Article Text

Statistics from Altmetric.com
Learning objectives
To understand the impact of the COVID-19 pandemic on the management of severe aortic stenosis (AS).
To appreciate the evidence base supporting transcatheter aortic valve implantation (TAVI) as a treatment for AS.
To gain insights into how to select patients for TAVI during the COVID-19 crisis and adapt the AS pathway appropriately.
Introduction
The current COVID-19 outbreak presents an unprecedented challenge to health services worldwide. With the primary goal of reducing the risk of spread of COVID-19, protecting patients and healthcare teams and preserving access to necessary/emergency care, the UK National Health Service (NHS) issued specialty guidance for the management of cardiology patients during this time.1 All hospital trusts were advised early to defer non-urgent cardiovascular diagnostics and interventions and from an early stage, virtually all cardiac surgery ceased, apart from emergency cases. Patient pathways were modified to ensure the highest risk patients could continue to access urgent cardiac care (eg, patients presenting with ST-elevation myocardial infarction (MI)). The underlying aim was to ensure that emergency services remained resilient throughout what was then an unknown onslaught. This guidance was tailored to subspecialty areas including heart failure, arrhythmia, coronary disease and valvular heart disease, in particular the management of aortic stenosis (AS).
AS is common and affects patient groups particularly vulnerable to a poor outcome with COVID-19 infection, with an overall prevalence of clinically significant AS in those greater than 70 years approximately 1%–3%.2 Severe, symptomatic AS has a uniformly poor prognosis, with an estimated 1-year mortality of up to 40%,3 worse than many metastatic cancers. No medical therapy influences outcome, and the only available prognostic treatment is valve replacement/implantation.4 While surgical valve replacement (sAVR) was the treatment of choice for decades, transcatheter aortic valve implantation (TAVI) has become an increasingly safe and effective treatment option in patients at high or intermediate risk.5
There has been a dramatic growth in TAVI in recent years with 5197 TAVI procedures performed across 41 centres in the UK in 2018/2019 (approximately 78 per million population), an exponential rise mirrored in most developed countries.6 This dramatic growth in TAVI has been driven by technical and clinical advances. Devices have developed to allow more effective treatment to a more diverse and progressively lower risk group of patients.7 TAVI valves have become more sophisticated with lower profile delivery systems, with less paravalvular leak (PVL) and decreased need for permanent pacing.8
Further to this, the transcatheter procedure has itself evolved and become much more straightforward, with the fully percutaneous transfemoral route being the access of choice.9 The increasing experience and plateauing of learning curves has reduced periprocedural complications. Patient selection with the multidisciplinary Heart Teams has important advantages over solitary decision making.10 Perhaps as a result, evidence from recent trials has demonstrated equivalent or superior outcomes with TAVI when compared with sAVR in patients at intermediate or even low risk.11–13 The European Society of Cardiology/European Association for Cardio-Thoracic Surgery guidelines have recently been amended to include TAVI as an option for intermediate risk patients, after Heart Team involvement (figure 1).14

The latest guidelines illustrate that TAVI should be considered for patients at intermediate surgical risk from: Nishimura et al, American Heart Association/American College of Cardiology (AHA/ACC) guidelines, JACC 20017;70:252–89 (TAVR: TAVI). AS, aortic stenosis; AVR, aortic value replacement; TAVI, transcatheter aortic valve implantation; TAVR, transcatheter aorticvalue replacement.
During this global pandemic, continued access to TAVI for those already on waiting lists was deemed essential to ensure patients (who have extremely poor short-term and intermediate-term outcomes if untreated) received timely and potentially life-saving care. A specific advantage of TAVI in this setting is the lack of need for ITU or mechanical ventilation (as most cases are now performed using conscious sedation). The COVID-19 guidance therefore included the principle that patients who may have been accepted for sAVR could be ‘diverted’ to TAVI under the guidance of the Heart Team.
The rationale for performing TAVI in the COVID-19 crisis is therefore:
Critical AS carries a very high monthly mortality making the risk on the waiting list high.
The risk of TAVI rises as the disease advances making the procedure more challenging if patients wait longer.
Decompensated patients with critical AS spend a long time in hospital when not treated, thus using precious resources and increasing their vulnerability to nosocomial COVID-19 infection.
Unlike sAVR, TAVI is a procedure that (usually) requires no ventilation or use of critical care capacity. Moreover, much urgent cardiac surgery is suspended during the surge phase of the COVID-19 crisis mandating a greater delay to treatment for those on the sAVR waiting list.
TAVI length of stay is short, and patients are therefore subjected to less risk of acquiring COVID-19 during their hospital stay.
The literature shows equivalent outcomes to sAVR in all but low-risk patient groups.
This article seeks to explore and challenge some of these issues.
What is the monthly mortality on a TAVI waiting list?
Patients with severe symptomatic AS have poor overall survival without definitive treatment.15 In a surgical cohort, the risk of mortality while waiting for sAVR is most pronounced during the first 6 months after the referral date (3.7% at 30 days and 11.6% at 6 months).16 Outcome data from the PARTNER 1 trial (which compared TAVI with medical therapy in an inoperable risk patient group) showed an all-cause mortality of 50.7% at 1 year in the untreated group.17 Even for asymptomatic patients, long-term survival is poor, with a mortality of 21.1% at 3 years from diagnosis,18 suggesting that all severe AS patients do poorly in the long term in the absence of intervention.
Sudden cardiac death can occur with asymptomatic severe AS (without intervention) at a rate of approximately 1 in a 100,19 and may occur without any prodromal symptoms. Should symptoms develop, clinical deterioration may progress rapidly, and the risk of sudden death can escalate if AS is managed conservatively (4% at 1 month, 12% at 6 months).20 In a recent study of AS patients with a high probability of LV decompensation, more than 50% were either dead or hospitalised with cardiac failure within 2 years.21
Timing of intervention is also crucial, as perioperative morbidity is markedly increased if advanced left ventricular systolic dysfunction occurs due to a delay in intervention.22 23 Registry data unsurprisingly reveal greater mortality during the preoperative period for patients with established heart failure and advanced myocardial scarring.24 There is an increasing awareness that aortic valve intervention is often performed too late, and several studies are examining the effects of earlier intervention in presymptomatic patients.25
Is it reasonable to convert patients selected for sAVR to TAVI: the current data for TAVI in low risk patients?
Is ‘diversion’ of patients already accepted for sAVR to TAVI supported by the current evidence? The indication for TAVI has recently been expanded to include patients with intermediate surgical risk.26 The PARTNER 2A trial, which randomised 2032 patients with intermediate surgical risk (Society of Thoracic Surgery Predicted risk of Mortality (STS-PROM) score 4%–8% and Heart Team consensus) to either TAVI or sAVR, demonstrated equivalent outcomes at 2 years.27 A subsequent subgroup analysis showed superiority for the transfemoral TAVI cohort, when compared with the sAVR group.28 TAVI patients recovered faster post-procedure and had shorter in-hospital stays.29 The SURTAVI trial recruited 1764 intermediate risk patients and randomised them to TAVI with the self-expanding CoreValve or CoreValve Evolut R prostheses or sAVR.30 Again, there was no difference in the primary endpoint between both groups. The 2017 European guidelines emphasise that either intervention is reasonable in this group of patients, with treatment selection made by the local Heart Team on an individualised basis.
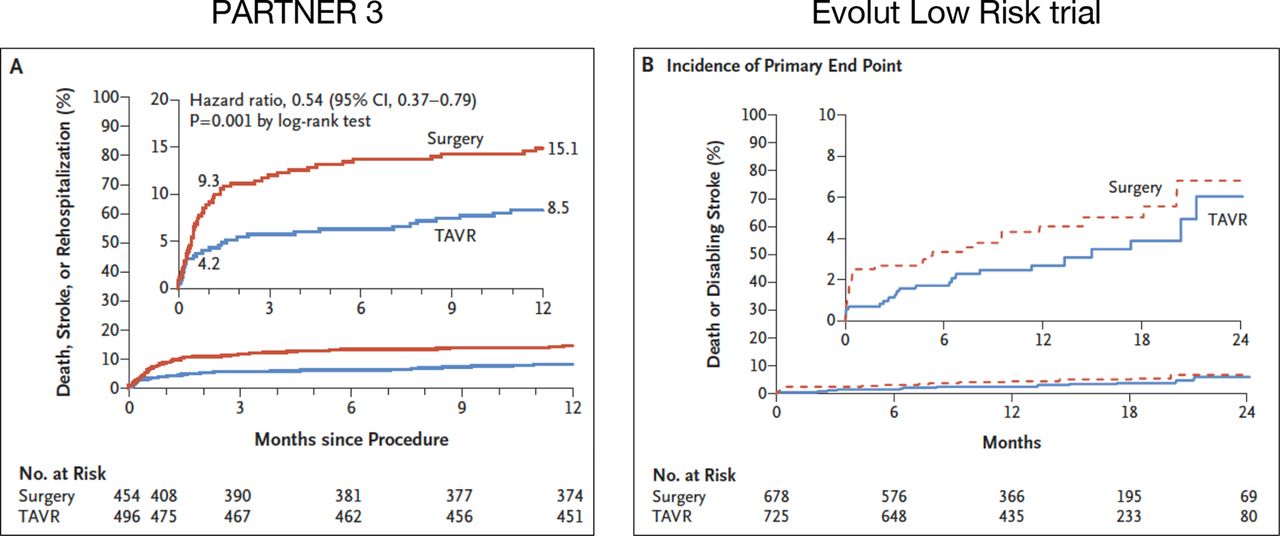
Consequent to these data, several prospective randomised trials were undertaken to evaluate outcomes after TAVI in patients at lower operative risk. In PARTNER 3, patients at low surgical risk were randomised to TAVI with the Sapien 3 device or sAVR. This trial showed a lower rate of the composite of death, stroke or rehospitalisation at 1 year with TAVI than with sAVR.31 The global, prospective, multicentre Evolut Low Risk Trial also showed TAVI to have an excellent safety profile and to be an effective treatment option in low-risk patients, with shorter hospital stays and improved quality of life (figure 2).32 As a result of these two pivotal trials, the US Food and Drug Administration (FDA) expanded the indications for use for both the Edwards Lifesciences’ Sapien 3 valve and Medtronic’s CoreValve Evolut systems in low-risk patients in August 2019. The Edwards Sapien 3 valve also received European CE mark for low-risk patients in November 2019.

Both the PARTNER 3 and the Evolut Low Risk trials showed favourable performance of TAVI versus surgical aortic valve replacement (AVR) in low-risk patients (TAVR: TAVI) from refs 31 and 32. TAVI, transcatheter aortic valve implantation.
However, these two studies did include high levels of patient selection and the mean age of patients was still >70 years. There are additional challenges with TAVI in younger and lower risk patients. These include:
TAVI valve durability
The evidence supporting TAVI valve durability and function is still not completely robust, and more data (particularly long term) are needed. Echocardiographic follow-up of the PARTNER 1a and 1b trials demonstrated stable haemodynamic valve parameters after TAVI over 5 years but longer term follow-up is lacking.33 The results have been similar in other series and for self-expanding transcatheter aortic valves.34 Mechanical issues with TAVI valves may also become an issue; subclinical leaflet thrombosis, which occurs at a significantly higher incidence after TAVI compared with sAVR, has unknown clinical significance and haemodynamic consequences,35 and this will need to be studied further. Prosthesis degeneration, valve durability and the need for aortic valve reintervention will also need to be further evaluated in this group of younger patients. Although valve-in-valve procedures have demonstrated encouraging results in patients with degenerated surgical aortic bioprostheses,36 whether these results can be achieved for valve-in-valve procedures in degenerated TAVI valves remains to be seen.
Paravalvular leak
Although there has been progress with newer valve designs, rates of PVL have been consistently higher in trials after TAVI compared with surgery, and it is well established that there is an adverse effect of significant PVL on long-term outcomes.37
The need for permanent pacing
Permanent pacemaker rates have also been higher in TAVI patients, particularly with the self-expanding valves.38 While pacing rates seem to be lower in younger patients (with healthier cardiac conducting systems) as demonstrated in the PARTNER 3 study, there is concern that pacing will have a greater impact in the treatment of younger patients who may need multiple generator changes throughout their lifetimes and be subject to longer term right ventricular pacing.
The higher incidence of bicuspid valve anatomy
Congenitally bicuspid aortic valve anatomy is more common in younger patients because these valves degenerate earlier than normal tricuspid aortic valves. Data from retrospective registries have demonstrated lower procedural success, higher stroke rates and higher residual PVL after TAVI in patients with bicuspid compared with tricuspid aortic valve disease.39 However, implantation of new-generation devices has improved outcomes, suggesting that TAVI may become a valid treatment option in bicuspid aortic valve disease in the future.
It seems therefore that while there are some data to support TAVI in low-risk patients, this is by no means complete and questions remain. Offering TAVI to low-risk patients already listed for sAVR during the COVID-19 crisis would therefore have to be done by Heart Teams on an individual basis, recognising the fact that this is (at present) outside the current guidelines.
Encouraging a streamlined TAVI pathway during the COVID-19 crisis
It is clear that any revised pathway during the COVID-19 pandemic will need to be streamlined and efficient with minimum use of hospital/personnel resource and minimal exposure of the vulnerable TAVI patient to potential COVID-19 infection. A number of questions arise in pathway design:
Should case selection be any different?
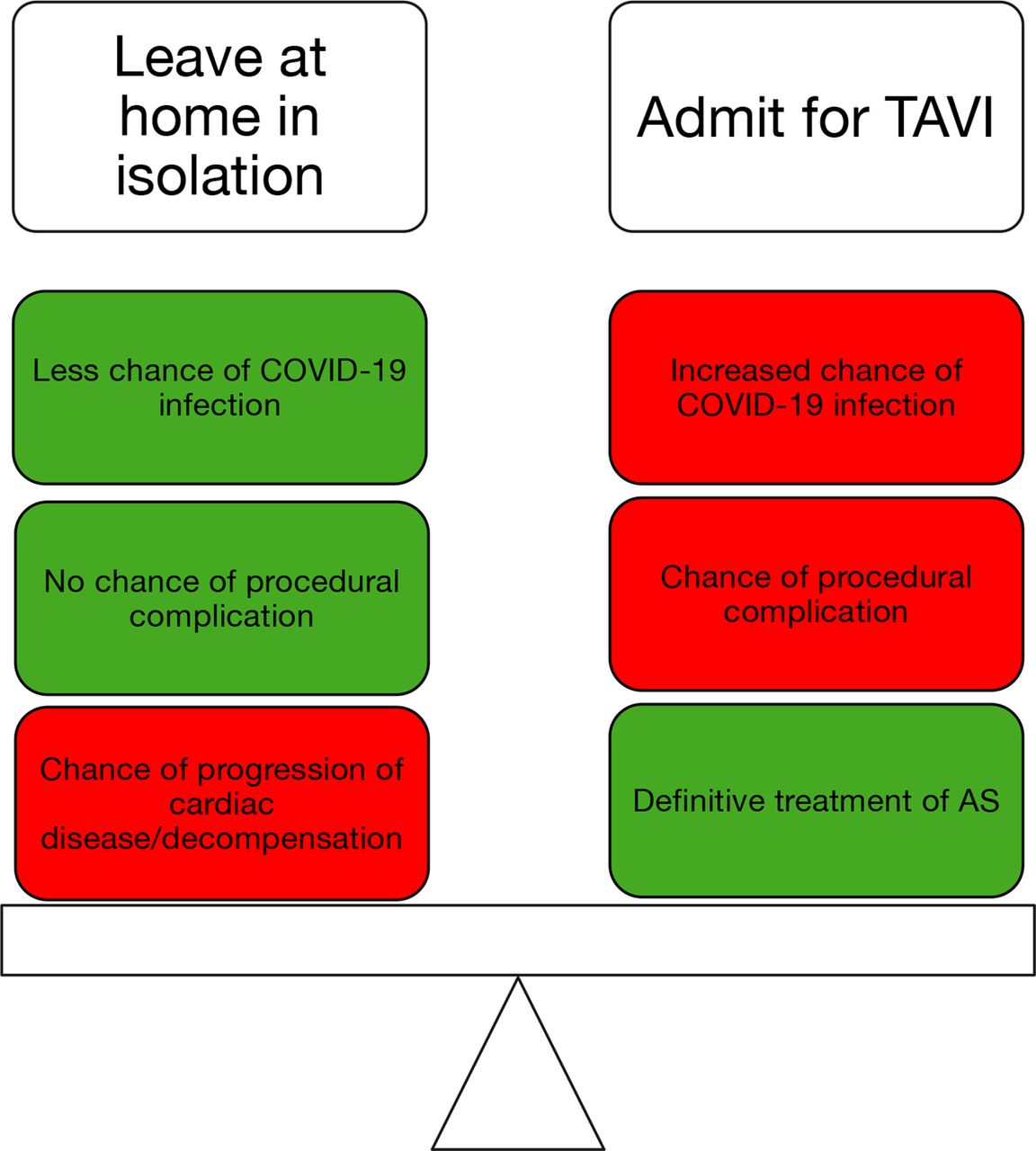
Great care should be taken when straying from best practice and well-evidenced guideline-driven therapy. However, the risk benefit equation that we all use in clinical decision making has changed in this surreal environment. We are now faced with an additional risk of exposing the vulnerable patient to infection with a potentially lethal virus so the case selection has to take account of this, particularly with patients not already in hospital: the risk of leaving the patient safely isolated at home with their untreated AS versus the risk of potentially exposing them to COVID-19 but treating their AS (figure 3).
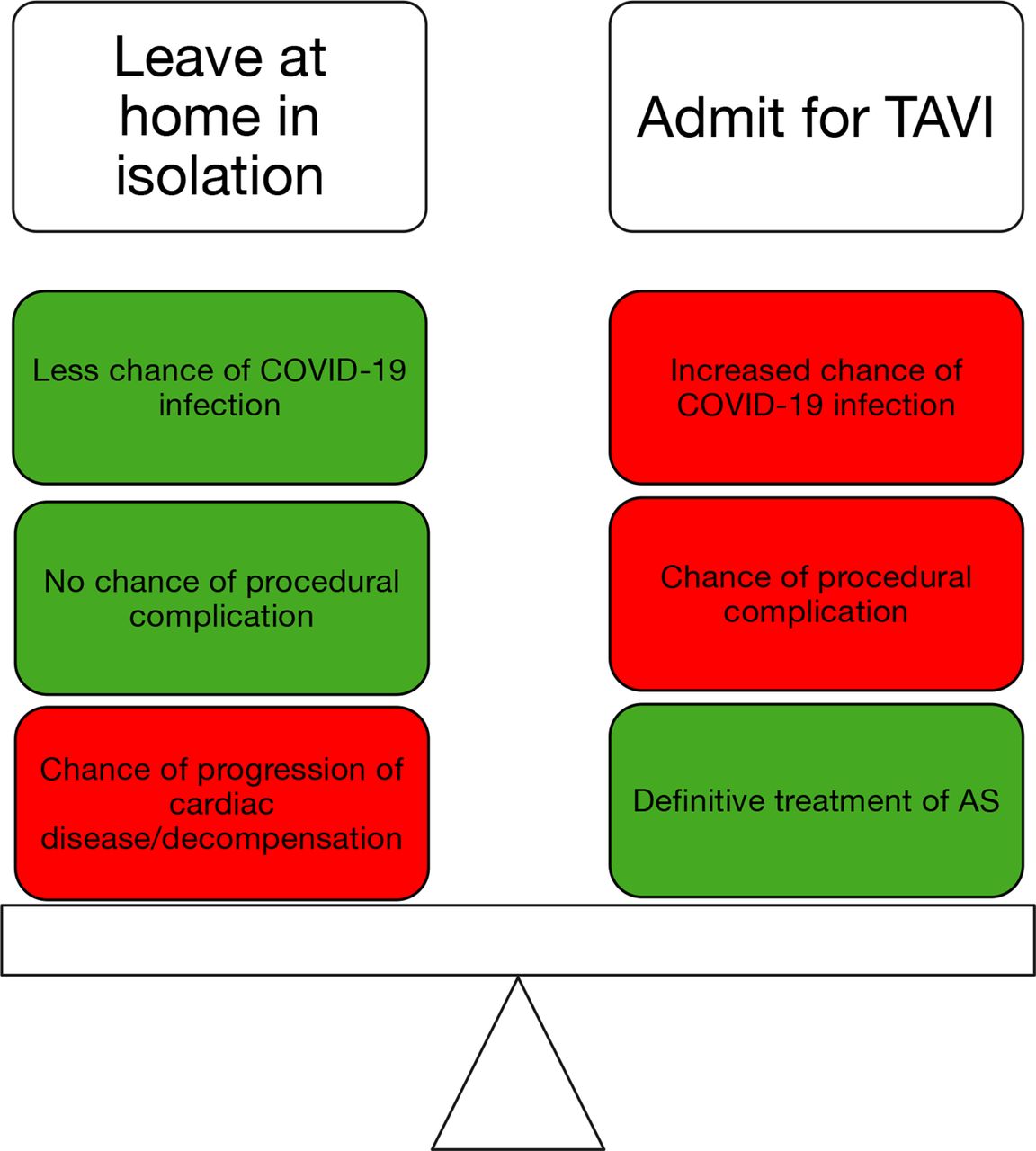
The decision to admit for a TAVI procedure in the COVID-19 crisis is a delicate balance of risks between leaving patients relatively safe from COVID-19 but with untreated AS versus admitting and treating the AS but potentially exposing the vulnerable patient to COVID-19. AS, aortic stenosis; TAVI, transcatheter aortic valve implantation.
Should the work-up be any different?
The work-up investigations should be streamlined and minimised. If the patient is an outpatient, then a single trip to a COVID-19 free centre would be optimal. Transoesophageal echocardiography is aerosol generating and should be avoided. If a good quality gated CT coronary angiogram is obtained for device sizing, then an invasive coronary angiogram may not be necessary.
Is there a role for balloon aortic valvuloplasty (BAV)?
Some have advocated the use of BAV instead of more definitive treatment to expedite discharge, but this may just delay the problem without any proven prognostic benefit and a procedural risk close to that of TAVI.
Should the procedure be done differently?
It is also dangerous to stray from a procedure that has evolved through painstaking iterations over many years, but there is a good case for making the procedure as simple as possible and using the TAVI prosthesis with which the operator/institution is most familiar. Some centres have offered TAVI without the option of surgical bail-out, but this should be discussed with the Heart Team (and perhaps the broader clinical leadership/ethics committee in the hospital) and the patient, ideally being incorporated into the consent process.
Should length of stay be shorter?
Current advances in TAVI have allowed for shorter inpatient hospital stays postimplantation, in particular for transfemoral procedures.40 Numerous studies have evaluated the safety of early discharge. In a retrospective review of 393 patients, of whom 38% were discharged within 48 hours, there was no difference in terms of 30-day mortality, rehospitalisation or disabling stroke between the early and standard discharge groups.41 Similar outcomes were noted in another study of 337 transfemoral TAVI patients.42 In a different group of 120 patients that underwent TAVI at a single centre, 55% of patients were discharged on either the same day as the procedure, the following day or within 72 hours of their intervention.43 These preliminary studies have provided supportive evidence that early discharge after TAVI is safe and feasible and indeed now that median length of stay in the UK is down to 3 days, it should certainly be feasible during the pandemic (table 1).
Factors to consider doing differently along the patient pathway for AS during the COVID-19 crisis
The ethics of TAVI in the COVID-19 pandemic
During the planning of emergency healthcare services during the COVID-19 pandemic, there has been extensive discussion about the ethics of who should be treated actively (eg, ventilated) and whom should receive only palliation. Some have questioned any investment in the treatment of elderly patients with AS when young people are dying of COVID-19. Of course, unlike COVID-19, there is a well-evidenced and deliverable treatment for AS, and moreover, early definitive treatment of AS will reduce length of stay and free up hospital capacity.
A step-wise plan in responding to COVID-19
Creating capacity during the COVID-19 surge phase
The capacity of health systems to respond to COVID-19, especially in countries experiencing large case numbers, has been a great concern. Data from China, Italy and Spain suggest that a sizeable proportion of those infected with the novel coronavirus will be admitted to hospital, with as many as 10% of cases requiring intensive care unit admission.44–46 For those admitted to intensive care requiring ventilation, the majority will require respiratory support for up to 2 weeks,45 46 and a poor prognosis is being reported in this patient group.47 These experiences with COVID-19 highlight the fact that creation of surge capacity, which is the ability of a health system to cope with a sudden and unexpected influx of patients in an emergency or disaster situation, will be required.
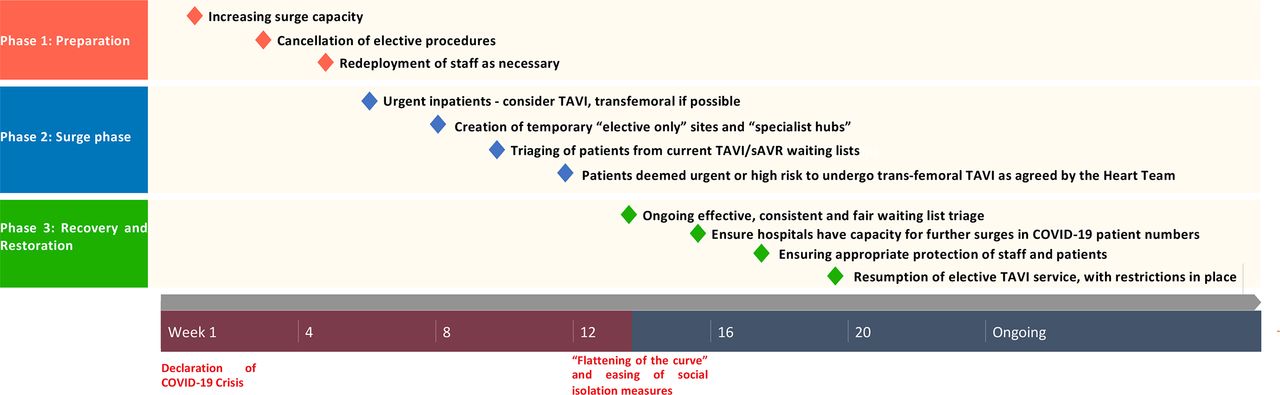
Surge capacity can be created from a reallocation of resources, both intrinsic and extrinsic.48 As part of this process, guidance issued in the UK recommended progressive postponement of all but the most urgent elective surgery (in all specialties) and internal repurposing of operating theatres, recovery rooms, intensive care beds and staff. A consensus document issued by the NHS and the Royal Colleges of Surgeons advises deferring surgical intervention for up to 4 weeks, unless there is deteriorating clinical status.49 These time intervals may not accord with usual clinical practice and may result in greater risk of an adverse outcome. TAVI activity will be restricted to an absolute minimum during this crisis phase (inpatients who cannot be discharged safely) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A step-wise plan to modify TAVI services during the COVID-19 pandemic. sAVR, surgical valve replacement; TAVI, transcatheter aortic valve implantation.
After surge capacity is created and there is confidence that hospital capacity for COVID-19 is resilient, new pathways need to be designed to manage patients already in hospital or some way along the pathway (eg, waiting for multidisciplinary meeting (MDM) discussion). One option in dealing with this situation if possible is to create temporary ‘elective-only’ sites, with aortic valve intervention being performed at specialised hubs for those patients on current waiting lists that are deemed urgent. Keeping these sites (relatively) ‘COVID-19-free’ would be easier to allow safer cohorting of patients and potentially less exposure of vulnerable patients to the virus. In the early phases of the outbreak, additional capacity can be sourced from the private sector to ensure that aortic valve surgery and elective TAVIs can be completed before the predicted surge in demand. Emergency legislation has been passed in the UK that has enabled the NHS to take over the management of such facilities and services to ensure a fully available, cost-effective national response effort to the pandemic. These measures allow for more hospital beds and resources to be available for dealing with the increasing COVID-19 inpatient numbers while maintaining operability across the UK. These solutions will depend on local resources.
Triage of patients from the TAVI/sAVR waiting list
Most agree that patients with AS waiting for TAVI should be ‘risk stratified’ in some way. For general surgical procedures, the Royal College of Surgeons in the UK have advised ‘Priority levels’ from 1a/b (emergency/urgent) to 4 (those that can be safely delayed for >3 months).49 Others have merely divided patients into ‘high risk’ or ‘essential’ and ‘normal/low risk’ or ‘non-essential’.50 Any stratification should follow certain objectives that reflect core ethical principles. Any clinicians making these decisions will have to balance the likely risks and benefits for individual patients while also considering societal needs during this pandemic. The most urgent of patients could be determined using numerous criteria, which would need to be standardised. Risk scores and calculators may be created to identify patients who may deteriorate and require unplanned hospitalisation and urgent TAVI.51 These criteria could include clinical metrics (syncope, New York Heart Association (NYHA) class IV symptoms, comorbidities and previous admission with heart failure) or investigation endpoints (N-Terminal Brain Natriuretic Peptide (NT-pro-BNP), gradients across the AV, valve area and LV systolic function) table 2.52 53 Historical clinical prediction models that have considered prior episodes of cardiac failure and advanced kidney impairment may also be useful.15
Factors to be considered in identifying higher risk AS patients during waiting list triage
The recovery and restoration plan
Perhaps the most challenging aspect of service delivery is the last phase, the so-called ‘recovery phase’, largely because there are many unknowns and any predicted timeline is guesswork at present. After the surge phase of the COVID-19 pandemic, planning must commence for reintroduction of a TAVI service, but in the absence of an effective treatment for COVID-19, severe restrictions will remain. The principles guiding any recovery plan are: (A) effective, consistent and fair waiting list triage to treat those AS patients most at risk first; (B) respecting the priorities of hospital capacity to deal with patients with COVID-19 and perhaps further surges in patient numbers as ‘social lockdown’ measures are eased; (C) minimising the chance of infecting patients with COVID-19 when they are brought to the hospital for work-up investigations/TAVI procedures; (D) protecting healthcare staff from undue COVID-19 infection; and (E) being as cost-effective as possible,
The detail of any plan will depend on local resource but will involve creating ‘COVID-19-clean’ environments, perhaps by dividing departments or catheter labs, wards or even institutions with appropriate division of staff in these areas.
Quite how the COVID-19 pandemic will affect structural cardiac intervention in the future remains to be seen and will depend on economic recovery and healthcare prioritisation in the coming years.
Conclusions
The unprecedented disruption of the COVID-19 pandemic has created huge challenges for patients with AS and for Heart Teams trying to manage them. The international sharing of experience and research data has helped to create some clarity and perspective, but many hurdles remain. Fortunately, the treatment of AS and TAVI has a large and well-established evidence base to guide clinical practice during this time, although outside the environment of a global pandemic. The introduction of this new variable (COVID-19) has altered (and sometimes confused) clinical decision making and the risk–benefit relationships that underlie our therapies and interventions. However, first principles of good clinical practice should be adhered to wherever possible, such that clinicians do not lose sight of well-evidenced guidelines and patients remain at the centre of all management plans. In doing this, we will successfully navigate the uncharted waters that lie ahead of us.
Key points
The COVID-19 pandemic has had an unprecedented impact of the delivery of cardiovascular care.
The aortic stenosis (AS) pathway has had to change during this crisis, with a different, new risk–benefit balance to consider.
Transcatheter aortic valve implantation (TAVI) is an effective treatment for AS and has less impact on hospital (and particularly critical care) capacity than surgical AVR.
Systematic, fair patient selection/prioritisation is mandatory to maintain a TAVI service at this time.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Supplemental material
References
Footnotes
Contributors BK wrote the first draft of this manuscript and contributed to the revisions and creation of the tables and figures. PM conceived the idea, rewrote the manuscript and edited all versions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article
Author note References that include a * are considered to be key references.