Article Text

Statistics from Altmetric.com
One of the most feared complications in atrial fibrillation (AF), an epidemic disease associated with increased comorbidities and subsequent mortality, is stroke and/or systemic embolism related to left atrial and especially left atrial appendage thrombus formation. Besides stroke and systemic emboli, heart failure and death are equally feared complications in this arrhythmia. AF is associated with left atrial structural remodelling (atrial fibrosis) and hypercoagulability status; both may cause and promote AF due to the atrial cardiomyopathy occurrence.1 Therefore, left atrial thrombus could be the result of this vicious circle associated with this thrombogenic cardiomyopathy.1
Nowadays it is well known that thromboembolic risk scores (CHA2DS2-VASc - C: congestive heart failure; H: hypertension; A: age 75 years or older; D: diabetes mellitus; S: stroke, transient ischemic attack, or systemic throboembolism (including any history of cerebral ischemia); V: prior myocardial infarction, peripheral arterial disease, or aortic plaque; A: age 65 to 74 years; Sc: sex category (female); and CHADS2 - C: congestive heart failure; H: hypertension; A: age 75 years or older; D: diabetes mellitus; S: stroke, transient ischemic attack or systemic thromboembolism (including any history of cerebral ischemia) recommended by the guidelines have a suboptimal predictive accuracy in patients with AF before anticoagulation treatment. Moreover, transoesophageal echocardiography seems to be indicated in patients with non-paroxysmal AF (persistent, long-lasting persistent and/or permanent) and high thromboembolic risk, as assessed by both scores, despite having received correct anticoagulation therapy. An ideal thromboembolic risk assessment tool allowing clinicians accurate patient selection and appropriate risk stratification has yet to be created.
Since its first incorporation in the 2010 guidelines, CHA2DS2-VASc has been recommended in non-valvular AF irrespective of AF type (paroxysmal vs non-paroxysmal AF). The paper by Kapłon-Cieślicka et al entitled: ‘Atrial fibrillation type and renal dysfunction as important predictors of left atrial thrombus’ might open a new door in thromboembolic risk assessment and stratification in patients with AF.2 The authors proposed a new risk score, CHA2DS2-VASc-RAF (C: congestive heart failure; H: hypertension; A: age 75 years or older; D: diabetes mellitus; S: stroke, transient ischemic attack or systemic thromboembolism (including any history of cerebral ischemia); V: prior myocardial infarction, peripheral arterial disease, or aortic plaque; A: age 65 to 74 years; Sc: sex category (female); R: renal dysfunction; AF: atrial fibrillation type - paroxysmal or non-paroxysmal), to predict left atrial appendage thrombus, which includes two new parameters: AF type and renal dysfunction (defined as glomerular filtration rate (GFR) <57 mL/min/1.73 m2). Both parameters seem to significantly improve CHA2DS2VASc’s thromboembolic risk stratification and prognostic value in AF.
In the current guidelines, AF type is not considered a criterion for a higher thromboembolic risk. There are many studies in the literature which have found no difference in outcomes between paroxysmal versus non-paroxysmal patients with AF in terms of thromboembolic risk.3 A careful critical analysis of these studies revealed the following reasons for a negative result: anticoagulation was either not uniform by design or inconsistent; there were imbalances of the randomisation scheme between paroxysmal and non-paroxysmal patients with AF; there were significant differences in the use of oral anticoagulation rates across AF types; lower thromboembolic risk or more heterogeneous populations. In addition, chronic kidney disease is known to be strongly associated with other components of the CHA2DS2-VASc risk model such as heart failure, hypertension or diabetes. However, a large randomised trial, ROCKET-AF, comparing patients with paroxysmal versus persistent AF revealed a higher risk of death and stroke for the latter.3 In addition, rates of stroke or systemic embolism in both types of AF did not differ by treatment assignment and rates of major bleeding were similar. Similarly, in a recently published meta-analysis, which included 176 975 patient-years in the non-paroxysmal AF group and 62 553 patient-years in the paroxysmal AF group from 18 studies, non-paroxysmal AF was associated with a higher risk of overall thromboembolic events compared with paroxysmal AF and major bleeding rates did not differ among groups.4 AF type as a new parameter introduced by Kapłon-Cieślicka et al 2 in thromboembolic risks prediction might be an important contribution to current risk stratification in these patients. In this new score, CHA2DS2-VASc-RAF, persistent AF has 4 points and is less powerful than permanent and long-lasting persistent AF, which have 10 points. Therefore, the authors underlined that ‘patients with non-paroxysmal AF and a CHA2DS2-VASc score of 0 or 1 point should not automatically be attributed to the low thromboembolic risk and disqualified from anticoagulant treatment’.2
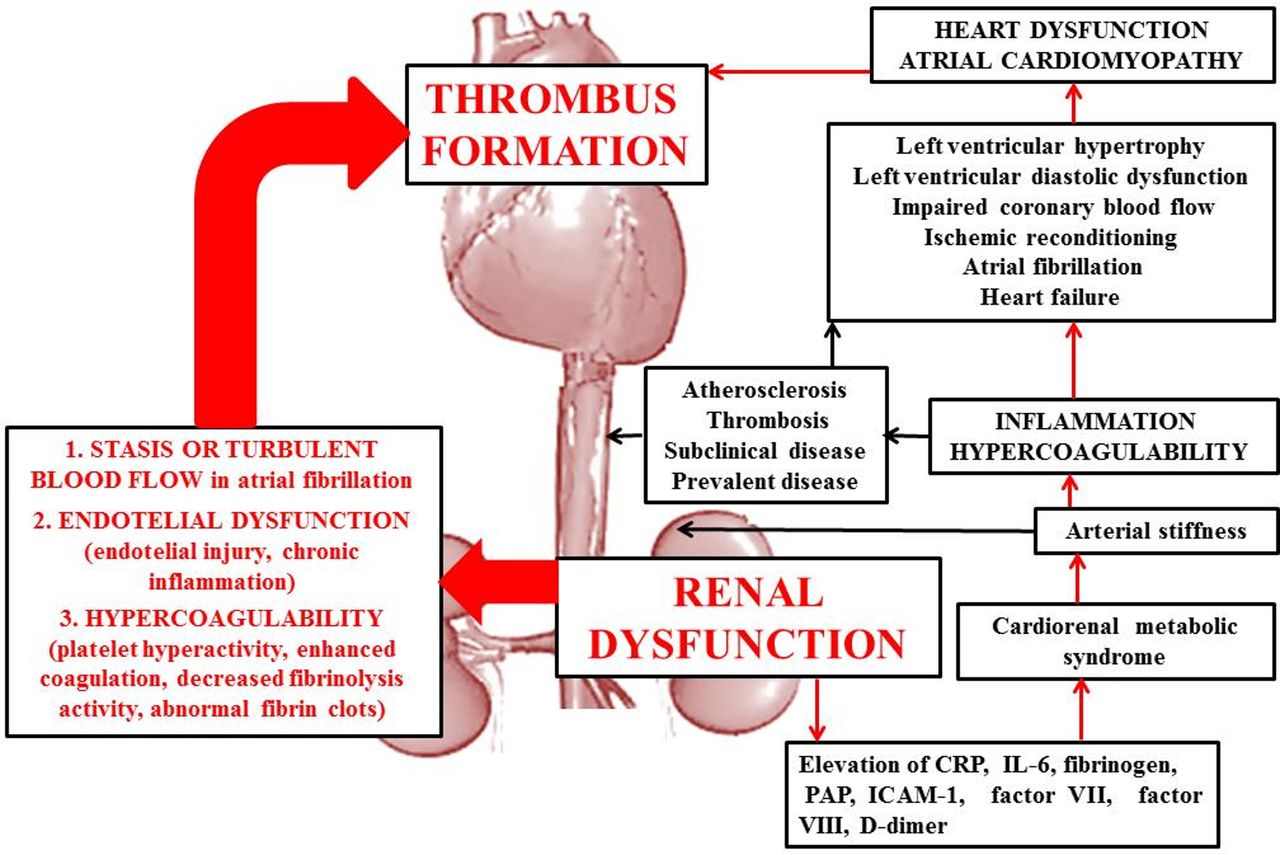
Renal dysfunction as a predictor of thromboembolic risk in AF was not recognised in clinical practice, so far. It seems that relative risk of stroke increases with declining GFR (an average 7% with every 10 mL/min/1.73 m2) and increasing albumin–creatinine ratio (an average 10% with every 25 mg/mmol).5 The impaired renal function could contribute to increased risk of stroke via procoagulant and inflammatory pathways and changes in arterial compliance/stiffness. In renal dysfunction, there are increased levels of inflammatory and procoagulant biomarkers, including C reactive protein, interleukin-6, fibrinogen, plasmin-antiplasmin complex, factor VII, factor VIII and D-dimer. These biomarkers will induce inflammation and hypercoagulability which seem to be present early in renal disease and could promote atherosclerosis and thrombosis.6 In cardiorenal metabolic syndrome, structural and functional changes of the vascular wall will promote arterial stiffness.6 The possible interactions between renal dysfunction, atrial cardiomyopathy and heart dysfunction via procoagulant and inflammatory pathways, atherosclerosis, thrombosis and arterial stiffness are presented in figure 1.

{kind=link}
The interactions between renal dysfunction and thrombus formation pathways through heart dysfunction and atrial cardiomyopathy. CRP, C reactive protein; ICAM-1, intercellular adhesion molecule-1; IL-6, interleukin 6; PAP, plasmin-antiplasmin complex.
Despite the well-known association between renal dysfunction and thromboembolism and its role in AF-related strokes, it has not been yet included in CHA2DS2-VASc. The acronyms ‘c’ was initially intended to stand for creatinine clearance <30 mL/L or proteinuria, but at the time there were insufficient evidence for renal dysfunction to become a parameter of the risk score. Later was proposed R2CHADS2 score (R: renal dysfunction; C: congestive heart failure; H: hypertension; A: age 75 years or older; D: diabetes mellitus; S: stroke, transient ischemic attack or systemic thromboembolism (including any history of cerebral ischemia), in which renal impairment was defined as a creatinine clearance <60 mL/min/1.73 m2 using the Cockcroft-Gault formula3; it has been assigned 2 points—powerful equivalent to that of previous stroke or a transient ischaemic attack in the CHADS2 or CHA2DS2-VASc score. It ranges between 0 and 8. Renal impairment was also included in another thromboembolic risk score, ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation), with 1 point for proteinuria, and eGFR <45 mL/min or end-stage renal diseases.7 ATRIA score ranges between 0 and 12 for those without a prior stroke and 7 and 15 for those with a prior stroke. However, neither R2CHADS2 nor ATRIA has been imposed into clinical practice. In addition, these risk scores which were developed to predict left atrial thrombus formation called for validation in larger cohorts to confirm their predictive power of the stroke.
According to the following scores, renal dysfunction could also increase the haemorrhagic risk in patients with AF in addition to the thromboembolic risk: HASBLED in which dialysis, transplant, creatinine >2.26 mg/dL or >200 µmol/L have 1 point; ATRIA in which eGFR <30 mL/min or dialysis-dependent has 1 point; ORBIT with 1 point for eGFR <60 mL/min, HEMORR2HAGES with 1 point for renal disease; SAMe-TT2R2 with 1 point for renal disease. Only the first one is recommended by current guidelines, being used in the haemorrhagic risk assessment in patients with AF under anticoagulation treatment. In end-stage renal disease, the threshold for anticoagulation therapy to prevent ischaemic stroke should probably be higher than in the general population because of different risk–benefit ratio. Therefore, in patients with high bleeding risk and chronic kidney disease, physicians should not withhold anticoagulation therapy or use a subtherapeutic intensity of anticoagulation, because they also have an increased risk of thromboembolism.
In the new risk score, CHA2DS2-VASc-RAF, renal dysfunction was defined as GFR <56 mL/min/1.73 m2 and has 2 points (similarly with stroke or age >75 years). Beyond potentially improved risk stratification, there are other possible practical implementations of renal dysfunction as a predictor of thromboembolic risk through CHA2DS2-VASc-RAF. It is well known that the use of non-vitamin K antagonists is restricted in patients with impaired renal function. Lower doses of non-vitamin K antagonists are recommended in patients with only moderate renal impairment and AF. In those with severe renal dysfunction or hemodialysis, treatment with vitamin K antagonists remains the better option. Another debate related to renal dysfunction as a predictor of thromboembolic risk could be which GFR formula should be used for risk stratification in non-valvular patients with AF. Renal dysfunction frequently defined as GFR <60 mL/min/1.73 m2 could be assessed by the Cockcroft-Gault formula, MDRD (Modification of Diet in Renal Disease) or CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) equation. The MDRD equation underestimates GFR and the Cockcroft-Gault formula overestimates GFR at >60 mL/min/1.73 m2 in healthy individuals, and both equations overestimate GFR at >60 mL/min/1.73 m2 in people with reduced muscle mass (who are more likely to be unwell and may be at higher risk of stroke).8 However, it seems that the Cockcroft-Gault formula might be more appropriately in classifying individuals with respect to the risk of ischaemic cerebrovascular.8 Although the new score, CHA2DS2-VASc-RAF, makes more complex thromboembolic risk stratification, this added complexity may be counterbalanced by the widespread availability of electronic devices.
In conclusion, AF type and renal dysfunction are new challenges in thromboembolic risk assessment. Both are related to the fundamental characteristic of the structural pathology associated with AF which is fibrosis.1 This pathogenic process will induce atrial cardiomyopathy, ‘a specific, primary form of biatrial pathology, characterised by extensive fibrosis as the substrate underlying atrial arrhythmias and thromboembolism’.1 Probably it is time to explore more about this new entity named atrial cardiomyopathy in each patient with AF.
Footnotes
MF and DMT contributed equally.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.
Patient consent for publication Not required.
Linked Articles
- Cardiac risk factors and prevention