Article Text

Statistics from Altmetric.com
Learning objectives
How to diagnose chronic thromboembolic pulmonary hypertension.
How to decide on best interventional strategy—pulmonary endarterectomy (PEA) versus balloon pulmonary angioplasty (BPA).
Understanding the techniques, efficacy and safety of PEA and BPA.
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) occurs due to persistent pulmonary obstruction and vasculopathy after an acute pulmonary embolism and is underdiagnosed. Patients experience breathlessness and symptoms and signs of right heart failure and without treatment the prognosis is poor. Available interventional approaches include pulmonary endarterectomy (PEA) and balloon pulmonary angioplasty (BPA), as well as pulmonary hypertension-targeted drug therapy. The choice of treatment depends on anatomical, haemodynamic and patient factors and is determined multidisciplinary team assessment. This review will cover the assessment and treatment of CTEPH with a particular focus on PEA and BPA, as well as highlighting future therapeutic directions.
CTEPH is a condition caused by failure of resolution of acute pulmonary embolism (PE) and results in fibrotic tissue deposition and altered vascular remodelling that occludes the pulmonary arteries.1 It has been estimated that between 0.56% and 3% of acute PE develop CTEPH2 resulting in an incidence of 0.9–5.7 cases per million and a prevalence of 8–40 cases per million, although this is likely to be an underestimate as the condition is often under-reported.3 4 Mechanical obstructions and secondary pulmonary vasculopathy cause pulmonary hypertension (PH), right ventricular remodelling and dilatation culminating in breathlessness, a worsening exercise tolerance, presyncope and fatigue that is progressively fatal due to right heart failure.5
Diagnosis of CTEPH
CTEPH is diagnosed in patients with persistent symptoms of breathlessness, evidence of PH at rest (newly defined as mean pulmonary artery pressure (mPAP) >20 mm Hg (rather than >25 mm Hg) in combination with pulmonary arterial wedge pressure ≤15 mm Hg and pulmonary vascular resistance (PVR) ≥3 Wood units (WU)) and imaging suggestive of thromboembolic pulmonary obstruction following 3 months of effective anticoagulation.6 Both ventilation-perfusion scintigraphy (V/Q scan) and CT pulmonary angiography (CTPA) are accurate methods for the detection of CTEPH with excellent diagnostic efficacy (100% sensitivity, 93.7% specificity and 96.5% accuracy for V/Q scan; 96.1% sensitivity, 95.2% specificity and 95.6% accuracy for CTPA).7 Dynamic contrast-enhanced lung perfusion MRI also has a similar sensitivity (97%) for diagnosing CTEPH to V/Q scans.8 However, cross-sectional imaging has the added advantage of determining the distribution of thromboembolic lesions, and this can guide interventional treatment (figure 1). CTPA is currently widely used for assessment of operability, although contrast-enhanced MRI pulmonary angiography can also be used to image the pulmonary vasculature. In addition, cross-sectional imaging provides information on coexisting parenchymal lung disease subtended by diseased pulmonary arteries that may dissuade treatment.

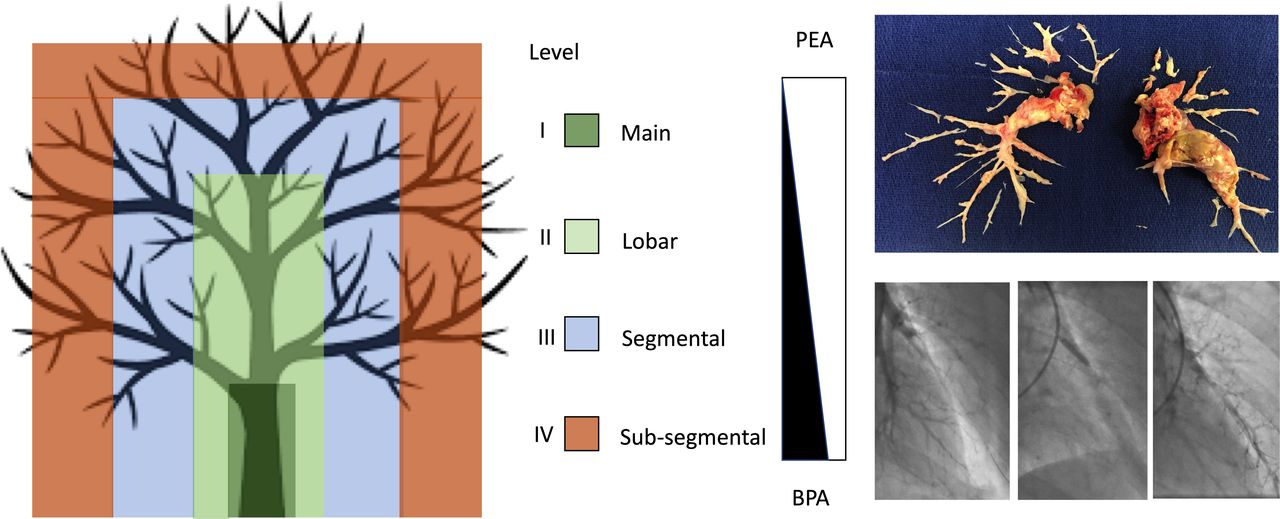
Schematic of the pulmonary artery tree summarising the University of California San Diego chronic thromboembolism surgical classification and how this influences treatment. Upper right panel: pulmonary endarterectomy (PEA) specimen with clearance of level I–IV disease. Lower right panel: balloon pulmonary angioplasty (BPA) tryptic angiographic frames of (1) an occluded left anterobasal (A8) subsegmental branch, (2) semicompliant balloon inflation, and (3) improved contrast opacification distally.
Non-selective and, in particular, selective segmental digital subtraction angiography (DSA), as well as cone beam CT, provide greater resolution and are useful in detecting distal subsegmental disease as well as paucity of lung parenchymal contrast blush and venous return to a territory that may justify treatment by balloon pulmonary angioplasty (BPA). Thromboembolic pulmonary lesions by DSA are often best viewed from the contralateral projection (right anterior oblique for the left lung and left anterior oblique for the right lung) where there is less vessel overlap. Lesions have been described as discrete rings and webs, linear slits, subtotal tapered or total blunt or pouch occlusions, with the latter being more complex to treat by intervention (figure 2).

Images of inoperable chronic thromboembolic pulmonary hypertension (CTEPH): multiple perfusion defects are demonstrated on lung perfusion scintigraphy (A) and patchy lung parenchymal opacification with contrast (mosaicism) is also seen on CT (B). CT pulmonary angiography (C and D) and MR angiography (E) confirm limited and predominantly distal (arrowhead) segmental and subsegmental disease distribution that was confirmed on selective invasive pulmonary angiography (F—arrow, occluded left posterobasal artery branch (A10)). This patient went on to have balloon pulmonary angioplasty (BPA).
When to refer
All patients with suspected CTEPH should be referred to a CTEPH service that has pulmonary endarterectomy (PEA) and BPA capabilities and hosts the CTEPH multidisciplinary team (MDT). The minimum data set that is required from referring regional PH centres to inform the MDT should include clinical details, the patient’s functional class (FC) and significant comorbidities, a 6 min walk distance (6MWD), lung function test, transthoracic echo report, haemodynamic assessment by right heart catheterisation and anatomic assessment from at least two imaging modalities—CT, MRI or invasive pulmonary angiography.
Treatment selection
The sixth World Symposium on Pulmonary Hypertension (WSPH) proposed a treatment algorithm for the patients with CTEPH (figure 3).9 Patients should receive lifelong vitamin K antagonist (warfarin) on non-vitamin K antagonist oral anticoagulant and then should undergo an MDT assessment, including a surgeon experienced with PEA (ideally performing more than 50 operations per year), PH specialist, BPA interventionist and CTEPH-trained radiologist, to determine the best treatment strategy. Generally, patients with operable CTEPH (surgically accessible, high disease burden without a major contraindication to surgery) should receive PEA as the treatment of choice. For those deemed inoperable (disease burden that fails to justify the risk of major surgery and/or a distribution of disease that is inaccessible), initiating medical therapy and considering BPA is appropriate. Patients with persistent/recurrent symptomatic PH following PEA should receive medical therapy and be considered for BPA or redo endarterectomy. The decision to offer BPA should also take into account clinical, functional, haemodynamic and imaging data (table 1). The available therapies are not necessarily mutually exclusive, and the choice offered will depend on the local expertise available.

Chronic thromboembolic pulmonary hypertension (CTEPH) treatment algorithm.9 #Multidisciplinary: pulmonary endarterectomy surgeon, pulmonary hypertension (PH) expert, BPA interventionist and radiologist. ¶Treatment assessment may differ depending on the level of expertise. +BPA without medical therapy can be considered in selected cases. BPA, balloon pulmonary angioplasty.
Patient selection for BPA
Operable CTEPH
Pulmonary endarterectomy
PEA is the established therapeutic intervention with the most published evidence and is the guideline recommended treatment for patients with CTEPH.9–13 The recommendation is class I for ‘operable’ patients, but the level of evidence is only C as there has never been a randomised controlled trial (RCT).13 However, the guidelines and the sixth WSPH recommendations differentiate operable and non-operable CTEPH, but in clinical practice this distinction is subjective and determined by surgical experience and local practice. Thus ‘operability’ remains the key decision in the assessment of patients with CTEPH, and this should be determined by an experienced MDT.
PEA technique
PEA is however a major surgical procedure involving general anaesthetic, median sternotomy, cardiopulmonary bypass and deep hypothermic circulatory arrest (DHCA).10 14 The DHCA is required to give a completely bloodless field and allow adequate visualisation to perform a complete endarterectomy to clear all obstructive materials (see figure 1). The original technique was popularised by the team from the University of California at San Diego and although the basic technique is relatively unchanged, experienced modern surgeons are able to clear more distal disease at subsegmental level.9 PEA surgery can clear the most proximal laminated thrombus as well as more distal subsegmental webs and occlusions in vessels of 1–2 mm. As with any cardiac surgical procedure, patients require intensive care following surgery and at least a week of hospitalisation and full recovery may take 2–3 months.
Efficacy of PEA
Of the three possible treatments, PEA has the most published evidence for efficacy. In the largest series published to date, mPAP reduced from 45.5 mm Hg before surgery to 26.0 mm Hg after surgery, and PVR fell from 719.0 to 253.4 dyn.s.cm−5.15 The magnitude of this perioperative haemodynamic improvement is similar to that seen in other published surgical series and, unlike the improvement with BPA and drug therapy, is manifest immediately following surgery. In the first international CTEPH registry the 6MWD increased from 362 to 459 m in 386 operated patients.16 In the long-term follow-up of 880 UK patients following PEA, FC (% 1/2/3/4) improved from 0/9/68/23 to 34/47/15/0.17 The latter series is also the largest long-term complete follow-up of patients following PEA surgery and demonstrated a 10-year survival of 72% for an average age of 57 years.17 This series also highlighted that although survival was excellent, residual PH was common with 51% having an mPAP of >25 mm Hg at 6 months following PEA surgery. This emphasises the need for careful follow-up and that some patients may require additional therapy even after surgery.
Safety of PEA
In the original international CTEPH registry, including 386 incident patients operated in 17 centres, in the era 2007–2009, the in-hospital mortality was 4.7%.16 Some perioperative complication was recorded in 49.2% of patients. Most complications are the same as those reported after any major surgical procedure, but specific complications related to PEA surgery include residual PH and right ventricular failure, reperfusion lung injury and airway haemorrhage. In modern practice the latter serious complications can be managed with extracorporeal membrane oxygenation support. In a more recent report from a single specialist centre the in-hospital mortality was 2.2% for the most recent 500 patients.15
Inoperable CTEPH
Medical therapy
Survival at 3 years in unoperated patients is 70% and is not affected by medical therapy, although preliminary data suggest that the soluble guanylate cyclase riociguat may improve medium-term survival.18 PH-targeted medical therapy, using riociguat or the endothelin receptor antagonists bosentan and macitentan, has short to medium-term evidence of haemodynamic, exercise and symptomatic improvement in recent double-blind placebo-controlled clinical trials.19–22 In the Chest-1 Trial mPAP fell by 10% and the PVR by one-third, while 6MWD increased by just over 10% in the riociguat arm and 33% of patients reported a one-grade improvement in FC. The safety and efficacy of riociguat appears to extend beyond 2 years18 22 although longer term mortality benefits have not been demonstrated. These therapies may be used alone or in combination, as well as alternatives (phosphodiesterase inhibitors and prostanoids). However, they do not modify the underlying mechanical thromboembolic/fibrotic obstruction and as a result must be taken lifelong, incurring not insignificant expense, as well as morbidity from side effects in some patients. Therefore, drug therapy in CTEPH is usually only recommended by exclusion if surgical or interventional therapy is not possible or has already been used. To date, the concept of drug bridging therapy prior to interventions remains controversial and although often used in practice, it is not included in the guidelines as there has not been an RCT to prove safety and efficacy.
Balloon pulmonary angioplasty
BPA was first described by Feinstein et al 23 in the USA but it was initially abandoned due to the frequency of major complications and received little attention internationally until the fifth WSPH.24 However, refinement of the technique in Japan and Europe over the past 10 years25 has seen a resurgence in its use for patients with inoperable CTEPH with encouraging results. The 2015 European Society of Cardiology/European Respiratory Society guidelines for the diagnosis and treatment of PH have recommended BPA in patients with CTEPH who are technically inoperable or carry an unfavourable risk-benefit ratio for PEA surgery (recommendation class IIb, level of evidence: C).13
BPA technique
In its simplest form, with the patient awake, femoral or jugular venous sheaths are inserted under local anaesthetic and balloon-mounted catheters (typically 2–4 mm in diameter) are introduced over a guide wire into pulmonary segmental and subsegmental diseased vessels and inflated to unblock them and restore flow, as evidenced by improved lung parenchymal contrast blush and venous return (figure 4). There is no consensus as to the best approach; some advocate focused treatment, limited to lobar segments, with a near 1:1 balloon-to-artery ratio, whereas others are proponents of a more extensive, diffuse treatment strategy initially with much smaller balloons. Intravascular imaging or functional assessment, aiming to achieve a mean distal to proximal arterial pressure ratio (Pd/Pa) >0.80 unless the baseline mPAP is >35 mm Hg, may also be used.26 What is agreed is that serial separate treatments are required, titrated to the prevailing pulmonary haemodynamics (fewer segments treated and/or smaller diameter balloons used and/or limiting Pd when the mPAP is high) to minimise the risk of complications, as well as limiting the amount of contrast and radiation administered per procedure. Typically, a complete treatment course involves four to six separate BPA procedures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pre-BPA: subtotal occlusion (white arrow) of right anterobasal artery (A8) imaged in the left anterior oblique projection. Post-BPA: improvement in subsegmental arterial contrast opacification and lung parenchymal contrast blush (black arrow) as well as pulmonary venous return (arrowhead). BPA, balloon pulmonary angioplasty.
Efficacy of BPA
Meta-analysis of observational data suggests that the effects of BPA may be superior to medical therapy and possibly equivalent to PEA.27 Haemodynamic and symptomatic improvement is not immediate and presumably requires vascular healing to occur. In a systematic review of published longitudinal cohort studies comparing the ‘before’ and ‘after’ effects of BPA treatment delivered in mean of 2.5–6.6 sessions,28 mPAP reduced by around 14.2 mm Hg, PVR by about 300 dyn.s.cm−5 (3.75 WU), the 6MWD was increased by around 67 m and FC fell by over one grade. Right ventricular reverse remodelling with a reduction in N-terminal pro B-type natriuretic peptide has also been reported.29 30 The therapeutic effects of BPA may be affected by the phenotypic differences in those offered BPA; many early BPA studies, particularly from Japan, had proximal surgically operable disease and were not on PH-targeted treatment. Nevertheless, contemporaneous data of patients with inoperable disease from an experienced surgical centre and on PH-targeted medical therapy confirm the persistent efficacy of BPA.30
The first RCT to compare treatment strategies within the CTEPH algorithm, Riociguat Versus Balloon Pulmonary Angioplasty in Non-operable Chronic Thromboembolic Pulmonary Hypertension trial (NCT02634203), has shown that BPA achieves a significantly lower PVR than riociguat, but equivalent exercise capacities were observed.31 In reality, medical therapy and BPA are likely to be complementary—each treating different aspects of the disease process; BPA treating segmental and subsegmental diseases, while medical therapy tackles the microcirculatory vasculopathy that often coexists.
Reassuringly, the effects of BPA appear durable out to 5 years, with restenosis being a rare occurrence.32 33 In addition, data exist to support BPA for broader indications including the treatment of residual disease after PEA34 as well as in patients with chronic thromboembolic disease—chronic thromboembolic lesions but without PH at rest.35
Safety of BPA
BPA is an invasive treatment and is associated with complications which are reported at a rate of approximately 10% of procedures in contemporary practice, although where routine CT follow-up is performed, this value may be higher.25 Determining the precise rate of complications is difficult as reporting varies from study to study and variable definitions have been used. This has necessitated clearer guidance on BPA complication definition to improve and homogenise future reporting by the sixth WSPH.9 A recent systematic review36 has confirmed in contemporary cohorts that mortality is generally below 2%. Mechanical circulatory support was required in 2.4%, endotracheal intubation in 4.6% and non-invasive ventilation in 22.5%. Other complications are generally reported per procedure; haemoptysis (often due to distal wire exit) was reported in 13.5% and lung reperfusion injury (LRI-oedema) in 22%. The former may require prolonged balloon inflation, reversal of anticoagulation or rarely transcatheter gel or coil embolisation, whereas the latter usually settles with supplemental oxygenation, diuretics and time.
LRI may be predicted and possibly avoided by calculating the Pulmonary Edema Prediction Score Index defined as the product of PVR (WU) and the sum change in pulmonary flow.37 A score of less than 35 has a negative predictive value for LRI of 92.3%. Similarly, others have advocated that maintaining the Pd <35 mm Hg downstream of treated lesions achieves the same haemodynamic improvements as BPA without this guidance, but with fewer episodes of LRI.26 A pragmatic approach of delaying treatment of high-risk lesions (occlusions) until the pulmonary pressures have reduced by BPA and adjunctive PH-targeted drug therapy seems a sensible approach to avoid both LRI and haemorrhagic complications.
Future directions
BPA is now sufficiently developed that appropriately powered RCTs comparing PEA versus BPA for segmental and subsegmental (levels 3 and 4) CTEPH could be planned in centres with equivalent experience in both techniques. However, consensus in the interpretation of imaging and standardisation of the surgical and BPA approach between centres will be important to deliver meaningful comparisons. The immediate focus of registries, such as the international CTEPH association BPA registry, should be to guide which endpoints to use and to define what constitutes a ‘good outcome’ for the patients with CTEPH; ideally this will be long-term survival with a good FC and quality of life. Ultimately, the issue of cost-efficacy needs addressing to determine if lifelong PH-targeted drug therapy remains necessary after BPA. It is currently unclear whether BPA alone will prevent disease progression from the associated vasculopathy, or whether ongoing PH-targeted therapy after haemodynamically successful BPA is still necessary. Finally, pulmonary artery denervation may offer further haemodynamic and symptomatic benefits to patients with residual CTEPH (NCT02745106), although its role in the treatment cascade remains to be established and it is not recommended in the current guidelines.
Conclusion
Surgical and interventional techniques have evolved to enable patients with CTEPH to benefit from these complementary therapies. A multidisciplinary approach integrating imaging, haemodynamic and clinical data is necessary to provide optimal CTEPH treatment, targeted to the individual. Some patients with CTEPH are likely to benefit from multimodality therapy, although the exact sequence of interventional and drug therapies remains to be determined and further RCTs are required.
Key messages
A multidisciplinary approach is necessary to select the optimal interventional treatment for patients with chronic thromboembolic pulmonary hypertension (CTEPH).
If the patient has technically operable disease and the risk:benefit ratio is favourable then pulmonary endarterectomy surgery is indicated, as there is published mortality as well as haemodynamic and symptomatic benefits.
Patients with inoperable disease may be considered for pulmonary hypertension-targeted medical therapy and/or balloon pulmonary angioplasty which both have published haemodynamic and symptomatic benefits.
The interventional strategies for CTEPH are likely complimentary and further research is needed to determine the optimal sequence of interventional and drug therapies.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Supplemental material
Footnotes
Contributors SPH and DJ reviewed the literature, wrote and edited the manuscript and are equal contributors. SPH is the guarantor of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; externally peer reviewed.
Data availability statement There are no data in this work
Author note References which include a * are considered to be key references