Article Text

Statistics from Altmetric.com
Learning objectives
To outline the causes and epidemiology of non-infective endocarditis.
To explore the pathophysiology of non-infective endocarditis.
To discuss the appropriate investigation of patients with suspected non-infective endocarditis.
To highlight the key principles of management of non-infective endocarditis and when surgical intervention should be considered.
Introduction
Endocarditis is defined as inflammation of the endocardium, the lining of the cardiac chambers and valves, and characterised by vegetations, most commonly caused by infection with bacteria or fungi. Non-infective endocarditis, also known as non-bacterial thrombotic endocarditis (NBTE) or aseptic endocarditis, refers to a rare condition characterised by formation of sterile vegetations. Without treatment, these can lead to valve dysfunction, heart failure, systemic embolism and death. Herein, we review the pathophysiology, clinical features, diagnosis and treatment of NBTE.
Background
The first description of sterile vegetations on the heart valves was provided by Zeigler in 1888.1 Libman and Sacks then published a case series of four patients in 1924 which associated these atypical lesions with systemic lupus erythematosus (SLE).2 These vegetations are not associated with an inflammatory response or bacteraemia and commonly occur as a result of fibrin deposition and platelet aggregation. Sterile vegetations can develop in a number of conditions, including autoimmune disease, malignancy and hypercoagulable states. Although Libman–Sacks endocarditis refers specifically to NBTE seen in patients with the autoimmune disorders SLE and antiphospholipid syndrome (APLS), other interchangeable terminology for NBTE includes verrucous endocarditis and marantic endocarditis.
A vegetation is defined as an oscillating intra-cardiac mass on a valve (or its supporting structure) or implanted material. The rapid evolution of echocardiographic imaging techniques has resulted in higher rates of vegetation detection in more recent studies using these developed imaging modalities.3 4
Epidemiology
NBTE is a rare condition and most commonly diagnosed at post-mortem. The exact incidence is unknown but rates of up to 3.7% have been reported at autopsy.5 6 The incidence increases with age (likely due to the association with malignancy) with no known gender predominance.6 7 NBTE has a well-known association with autoimmune conditions and malignancy.6 7 In the largest study of culture-negative endocarditis, NBTE accounted for 2.5% of cases.8 Patients with definite endocarditis but no underlying autoimmune or malignant condition were more likely to have a positive serum rheumatoid factor compared with those with confirmed aetiology, highlighting the likely under-estimation of immune-mediated causes.
Echocardiographic studies have found vegetations in 11% of patients with SLE and no evidence of infection.9 Although uncommon, NBTE has been reported in rheumatoid arthritis.8 10 There are isolated case reports of NBTE associated with rarer autoimmune conditions, including granulomatosis with polyangiitis, Behçet’s disease and adult-onset Still‘s disease.11 12 Post-mortem studies have also identified NBTE in patients with HIV, although the incidence is lower than initially thought.13
NBTE is common in neoplastic conditions with one prospective study reporting a prevalence of 19% in patients with underlying malignancy (most frequently adenocarcinomas, particularly of the pancreas and lung).6 7 14–16
Coagulation abnormalities indicative of disseminated intravascular coagulation (DIC) have also been found in up to 50% of patients with NBTE, suggesting a strong relation with hypercoagulable states, including primary APLS, burns and sepsis.15–17
Table 1 summarises the conditions associated with NBTE and their reported prevalence. Ante-mortem diagnosis is rare and NBTE is therefore often underestimated. With improved imaging modalities, there is significant variability in the prevalence of NBTE reported in the literature. Patients often have a combination of conditions predisposing them to NBTE (such as malignancy and a hypercoagulable state).
Summary of conditions associated with non-bacterial thrombotic endocarditis and their reported prevalence
Pathophysiology
Deposition of sterile fibrin and platelets on the surface of valve leaflets is the pathological hallmark of NBTE (figure 1). Vegetations may be microscopic or large in size with a clustered, wart-like appearance, although diffuse leaflet thickening may develop in the chronic, treated phase of the disease.18 They may occur anywhere on the endocardial surface, with a predilection for the left-sided heart valves.5 12 19 Potential mechanisms include the combination of sheer stress on the mitral valve arising from turbulent flow and oxidative stress compared with low pressure flow of de-oxygenated blood in the right heart. Unlike conventional infective endocarditis, these vegetations are not associated with inflammation or bacteraemia. The valves are usually previously undamaged but NBTE can also arise in patients with pre-existing valve disease.7
In infective endocarditis, underlying damage to the valve endothelium through trauma or other phenomena is frequent. Bacteria then adhere to this damaged endothelium and propagate, resulting in formation of a vegetation that promotes activation of the clotting cascade with fibrin and platelet deposition over the clusters of bacteria. In turn, this often leads to valve destruction and failure, which is rare in NBTE.
The aetiology of NBTE is poorly understood and a number of different interacting mechanisms (including circulating immune complexes, hypercoagulable states and carcinomatosis) may play a role, ultimately resulting in endothelial damage and exposure of the subendothelial connective tissue to circulating platelets (figure 2).

The overlapping causes of non-bacterial thrombotic endocarditis.
Immune mechanisms
Pathophysiological studies in patients with SLE have demonstrated deposition of immunoglobulins and complement complexes along the edges of valve leaflets and within valvular vegetations, suggesting a major pathogenic role of immune complexes in mediating valvular tissue injury.20 21 Patients with SLE and secondary APLS have a similar prevalence of valvular involvement to those with SLE alone and no detectable anticardiolipin antibodies.19 NBTE may also occur (though less commonly) in patients with primary APLS. Although it was originally thought that APLS promoted a hypercoagulable state with thrombus formation and NBTE, it is now recognised that it may also mediate valve damage by direct immune-mediated reactions. Patients with APLS and valve involvement have higher circulating levels of anticardiolipin antibodies directed against negatively charged phospholipids present in endothelial cell membranes.21–23
Hypercoagulable states
Impaired antithrombotic mechanisms in patients with APLS, malignancy and hypercoagulable states are implicated in the pathogenesis of thrombosis and subsequent valve lesions. The instigating factor is unknown but it is likely that endothelial damage provides the foundation for deposition of platelets and fibrin in an already prothrombotic state.
In addition to APLS, there is an association between patients with coagulation abnormalities suggestive of DIC and NBTE. In one study, 50% of patients with DIC were found to have NBTE, supporting the view that these conditions are related and result from a hypercoagulable state.17
Carcinomatosis
The association of NBTE with malignancy (particularly adenocarcinomas of the pancreas and lung) is well known.16 Macrophages interact with malignant cells to produce circulating cytokines (such as tumour necrosis factor and interleukin-1) that cause endothelial damage with consequent promotion of sterile thrombi and platelet disposition.24 These macrophages also stimulate production of clotting factors to create a hypercoagulable state.22 Patients with advanced malignancy may also have clotting abnormalities suggestive of DIC, further promoting a hypercoagulable state.17 The combination of these mechanisms results in thrombotic valve lesions in these patients.
Diagnosis
Diagnosis requires a low index of clinical suspicion. Investigations and assessment should be aimed at differentiating NBTE from infective endocarditis (including culture-negative infective endocarditis), identifying systemic embolism, assessing the valve lesions and defining the underlying cause.
Clinical features
Patients are most commonly asymptomatic and systemic embolism is the principal clinical manifestation. The lack of inflammation at the site of valve attachment means that vegetations are more friable than those seen in infective endocarditis, with a high incidence of embolism, particularly to the spleen, kidney or digits (figure 3). Cerebral and coronary emboli are less common but more likely to manifest with symptoms.6–8 25
Clinical signs and symptoms suggestive of the underlying condition predisposing to NBTE may also be apparent (eg, anorexia and cachexia in advanced malignancy, cutaneous lesions, arthralgia and synovitis in SLE or other autoimmune conditions). Valve destruction is infrequent. Patients rarely present with murmurs or signs and symptoms of valve insufficiency and heart failure. In those that do, valve regurgitation is more common than stenosis7 (figure 3).

Digital infarcts in a patient with NBTE and metastatic colon cancer. NBTE: non-bacterial thrombotic endocarditis.
Laboratory investigations
Blood cultures/microbiology: Diagnostic work-up for infective endocarditis should be performed to differentiate infective endocarditis from NBTE. Three sets of blood cultures should be taken prior to commencing antibiotic therapy. To differentiate between NBTE and culture-negative infective endocarditis, typical and atypical infective endocarditis organisms (including fungi, HACEK group, Coxiella or chlamydia) should be sought using specialised techniques. PCR may be performed on the tissue of explanted valves (or blood PCR if available) to look for fastidious organisms such as Tropheryma whipplei, Coxiella burnetii and Bartonella species, where appropriate. Serial negative blood cultures and atypical serology are required for a diagnosis of NBTE. However, negative blood cultures can be misleading and are observed in up to 30% of cases of infective endocarditis, often as a result of prior antibiotic therapy.26
Blood tests: Extended coagulation screening and clotting factor assay should be performed, including prothrombin time, partial thromboplastin time, fibrinogen, thrombin time, D-dimers and cross-linked fibrin degradation products to assess for clotting disorders or evidence of a hypercoagulable state.
Immunological testing: Tumour markers, ANA, ENA, anti-dsDNA, rheumatoid factor, anticardiolipin antibodies and anti-β2-glycoprotein 1 antibodies should be measured to exclude any associated underlying autoimmune condition.
Imaging
Echocardiography: Despite low diagnostic yield, a transthoracic echocardiogram should be performed to look for vegetations on the heart valves if NBTE is suspected. It is important to note that the echocardiogram may be normal if the vegetation has already embolised. Transoesophageal echocardiography has greater sensitivity than transthoracic imaging, particularly in patients with small vegetations (<5 mm) and should be performed in patients with a normal transthoracic echocardiogram and a strong suspicion of NBTE.27 Vegetations of infective and non-infective aetiology cannot be differentiated on echocardiography. However, vegetations seen in NBTE are usually small (<1 cm), broad based and irregular in shape (figure 4).

Transthoracic echocardiographic image (parasternal long axis) demonstrating a vegetation (arrowed) on the mitral valve in a patient with metastatic lung cancer and associated NBTE. NBTE: non-bacterial thrombotic endocarditis.
Cardiac magnetic resonance (CMR): There are only limited case reports describing the role of CMR in diagnosis of NBTE.28 The higher resolution of CMR should enable identification of smaller valve structures and it may well have a diagnostic role in the future.29
Positron emission tomography (PET): Although commonly used in the diagnosis of prosthetic valve infective endocarditis or device-related infection, CT-PET has low sensitivity in native valve endocarditis and there are limited data concerning its use in the diagnosis of NBTE.30 A single case report has demonstrated increased tracer uptake in valve lesions associated with NBTE.31 32
Whole-body CT and MRI brain imaging should be performed in patients with suspected NBTE to look for evidence of systemic embolism (figure 5).
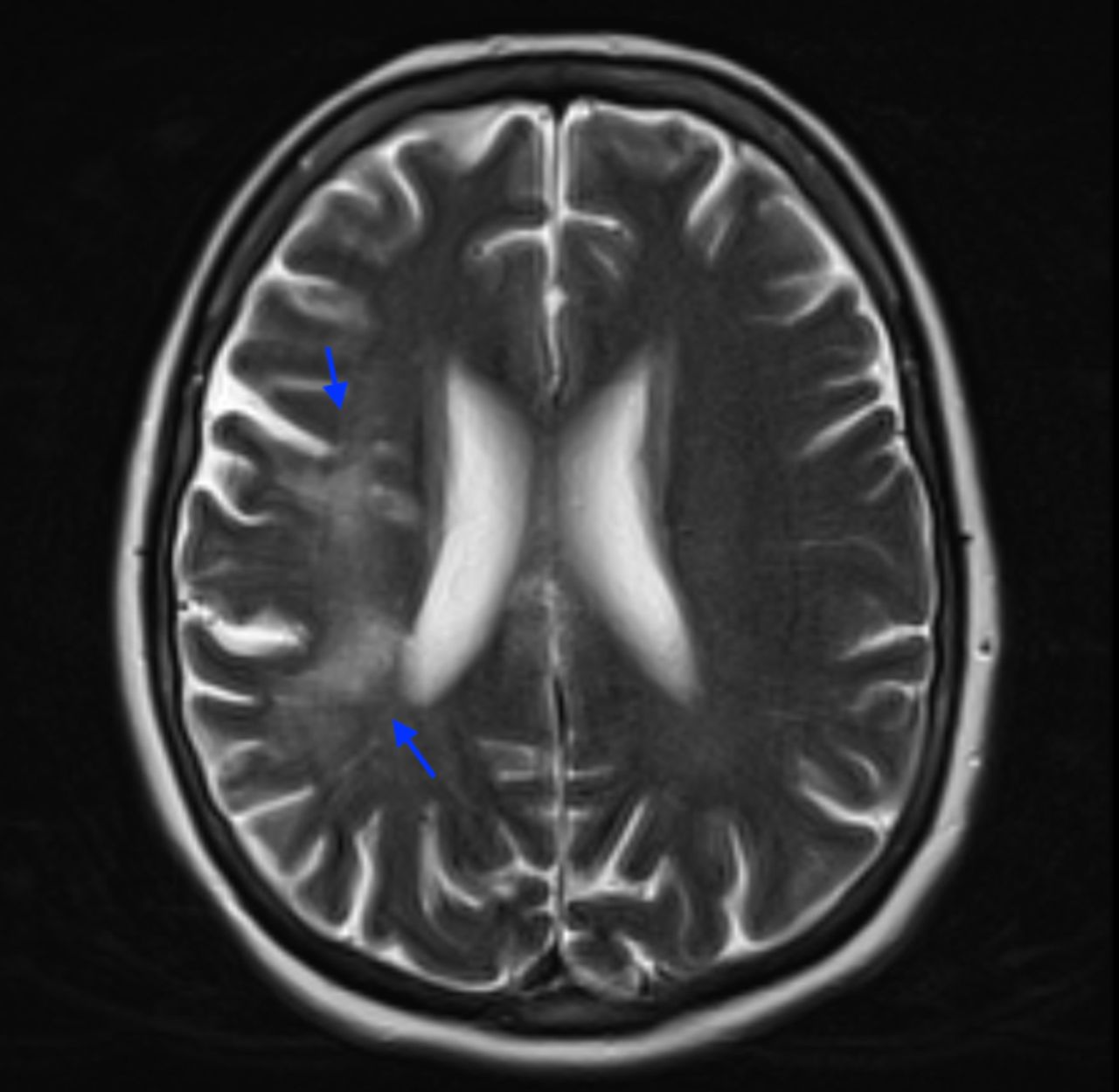
MRI brain of the same patient with end stage lung cancer, later diagnosed with NBTE, demonstrating multiple cerebral infarcts (arrowed). NBTE: non-bacterial thrombotic endocarditis.
Histology
Imaging tools are unable to distinguish between sterile vegetations and those of infective origin. Diagnosis can therefore only be confirmed on histological assessment.
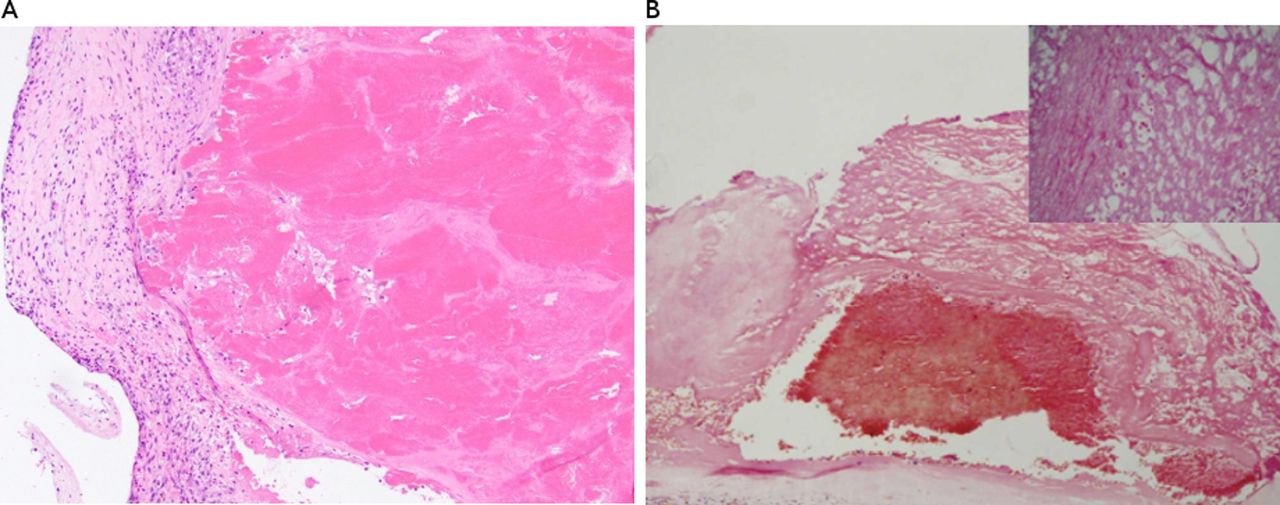
Vegetations vary in size and are usually located at sites of turbulent flow along the lines of valve closure or on the leaflets themselves.10 18 33 The valve lesions have similar histological appearances regardless of the underlying aetiology, consisting of degenerating platelets interwoven with fibrin strands, granulomatous tissue and fibrotic foci (figure 6).10 15 Inflammatory cells and infective microorganisms are absent.10 33 Histopathological examination also allows the diagnosis of primary cardiac malignancies, such as angiosarcoma and myxoma.

Typical appearances of vegetations (arrowed) on the mitral valve in NBTE (Asopa S et al 41). NBTE: non-bacterial thrombotic endocarditis.
In summary, the diagnosis of NBTE can only be confirmed by demonstration of platelet thrombi at autopsy or on histological examination of surgical specimens. A high index of clinical suspicion is therefore required for diagnosis. Patients with a high likelihood of the diagnosis of NBTE are those with a predisposing condition, features of systemic emboli and valve lesions with no evidence of associated infection (or valve masses that fail to respond to antibiotic therapy) (table 2).
Clinical features and diagnostic investigations differentiating NBTE from infective endocarditis
Treatment
Treatment of NBTE is aimed at identification and treatment of the underlying condition, and reducing the risk of systemic embolism. Surgery is rarely indicated, except in those patients with haemodynamic compromise or refractory heart failure. Unless there is a contraindication, all patients with a clinical diagnosis of NBTE should receive anticoagulant therapy.
Treatment of the underlying disease
Treatment should target the underlying autoimmune condition or malignancy, although there are limited data to demonstrate impact on the valve lesions.22 Underlying malignancy is often advanced with poor prognosis and palliative treatment may be most appropriate.
Patients with SLE should receive immunosuppressant therapy under the care of a specialist rheumatology team. NBTE associated with SLE may arise at any stage of the disease process (including the chronic treatment phase) and appears to be unrelated to disease activity.18 34 Treatment does not reduce the incidence of associated valve lesions—indeed, their incidence appears to have increased with improved immunological management and prolonged survival.
Anticoagulation
Systemic embolism from friable vegetations is common and unless there is a contraindication, all patients with a diagnosis of NBTE should be anticoagulated with low molecular weight heparin, unfractionated heparin or warfarin.7 35 Some studies have suggested that warfarin is less effective than heparin in preventing thromboembolic events in patients with malignancy.7 36 37 There is currently no evidence supporting the use of non-vitamin K antagonist oral anticoagulants. A recent trial comparing warfarin and rivaroxaban in the treatment of thrombotic APLS suggested an increased risk for recurrent thrombosis in rivaroxaban-treated patients.38 The risk of recurrent embolism is high and anticoagulation should be continued indefinitely unless there are major bleeding complications.
Heparin reduces the incidence of recurrent cerebral emboli (without promoting brain haemorrhage) in patients with NBTE presenting with ischaemic stroke.39 Management should be undertaken in conjunction with a Stroke Team, with cerebral imaging prior to anticoagulation and a low threshold for repeat imaging if new neurological signs are detected.
Surgery
Valve surgery is seldom required in the treatment of NBTE since the valve itself is usually undamaged, recurrent vegetations are common and the risk of surgery often outweighs the potential benefits (particularly in patients with advanced malignancy).7 14
There are no current guidelines as to which patients should undergo surgery, but intervention may be considered in patients who are haemodynamically unstable and those with acute heart failure of valvular origin, recurrent thromboembolism despite therapeutic anticoagulation or large left-sided vegetations with high embolic potential. Valve sparing surgery is frequently feasible35 (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary of treatment strategies in NBTE. NBTE: non-bacterial thrombotic endocarditis.
Prognosis
The condition is rare and no formal studies have examined the prognosis of patients with NBTE. Clinical experience demonstrates that the prognosis is usually poor, largely due to the strong association with advanced malignancy and recurrent systemic embolism.7–16 In one study, the incidence of ischaemic cerebral events in Libman–Sachs patients was 15% over 4-year follow-up.9
Follow-up
There are no current guidelines for the follow-up of patients with NBTE, although frequent monitoring (initially every 2–6 weeks) is important to exclude recurrent systemic embolism, ensure adequate anticoagulation and freedom from bleeding or thrombocytopaenia. Interval echocardiography (initially every 2–3 months) should be undertaken to monitor the progression or regression of valve lesions.
Conclusion
NBTE is a rare condition associated with autoimmune disease, malignancy and hypercoagulable states, and characterised by sterile friable vegetations composed of fibrin and platelets with high risk of systemic embolism. Most patients are asymptomatic and the condition is commonly diagnosed at post-mortem. A high index of clinical suspicion is therefore required for diagnosis. Management requires differentiation of NBTE from infective endocarditis, definition of the underlying cause, assessment of valve lesions with echocardiography and prevention of systemic embolism by means of anticoagulant treatment. Surgery is rarely indicated, except in patients with haemodynamic compromise, valve failure or high risk of embolism.
Key points
Non-bacterial thrombotic endocarditis (NBTE) is a rare condition characterised by the formation of sterile vegetations composed of fibrin and platelets on heart valves.
These sterile vegetations can develop in a number of conditions, including autoimmune disease, malignancy and hypercoagulable states.
Investigation involves differentiation of NBTE from infective endocarditis, definition of the underlying cause and assessment of valve lesions with echocardiography.
Systemic embolism from friable vegetations is common and all patients with a diagnosis of NBTE should be anticoagulated unless there is a contraindication.
Valve destruction is infrequent. Surgery is rarely indicated except in patients with haemodynamic compromise, valve failure or high risk of embolism.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Supplemental material
Supplemental material
References
Footnotes
Twitter @robertsthomson
Contributors All the listed authors on this paper fulfil the criteria of authorship. They have all substantially contributed to the content of this review article and have approve the final submitted version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information
Author note References which include a * are considered to be key references.