Article Text

Statistics from Altmetric.com
Clinical introduction
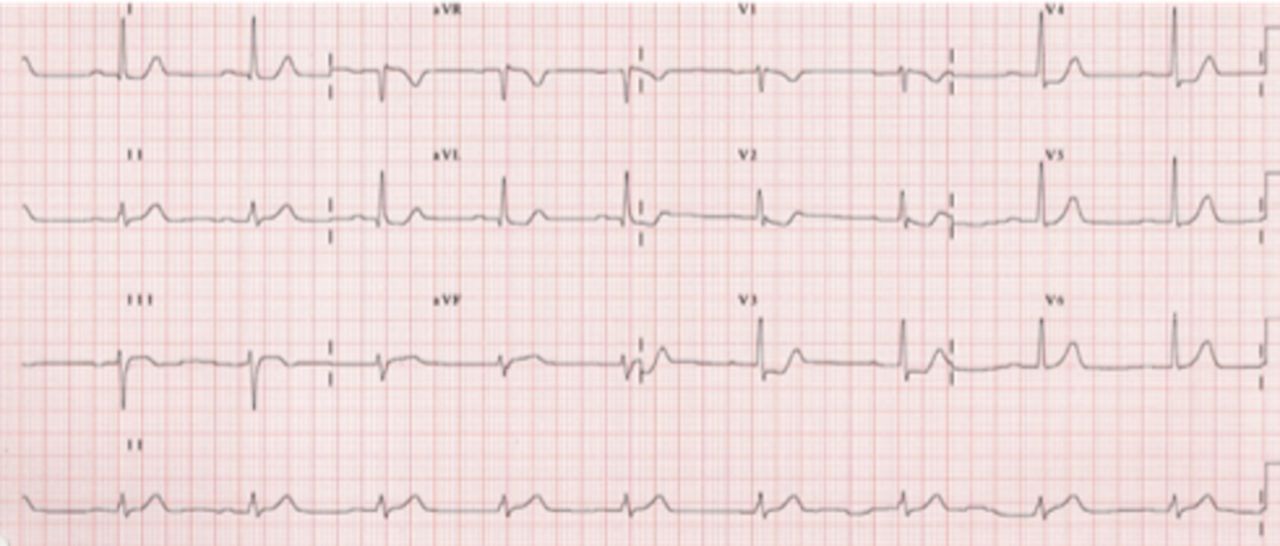
A man in his 70s with previous history of hypertension and dyslipidaemia with diagnosis of posterior myocardial infarction was admitted directly to catheterisation laboratory to perform primary angioplasty (prehospital ECG has sown in figure 1). On arrival, the patient was sweating and lethargic; his blood pressure was 60/45 mm Hg. First invasive pressure tracing was showed in figure 2. The coronary angiography showed total occlusion of obtuse marginal artery in proximal segment (figure 3).

Prehospital 12-lead electrocardiogram showing ST.

Invasive pressure tracing.

Coronary angiography showing total occlusion of obtuse marginal artery.
Question
What to do next?
Emergent pericardiocentesis.
Implantation of intra-aortic balloon counterpulsation.
Start perfusion of glycoprotein IIb/IIIa inhibitors.
Angioplasty of culprit artery.
Discussion
The key to correct diagnosis in this case is a presence of severe hypotension and paradoxus pulse in pressure tracing (figure 2). Echocardiography was immediately performed and revealed a large and dense pericardial effusion suggestive of hemopericardium (answer A).
Left ventricular free wall rupture (LVFWR) is an infrequent complication (<1%) of acute myocardial infarction (MI), but it is associated with a high mortality.1 2 Characteristically, LVFEW occurs in relatively elderly patients, with previous history of hypertension, and in most cases, the MI is the first one recorded, and it is usually transmural. Generally, history of persistent or recurrent chest pain is present and not infrequently these patients experience delay in admission to hospital.1 Echocardiogram should be performed as soon as possible to assess the presence of a pericardial effusion. Once the diagnosis of myocardial rupture is made, management starts with aggressive volume resuscitation, inotropic and vasopressor support and even percutaneous circulatory support. Furthermore, the patient can undergo a surgical repair of the rupture with pericardial patch. A weakened necrotic surrounding myocardium is a weak anchoring site for sutures in surgical repair; consequently, the outcome is poor with mortality rates in the order of 20%–75%.2 3 In this case, the patient was initially stabilised with aggressive colloidal solution infusion and emergent pericardiocentesis and soon after transferred to the operating room. After drainage of bloody fluid, four points of rupture were present at inspection figure 4). A pericardial patch was sutured and glued in place over the tear.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Surgical view of wall rupture after pericardial drainage.
Footnotes
Contributors I approved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.