methods.w76, w81 In established CAD, endothelium-dependent and endothelium-independent functions were predictive of CV events.w82, w83 Recovery of endothelial function following acute coronary syndrome was associated with event-free survival, compared with those with persistently impaired endothelial function.w66
Evidence from interventional trials
Endothelial function using the forearm plethysmography technique has been used in a number of interventional studies of lipid-lowering agents,w78 anti-inflammatory drugs,w84 dietary products,w85 in the understanding of physiologyw86 and in the early development of novel therapiesw87 or experimental medicine studies to confirm target engagement, proof of mechanism/concept and in go/no go decisions in drug development.
Clinical application
Forearm plethysmography can be used to measure physiological vasoactive responses to novel agents and the effects of substances on endothelial function. In these situations, it is a semi-invasive technique, with the need for intra-arterial brachial artery cannulation (although only a 27-gauge needle); therefore, its use is limited to small mechanistic studies and within the early phase research setting in specialist centres.
Digital reactive hyperaemia
Digital reactive hyperaemia plethysmography attempts to mimic the same principles as that for forearm plethysmography and is thought to be driven predominantly by endothelium-dependent NO.w88 However, the results must be interpreted with caution since the hands contain rich arteriovenous connections and capillaries, and therefore may not directly elicit arterial function per se as defined earlier while distribution of orally administered vasoactive agents may also not be linear. The reactive hyperaemia may reflect forearm resistance artery function rather than of hand microvasculature alone and may differ from the more conventional measures of endothelial function.
Description of technique
A finger probe is placed on the index finger of the hand undergoing reactive hyperaemic index (RHI) testing, with the sensor placed against the pulp of the distal phalanx, with an upper arm cuff in the ipsilateral side to achieve arterial occlusion while venous occlusion is achieved with an intrinsic venous tourniquet in the finger probe. A separate sensor is placed on the contralateral index finger and acts as an internal, nonischaemic control.w89 The pressure changes in the fingers are filtered, amplified and displayed following a computerised automated algorithm which reduces intraobserver and interobserver variability. Pressure change in the finger pulp is recorded over a baseline, occlusion and hyperaemia period.w88 The RHI is the ratio of hyperaemic pulse wave amplitude over the recording period divided by baseline pulse wave amplitude over the same ratio in the control finger (not subjected to occlusion and hyperaemia). Glyceryl trinitrate is administered and the above steps repeated to test endothelium-independent function.w90, w91
Evidence of use from cross-sectional and epidemiological studies
In a meta-analysis of six studies with 1602 participants, log digital hyperaemia index correlated with the pooled adjusted risk ratio for CV events.w65 However, the meta-analysis only included studies with a CV disease cohort and comparable studies in both CV disease and non-CV disease cohorts have not been conducted to establish the predictive ability of digital reactive hyperaemia for CV events. In a cross-sectional study of 5000 individuals, RHI showed a reducing trend with age in men, but not in women, nor was there a trend with CV risk score quantiles (SCORE).w92 Some studies failed to show a reduction of digital reactive hyperaemia in conditions associated with endothelial dysfunction (DM and renal impairment) when compared with healthy controls, and failed to show a reduction in RHI following interventions known to cause acute endothelial dysfunction (smoking and acute glucose challenge in healthy volunteers).w93 The role of RHI, therefore, remains to be determined.
Evidence from interventional trials
RHI has been used to assess changes in microvascular function in small intervention studies as a surrogate for endothelial function, although most of these studies were conducted in Japan. RHI improved following exercise intervention in healthy women,w94 lenvatinib and growth hormone in patient groups with non-CVw95, w96, and statin therapyw97 and oral antidiabetic drugsw98, w99 in patients with established CAD and hypercholesterolaemia and DM, respectively.
Clinical application
This remains a research technique, further studies are required to validate its use, and determine what aspect of endothelial function RHI measures.
Emerging techniques in the assessment of endothelial function
Optical coherence tomography (OCT) of the retina and choroid is a novel, noninvasive technique of assessing arterial function.w100 Thinner choroid measurements were associated with markers of endothelial dysfunction and increased aortic stiffness, in a cross-sectional prospective study comparing 50 patients with chronic kidney disease, 50 with hypertension and 50 healthy controls.w101 However, the association between OCT measures and endothelial function as well as the relationships with clinical outcomes needs to be validated in future studies.
Conclusion
Assessments of endothelial dysfunction and arterial stiffness provide dynamic and early evidence of atherosclerosis and CV disease. This review provides an overview of how to conduct these tests, how to interpret the results, their use in a variety of observational and interventional studies and their limitations and applicability. Endothelial dysfunction is a systemic phenomenon and correlates well with coronary endothelial dysfunction and outcomes while arterial stiffness is independently predictive of CV mortality. There is scope for clinical use in risk stratification including FMD and PWV, although some assessments, such as forearm blood flow, remain experimental due to its specialist nature but is useful in clinical drug development to dissect mechanisms and provide proof-of-concept. Measures of arterial stiffness and endothelial function additionally provide short-term and intermediate endpoints for experimental trials investigating the potential effects of novel or existing therapies to modulate CV events.
Supplementary references are provided in online supplementary file.
Supplemental material
Key messages
Arterial stiffness and endothelial function provide global assessments of cardiovascular (CV) disease burden and provides at a functional level, early detection of organ damage, which can improve risk stratification in CV disease.
There are several methods of measuring arterial function which can be employed in cross-sectional and epidemiological studies as well as interventional trials.
The use of these methods of assessment in the clinical setting is beginning to be recognised in international guidelines while others remain experimental.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Acknowledgments
We would like to acknowledge Professor Ian Wilkinson, Dr Carmel McEniery and Dr Thomas Hiemstra who provided advice during the construct of the manuscript. We would also like to acknowledge Dr Kaisa M. Mäki-Petäjä who kindly donated pictures for the conduct of FMD and Forearm blood flow in figures 3 and 4, respectively, and contributed towards the construct of the manuscript.
References
Footnotes
Contributors All listed authors provide substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data, drafting the work or revising it critically for important intellectual content, provided final approval of the version published and an agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding ZS acknowledges funding support from the Experimental Medicine Training Initiative (RG81329), University of Cambridge. JC and ZS acknowledge funding support from the NIHR Cambridge Biomedical Research Centre, Cambridge University Hospitals NHS Foundation Trust.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Patient consent for publication Not required.