Article Text

Statistics from Altmetric.com
- Positron emission tomographic (PET) imaging
- echocardiography
- tricuspid valve disease
- cardiac imaging and diagnostics
Clinical introduction
A woman in her 60s was referred for a routine echocardiogram after identification of a systolic murmur by her general practitioner. She was asymptomatic and clinical examination revealed only mild ankle oedema. Medical history included treated hypertension, a right nephrectomy and adrenalectomy 2 years previously for a benign cystic lesion and a 5 cm ovarian cyst under gynaecology surveillance. She had also recently been diagnosed with irritable bowel syndrome (IBS) by gastroenterology.
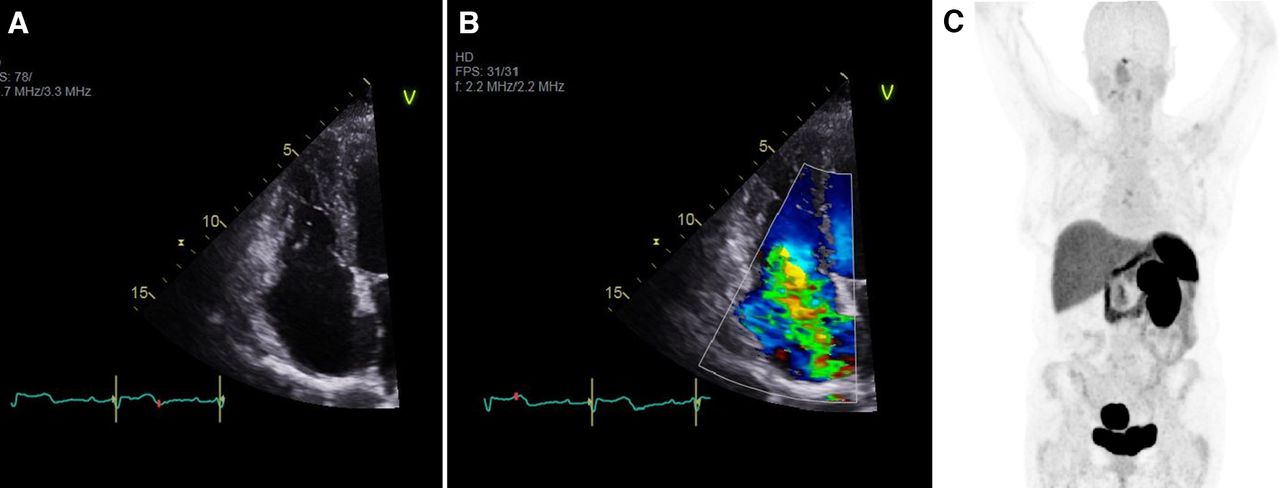
Transthoracic echocardiography demonstrated thickening of the tricuspid valve with severe regurgitation and a pulmonary artery systolic pressure of 55 mm Hg (figure 1). There was also mild to moderate mitral regurgitation and mild left ventricular dysfunction, with an ejection fraction of 50%. She was referred for cardiac MRI, which confirmed severe tricuspid regurgitation and showed no evidence of myocardial fibrosis. She underwent a CT of the thorax abdomen and pelvis, which reported unremarkable appearances of the liver, left kidney, adrenal gland, spleen, pancreas and a 5 cm cystic lesion in the right adnexa. A whole-body positron emission tomography (PET) scan was performed (figure 1).

Transthoracic echocardiogram showing apical four-chamber view of the tricuspid valve (A), with colour Doppler (B). Whole-body positron emission tomography scan (C).
Question
What is the most likely diagnosis?
Paraganglioma.
Carcinoid syndrome.
Hypereosinophilic syndrome.
Tuberculous valvular endocarditis.
Libman-Sacks endocarditis.
Answer
B. Carcinoid syndrome secondary to an ovarian neuroendocrine tumour.
Discussion
A number of extracardiac pathologies involve the valvular apparatus. On further questioning, the patient reported episodic diarrhoea and flushing (previously attributed to IBS). Such symptoms occur in carcinoid syndrome secondary to serotonin release.1 Urinary and hormone analyses revealed raised 5-hydroxyindoleacetic acid, chromogranin A and B, and gastrin. PET demonstrated a 55 mm solid cystic and hypervascular ovarian mass with positive gallium response (figure 2). Primary ovarian neuroendocrine tumours (NETs) have an indolent course, accounting for <1% of all carcinoid tumours and 0.1% of all ovarian neoplasms.2 Unlike classical carcinoid tumours, ovarian NET cause symptoms in the absence of liver metastases as venous drainage bypasses the portal venous system.1

{kind=link}
{kind=link}
Axial CT, PET and fused PET-CT images through the ovarian lesion with cross hairs centred on lesion. PET, positron emission tomography.
Paragangliomas are extra-adrenal pheochromocytomas. Catecholamine secretion leads to paroxysmal episodes of severe hypertension, which can result in acute cardiomyopathy and intestinal symptoms3 but not isolated valve degeneration. Hypereosinophilic syndrome can induce restrictive cardiomyopathy due to eosinophilic infiltration, but rarely isolated valve disease. Tuberculosis (TB) valvular endocarditis is uncommon in immunocompetent individuals and usually only manifests in miliary TB.4 Libman-Sacks endocarditis can occur in patients with systemic lupus erythematosus (SLE), most frequently affecting the mitral valve, but additional SLE sequelae would be expected.5
The patient responded to somatostatin analogue therapy and awaits valve replacement.
Footnotes
Contributors All authors contributed to the idea generation, manuscript production and review. DH was responsible for manuscript submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.