Article Text

Statistics from Altmetric.com
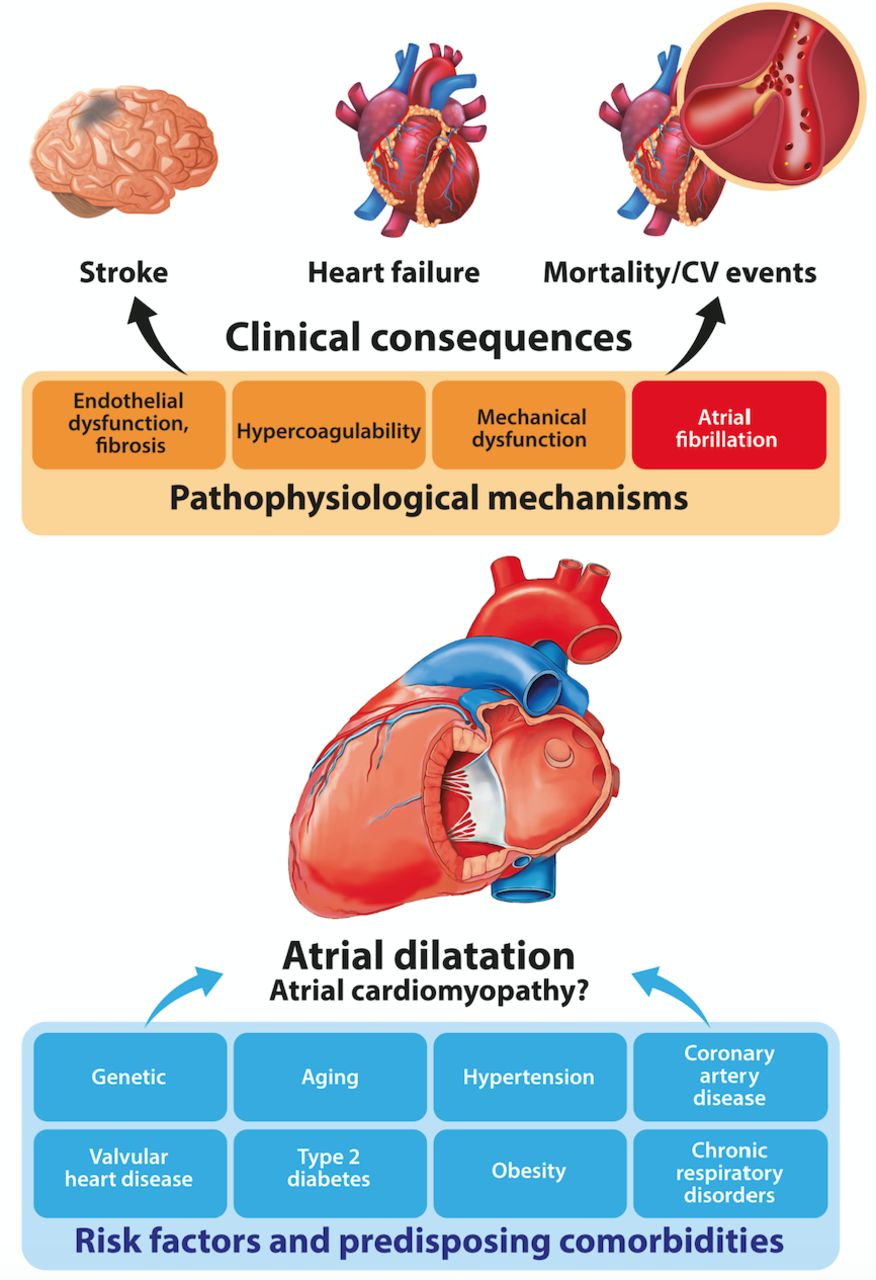
The left atrium (LA) plays an important role in cardiovascular homeostasis through the modulation of cardiac filling and output, as well as the regulation of circulatory volume and tone. LA remodelling is characterised by dynamic alterations in atrial structure, function and electrophysiology. Most frequently, it occurs in association with ageing, hypertension, ischaemia, metabolic and pulmonary disorders (central illustration, figure 1). LA dilatation, the hallmark of atrial remodelling, has been increasingly recognised as a prognostic biomarker of thromboembolic and cardiovascular events, in particular in patients with atrial fibrillation (AF). However, cardiovascular risk attributable to atrial dilatation also appears to be increased in individuals without AF and is incompletely explained by the associated comorbidities and risk factors. The clarification of this issue was attempted by putting forward the concept of atrial cardiomyopathy, as a primary form of atrial abnormality, in which atrial fibrosis, hypercoagulability, contractile and endothelial dysfunction may lead to incident AF, heart failure (HF) and thromboembolism, independent of other causes (central illustration, figure 1).1 However, evidence from human studies supporting this concept is inconclusive. Also, a comparison of cardiovascular risk associated with LA dilatation in patients with and without AF has not been systematically conducted.

{kind=link}
Central illustration: Risk factors and clinical consequences of left atrial dilatation
The study by Froehlich et al,2 published in Heart, provides a new insight into this important subject. This study presents a systematic review and a meta-analysis of 91 observational studies exploring the association between several indices of LA dilatation and outcomes in patients with AF (23 studies with a total of 14 936 participants) and those without AF (68 studies with a total of 50 720 patients). The studies included in the meta-analysis integrated data on a wide array of background cardiovascular pathology, including hypertension, ischaemic heart disease, HF and diabetes. The primary outcome was stroke or systemic thromboembolism. Secondary outcomes comprised incident HF, all-cause mortality and the composite of major adverse cardiovascular events (MACEs). Only longitudinal studies with more than 100 participants were considered. LA dilatation was assessed through four echocardiographic indices, including antero-posterior LA diameter and LA diameter indexed to body surface area (LADI), LA volume and LA volume indexed to body surface area (LAVI). The meta-analysis demonstrated that LA dilatation, in general, was associated with a higher risk of adverse outcomes independently of other clinical characteristics and regardless of AF. Of note, the strength of association was stronger in individuals without AF for most outcomes, including stroke, all-cause mortality and incident HF. None of the analysed indices of LA dilatation appeared predictive of stroke or all-cause mortality in patients with AF. Conversely, LA diameter and LADI, but not LA volume or LAVI, were associated with thromboembolism in the absence of AF. LA diameter was associated with incident HF in patients with AF, whereas LA volume and LAVI predicted incident HF only in individuals without AF. Most parameters of LA dilatation were independently associated with MACE regardless of AF.
The study merits appraisal for an accurate methodology, detailed literature research, sufficient data extraction, meticulous statistical analyses and quality assessment. However, several limitations deserve a comment as they pertain to the clinical utility of the results. The meta-analysis has shown a considerable heterogeneity in the prognostic power of the analysed indices of LA dilatation. This suggests a dissimilarity between the included studies; hence, a caution is warranted with regards to the interpretation and generalisation of the results. The lack of association between LA dilatation and the risk stroke and all-cause mortality in AF patients may be explained by a considerable use of oral anticoagulant therapy among patients with AF in the current meta-analysis. Both vitamin K antagonists and direct oral anticoagulants are highly effective in reducing the risk of stroke and all-cause mortality in AF. This effect might have attenuated the risks related to LA dilatation. Indeed, analysis of the placebo arms in earlier trials of vitamin K antagonists for stroke prevention in AF have shown a strong association of LA dilatation with the risk of thromboembolism. Furthermore, compared with individuals in sinus rhythm, patients with AF often demonstrate more advanced endothelial damage in the LA and reduced nitric oxide bioavailability as a consequence of endothelial dysfunction in both the LA and systemic circulation.3 These abnormalities may add to the prothrombotic state characteristic of AF but are often disproportionate to the extent of LA dilatation.3 Therefore, this effect could have confounded the association between LA dilatation and thromboembolic risk in AF. By contrast, increased LA diameter was associated with a higher risk of stroke and mortality in non-AF population, which may relate to a greater propensity for intercurrent development of AF that could not have been accounted for in the present meta-analysis. This association may also suggest the presence of an intrinsic thrombogenic substrate due to atrial cardiomyopathy; however, this concept requires further confirmation. Inclusion of echocardiographic quantification of LA dysfunction (eg, LA function index, LA strain and strain rate), in addition to the measures of LA dilatation, could refine the assessment of the underlying substrate in the LA. Recently, LA strain and strain rate have been found to inversely correlate with the extent of atrial fibrosis on cardiac magnetic resonance, independent of other echocardiographic parameters or cardiac rhythm during the assessment.4
The present study has shown a lack of association between LA volume or LAVI with subsequent thromboembolic events, despite the fact that LA volume has been acknowledged as a more accurate predictor of adverse outcomes (including stroke) compared with other indices of LA size and regardless of AF.5 This may be explained by the predominant use of two-dimensional echocardiography for the assessment of LA volume in the studies included in the present meta-analysis. Two-dimensional echocardiography is limited by geometric assumptions about LA shape and foreshortening of the LA cavity that may lead to an underestimation of the true LA volume as compared with more precise imaging techniques such as three-dimensional echocardiography, CT or cardiac magnetic resonance. The accurate assessment of LA volume may be further hampered by the loss of atrial contractility in AF. In addition, recent evidence indicates that minimum LA volume (rather than maximum LA volume) better reflects LA functional impairment (ie, hypocontractility) due to prolonged exposure to increased left ventricular filling pressure.6 Minimum LA volume also has a stronger prognostic significance for adverse outcomes.6 The present study does not differentiate between these indices, which could have limited the predictive value of LA volume for subsequent thromboembolic complications.
Dilatation of the LA is often viewed as a consequence of long-standing elevated filling pressure in the setting of left ventricular dysfunction, preceding the onset of overt HF. Thus, LA dilatation appears to be a biomarker of left ventricular dysfunction, rather than a determinant of the future development of HF. This concept is challenged by the study by Froehlich et al,2 suggesting an independent prognostic significance of LA dilatation for incident HF in patients with or without AF and a wide variety of associated cardiovascular disorders. In support of this observation, a recent study demonstrated that LAVI was an independent predictor of adverse cardiovascular outcomes, including HF, following first myocardial infarction.7 In addition, impaired LA function, even without apparent LA dilatation, has been shown to predict HF events.8
Furthermore, impaired LA function, as assessed by LA reservoir strain, has been correlated with LA dilatation and associated with a higher risk of MACE comprising cardiovascular and sudden cardiac death and HF hospitalisation, in patients with HF and preserved ejection fraction.9 This observation is corroborated and further extended by the present meta-analysis, suggesting that LA dilatation could be a harbinger of a greater risk of MACE in patients with various underlying cardiovascular pathology, with or without AF. Given that AF confers an intrinsic risk of MACE, even in the absence of overt coronary artery disease,10 these results merit further consideration for strategies tailored to refine cardiovascular risk stratification.
In conclusion, the present meta-analysis emphasises the significance of LA dilatation as a prognostic biomarker for several important clinical outcomes, including stroke, incident HF and mortality in patients with and without AF. Whether the risk attributable to LA dilatation could be truly separated from the cumulative impact of left ventricular dysfunction and other risk factors remains uncertain. Hence, the proof of concept of the presumed atrial cardiomyopathy is still missing. A more comprehensive evaluation of both functional and structural LA remodelling, with a combination of different imaging modalities, may be needed to better characterise atrial cardiomyopathy and its intrinsic prognostic implications.
Footnotes
Contributors All the coauthors have participated in the drafting, writing and final revision of the editorial.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.