Article Text

Statistics from Altmetric.com
Much of the last 2 centuries of modern medicine has been spent on eliminating subjectivity in medicine. This concerted effort to minimise clinician and patient subjectivity (and thereby bias) has led to one of the most remarkable breakthroughs of modern medicine—the randomised controlled trials (RCTs). While RCTs are highly effective in evaluating objective findings and ‘hard’ end-points, a similar adjudication of the more subjective endpoints, such as quality of life (QoL), is particularly difficult. This is especially true when testing medical interventions, where placebo effects are difficult to control. Significant efforts have been put in developing techniques and designing trials to reduce these placebo effects.
An erosion of the importance given to patient ‘well being’ and subjective improvement is an unfortunate consequence of this effort, even if an unintended one. However, in the 21st century, this is changing. All across medicine, focus is gradually reshifting towards patient-reported outcomes (PROs) and QoL. This is partly driven by a push from the Institute of Medicine in the early 2000s to incorporate the patient back into the focus of care and partly by market forces as the business of medicine becomes more patient and payer-centric.1 QoL has been defined by the WHO as ‘individuals’ perception of their position in life in the context of culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’.2 In a sense, this encompasses the definition of being human and everything that we value.
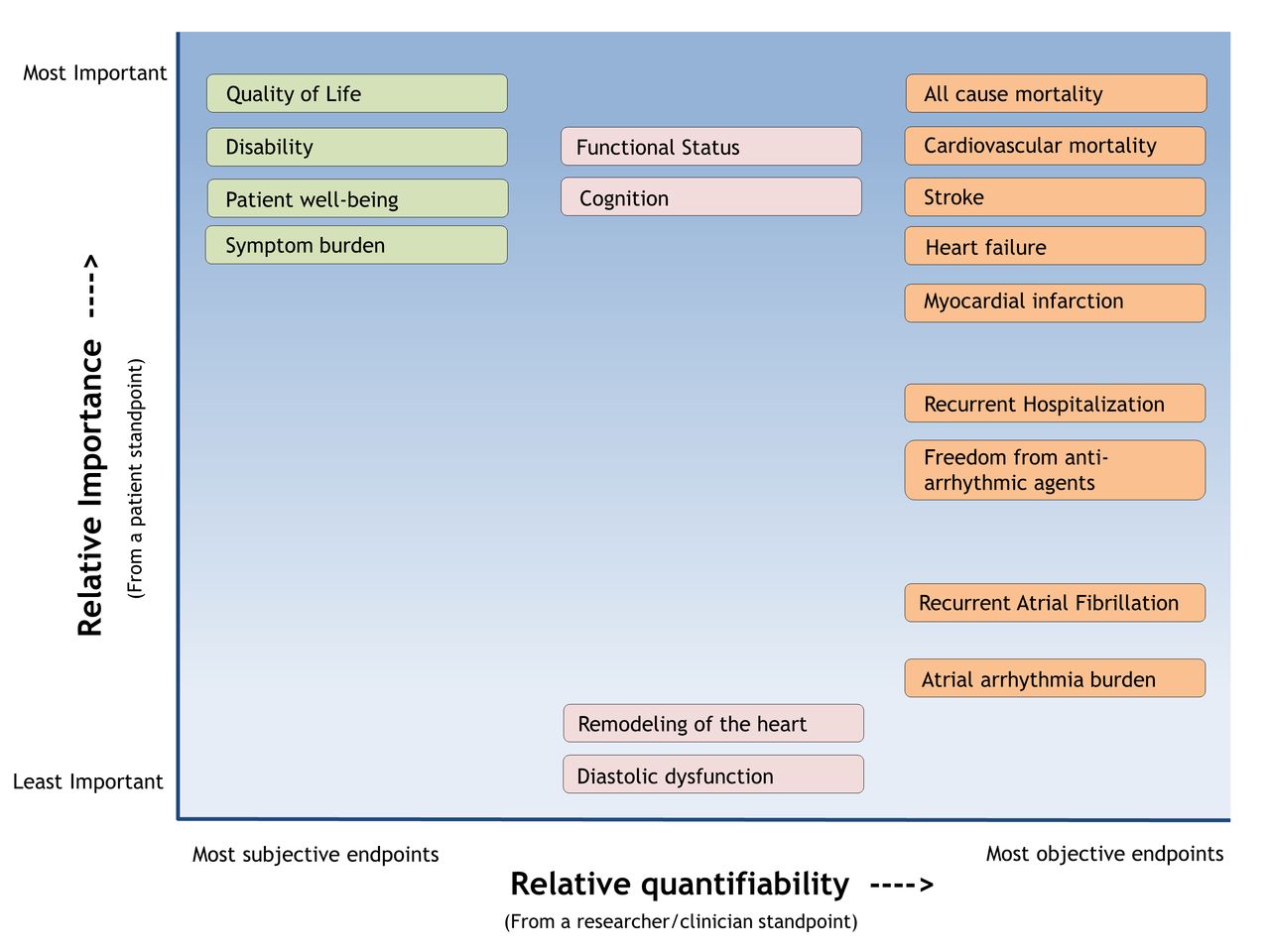
Since atrial fibrillation (AF) ablations were introduced in late 1990s, there have been multiple trials evaluating the outcomes of catheter ablation of AF in comparison to medical therapy (online supplemental table 1). These trials have traditionally evaluated various hard endpoints including mortality, stroke, heart failure, hospitalisations, bleeding, recurrent atrial arrhythmia, arrhythmia burden as well as various combinations of composite hard end-points (figure 1). In the more recent years, trials have also incorporated patient-centric outcomes including functional status, QoL, symptom burden and so on. The majority of the trials have shown a significant reduction in arrhythmia burden with AF ablation compared with alternative therapies but almost none have shown a survival benefit from catheter ablation and/or a decrease in major adverse cardiac events (MACE) (or similar composite end-points). The most consistent finding, however, is that all the trials which have measured patient QoL have shown a significant improvement in this metric (online supplemental table 1).
Supplemental material
{kind=link}
The different outcomes studied in various randomised trials evaluating atrial fibrillation ablation against medical therapy. Shown with relative objectivity on the X axis and relative importance to the patient on the Y axis.
Assessment of symptom improvement, functional capacity and QoL in patients with AF is not straightforward. Patients with AF can present with remarkably varied symptomatology, both in terms of severity and the nature of symptoms. Symptoms include a vague discomfort, an unpleasant awareness of cardiac motion, shortness of breath at rest and/or exertion, fatigue, chest pain, dizziness, lightheadedness, syncope and occasionally a full-blown heart failure from tachycardia mediated cardiomyopathy. QoL is a more comprehensive concept than symptoms alone. QoL in patients with AF can be a complex summation of symptoms, medication side effects, anxiety about the condition of AF and about risks of adverse outcomes, fear of stroke and bleeding, difficulties due to lost days of work, worry regarding the risk of arrhythmia recurrence and future morbid events as well as financial concerns. Due to these concerns, symptoms in AF contribute to, but do not account for all of the QoL impairments associated with AF.
In addition to the above challenges, the assessment of QoL of a patient with AF after catheter ablation is further complicated by multiple procedure-related factors such as procedural anxiety, excessive patient expectations from a ‘complex’ procedure as compared with a ‘simple’ medication, a real risk of procedural complications, procedural failure, placebo effect and the need to repeat procedures.
The International Consortium for Health Outcomes Measurement (ICHOM) has established cognitive functioning, health-related QoL, physical functioning and emotional functioning as important PROs in the management of AF.3 Previously, many AF ablation trials have evaluated QoL in patients with AF using different QoL measures and symptom checklists (online supplemental table 1). In aggregate, these trials comparing patients with AF randomised into medical therapy versus catheter ablation show that QoL improves in the catheter ablation group. However, a few issues remained unanswered—whether these changes in QoL correlate with arrhythmia recurrence and whether functional capacity and cognition, which ultimately are big determinants in a patient’s overall well-being, improve with ablation.
In this issue of Heart, Piccini et al have tried to explore these questions. They investigate the changes to QoL, functional status and cognition in patients after AF ablation in the AXAFA trial, and they evaluate these changes in the context of atrial arrhythmia recurrence.4 They found that improvement in QoL, functional status and cognitive function were greater in those without recurrent AF compared with those with recurrent AF. After adjusting for baseline QoL values and covariables, score improvement was higher for all the measures studied in the group without arrhythmia recurrence at 3 months, but only change in functional status remained statistically significant. In the overall cohort, cognitive function improved slightly after ablation regardless of recurrent AF.
Two important points can be gleaned from this study. First, functional capacity improves after a successful ablation. Functional capacity can be described as one’s maximum potential to perform the activities people do in the normal course of their lives to meet basic needs, fulfil usual roles and maintain their well-being. In essence, QoL reflects an individual’s perception of their functional status and is essentially tied to one-another as an outcome. One reason for the lack of statistical significance of the other QoL measures may have been the shorter follow-up, and it is possible that subsequent visits beyond 3 months will show a further divergence in QoL scores if arrhythmia recurrence rates remain low. Second, cognition appears to improve slightly after ablation, regardless of outcome. This is an important finding given that studies have shown a high prevalence of asymptomatic cerebral emboli after AF catheter ablation.5 MRI studies postablation have raised a concern for cerebral micro-emboli caused by ablation itself, with unclear long-term effects. This study is reassuring in that this risk is unlikely to be clinically significant, although longer follow-up would be required to study the effects on cognition in the long term.
As detailed above, there are multiple factors that add complexity to the assessment of QoL after an interventional procedure. These factors have the potential to bias the QoL assessment in either direction of null and are difficult to control for even in the most carefully designed RCTs. Interventional trials in which the patients are fully unaware of their randomised assignment, such as a sham-controlled RCT, might provide the conclusive answers. However, an adequate sham controlled trial carries various feasibility and ethical concerns and is unlikely to be a reality in the near future.6
Difficulties in measuring QoL and functional status in cardiac interventional trials should not be a deterrent to measuring them; rather, they should be a motivation to develop unified protocols and standards for evaluating PROs in procedure trials. The work of ICHOM AF working group is one such attempt to standardise the measured outcomes.3 We also need RCTs which focus on QoL as primary outcome measures, as opposed to studying QoL as a secondary analysis. To our knowledge, the CAPTAF trial was the only AF ablation trial studying QoL as a primary end-point.7 The CABANA trial studied QoL as a major objective; however, it was still a secondary end-point.8
Cardiology, as a specialty, has historically prioritised evaluating interventions using ‘hard endpoints’ or objectively measurable endpoints such as MACE and survival. This is clearly a very important standard to measure up to, but is that the ultimate goal? Patients come to their doctors with hopes of relieving symptoms and returning to a level of health they find enjoyable. As researchers and clinicians, our goals must align with those of the patients and what they value. It is heartening to see that more and more clinical trials in cardiology and electrophysiology are incorporating PROs as important endpoints. A slow but definite paradigm shift is occurring to incorporate therapies with a focus on improving patients’ lives, not just their hearts.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ArunRSridhar
Contributors AS: concept, manuscript preparation, critical editing. RC: manuscript preparation.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Arrhythmias and sudden death