Article Text

Statistics from Altmetric.com
Learning objectives
Why screen for cardiovascular disease?
When is screening justified?
Proposed cardiovascular screening programmes.
The rationale, need and opportunity of multiple screening.
The societal challenge of the ageing population
Although the incidence of cardiovascular disease (CVD) has decreased in recent decades, CVD remains a major healthcare challenge. In Europe alone, CVD causes 3.9 million deaths annually (45% of all deaths), and due to the demographic shift toward a more elderly it will continue to increase its prevalence.1 2 In 2015, almost 49 million Europeans were living with CVD, corresponding to slightly less than 10% of the population. This fact translates into annual losses of 26 million disability-adjusted life years (QALYs) and annual costs to society of approximately €210 billion, half of which is in healthcare costs.1
Remarkably, 80% of cardiac events and strokes are preventable and 25%–75% of these are through early detection and intervention.1 3 Therefore, strategies to prevent ischaemic events offer some of the greatest potential for improving public health. The uniform natural history and prevention of manifest atherosclerosis provides the possibility for much larger benefits than seen in cancer screening programmes due to the initiation of uniform cardiovascular preventive actions, when localised lesions are detected—also protects unidentified remote lesions.4–9 Thus, the development of new proposals for screening approaches is rapidly evolving, and influential bodies such as the US Preventive Services Task Force (USPSTF) and the UK National Screening Committee (UK NSC) have evaluated a number of proposals for cardiovascular screening and, as a result, currently recommend screening for a variety of individual conditions.
Prevention of cardiovascular atherosclerotic disease
Primary prevention
Primary prevention is the intervention against the modifiable risk factors of ischaemic events. Global risk scores such as the SCORE are recommended to combine individual risk factors into a single quantitative risk estimate.10–12
In Europe and USA, individuals with a 10-year risk of CVD death ≥5% qualify for lifestyle intervention and, when CVD death risk is ≥10%, drug treatment is frequently recommended. However, guideline-based recommendations for individuals ≥70 years are lacking despite the fact that >80% of CVD deaths occur in this age group.13 14
Nevertheless, population-based screening and intervention based on clinical risk scores does not reduce all causes or cardiovascular mortality.15 16 Although these trials were performed before or in the beginning of modern cardiovascular preventive treatment with statins, the conclusion from these trials was that screening was not needed due to the quality of the general practitioners. Thus, these studies do not address the potential of modern-day screening in primary prevention. Finally, the majority of these studies were in those aged <60 years, and the Cochrane review excluded studies targeting older patients, and from our point of view, those are the most relevant for in lesion-based pharmacological preventive strategy.15 16
Secondary prevention
Secondary prevention entails interventions that are specifically targeted against lesions, which can cause ischaemic events (eg, due to type IV lesions). Secondary prevention techniques require the visualisation of asymptomatic lesions whether by opportunistic, chance-based detection or by systematic screening. The rationale for screening has been discussed intensively.17 18 Overall, ultrasound-based screening for abdominal aortic aneurysm (AAA) of men has been found to reduce mortality in a cost-effective manner,19 although similar evidence supporting screening for CVD is lacking.12 13 20
Tertiary prevention
Tertiary prevention includes preventive actions that are taken to prevent new events after symptomatic disease, such as antithrombotic treatment after coronary revascularisation. Such preventative approaches are beyond the scope of this educational article.
Definition of screening
The idea of screening is more than 150 years old. Early in the twentieth century, screening for tuberculosis and syphilis was initiated, and the popularity of screening has grown ever since.21 22
WHO defines screening as the identification of unrecognised disease in an apparently healthy, asymptomatic population, by tools that can be applied rapidly and easily to the target population.21 22
Opportunistic screening
Opportunistic screening occurs when individuals, healthcare providers or the healthcare system take initiative to check for health conditions on an ad hoc basis, typically because of suspected risk. Unlike systematic, population-based screening, opportunistic screening is often not centrally managed, and thus has the advantage of little to no cost in regard to administration. The disadvantage is that the benefits and harms are usually unclear and not evaluated according to the same criteria that are used for systematic and centrally organised screening. A further issue is social inequality in regard to access to healthcare, because the initiative, at least at the first step of the process, is placed on the individual. As a result, if more informed, resourceful individuals are more likely to suspect and act on their risk, then opportunistic screening might lead to increased inequality in health, in addition to the overall, inferior effect of screening because individuals in the highest-risk category might not be reached at all.
Population-based screening
In population-based, systematic, screening programmes, everyone in the target population is invited. This implies the testing of asymptomatic, apparently healthy people, of which the majority will only be exposed to the negative effects of screening to identify the few who will enjoy a health benefit. Such screening is thus a distinct and complex public health strategy that requires additional resources, coordination and infrastructure. Consequently, a screening programme should be implemented only when its effectiveness has been proved; when human, financial and physical resources are present to cover nearly all the target groups; when facilities exist for the follow-up of abnormal results to confirm diagnoses and ensure treatment, as well as when the prevalence/health consequences of the disease are high enough to justify the efforts and costs of screening.22
In 1968, Wilson and Jungner proposed a number of still core criteria that should be satisfied for screening to be justified22 (table 1). In general, the condition for which the screening programme will be established must be an important health problem that can be detected and treated in an acceptable way for the target population, at costs that are reasonable.
The Wilson and Jungner criteria from 1968 that must be satisfied for screening to be justified
In addition, according to WHO, a screening programme should entail21:
Algorithms for systematic invitation and follow-up for screening positives.
Participation rate ≥70% of the target population.
Sufficient infrastructure and resources to offer the test and to adequately diagnose and treat those found to have the disease.
Robust monitoring and evaluation framework to assure quality.
It should be noted that successful models from high-resource countries with advanced healthcare systems may not be adaptive to countries without the needed infrastructure and resources to cover the population. Ideology and policies on screening may differ significantly between countries due to culture, disease pattern, and healthcare organisation and finance. As a result, there is no one-size-fits-all approach, and local adaptations are typically needed.
Assessment of the benefits and harms of screening
In many countries, national boards evaluate existing and proposed screening programmes, and some boards now recognise a need for further and more detailed criteria. In particular, regarding the balance between benefits and harms. Four current and former members of the USPSTF profoundly discussed this aspect and refer to the key concept of a net benefit, which includes the benefits of screening subtracted the harms23 (table 2). In general, there are four sources of harms, which must be quantified to estimate the net benefit:
The psychological consequences to quality of life (Qol) when individuals are made aware of risk, because of an invitation to screening and will not have certainty before the test result is known. This may not be a large harm, and the period of influence is limited, but the number of people affected is large.
False positives impact Qol due to anxiety and concern, and further diagnostic evaluation and surveillance may cause physical harms.
Overdiagnosis and its consequences due to unneeded treatment. True positives for whom the detection and following preventive intervention will not change their life course.24 However, because there is no way to predict the exact outcome for a specific person, the dilemma is that to reduce overdiagnosis, by, for example, lowering the indication threshold for preventive measures, the health benefit to those who are rightfully diagnosed is also reduced. Overdiagnosis may affect a person both physically and mentally for the rest of his or her lifetime.
Physical and psychological disutility related to the confirmatory testing and preventive intervention of the rightfully, true-positive diagnosed individuals.
Considerations for estimating the benefits and harms of a screening programme, modified from Harris, Sawaya, Mover and Calonge23
These harms must be estimated through randomised, controlled trials (RCTs) designed to deliver the evidence and/or systematic reviews, ideally expressed as loss of QALYs, which allow for quantification of the net benefit in one measure. To estimate the net benefit, these QALYs must be subtracted from the QALYs gained by the benefits of the screening and must be expressed as absolute effects as well as relative effects.
Value proposition of screening to society
The Wilson-Jungner criterion regarding the benefits of a screening programme being ‘economically balanced in relation to possible expenditure’ (table 1) remains another pivotal element of decision-making with regard to screening.22 Since 1968, methods such as cost-effectiveness and cost utility evaluations that incorporate and synthesise evidence concerning the net benefit against the total costs from a healthcare, or even a societal, perspective have evolved and become an obligatory part of assessments by, for example, the USPSTF or the UK NSC. These methods essentially assess the additional cost required to achieve additional value, which can be compared with the equivalent cost of value gains elsewhere in healthcare, or even in society, to inform priority setting. If prevention is to be judged on similar terms as other healthcare activities (when competing for funding), then this evidence is necessary to prioritise according to the value obtained for the money spent.
In societies where equity is a key concern, the value-for-money perspective should be supplemented by the distributional consequences, that is, not only is it important whether screening offers a mean additional benefit but also who receives this benefit—or in other words, whether screening exacerbates health inequality.25 Although this is not a formal assessment criterion, it is often considered by both the USPSTF and the UK NSC in practice. More recently, methods to directly assess the citizens’ preferences for screening based on information concerning benefits and harms have been proposed for consistency with the idea of value-based healthcare.26
Evaluated cardiovascular population-based screening programmes
The topics evaluated by the USPSTF and/or the UK NSC are listed in table 3 with their associated recommendations. Evaluations have mainly been focused on CVD risk factors, which is essentially different from the early detection of asymptomatic CVD by screening. However, USPSTF evaluated whether atherosclerotic surrogate markers would be useful but concluded that the current evidence is insufficient to support supplementing the traditional risk assessment for CVD by the addition of the ankle–brachial index (ABI), high-sensitivity C reactive protein level or coronary artery calcium (CAC) score. Screening of asymptomatic CVD has only been evaluated regarding atrial fibrillation (AF) and AAA.
USPSTF: https://www.uspreventiveservicestaskforce.org/BrowseRec/IndexUK
NSC: https://legacyscreening.phe.org.uk/screening-recommendations.php
Cardiovascular screening programmes evaluated by the US Preventive Service Task Force (USPSTF) and/or the UK National Screening Committee (UK NSC)
Hypertension
The USPSTF recommends annual screening for adults ≥40 years of age or who are at increased risk for high blood pressure (overweight or obese, and African-Americans). Adults between 18 and 39 years of age with normal blood pressure (<130/85 mm Hg) who do not have other risk factors should be screened every 3 to 5 years.
The evidence behind the recommendation is moderate-quality to high-quality RCTs, which have shown that the treatment of individuals ≥60 years of age toward a target blood pressure of 150/90 mm Hg reduces the incidence of stroke, heart failure and coronary heart disease events.27 Similarly, RCTs have demonstrated the efficacy of the treatment of younger adults to a target diastolic blood pressure of less than 90 mm Hg in reducing cerebrovascular events, heart failure and overall mortality.27
Diabetes
Population-based screening for diabetes is controversial. In the USA, this approach is recommended in asymptomatic adults every third year, if the sustained blood pressure is greater than 135/80 mm Hg. In the UK, it is not recommended due to insufficient evidence.28 29
The USPSTF found sufficient evidence that in adults who have hypertension and diabetes, lowering of the individual’s blood pressure below conventional target values reduces the incidence of cardiovascular events and cardiovascular mortality.
Dyslipidaemia
Although statin therapy is recommended for manifest CVD, nonetheless this treatment approach is more controversial as primary prevention. The USPSTF found level A evidence that men ≥35 years of age and women ≥45 years of age who are at increased risk for coronary heart disease ought to be screened for lipid disorders every fifth year. Population-based screening for familiar hypercholesterolaemia is neither recommended in the UK nor in the USA.
Risk of CVD assessment
In many countries, including the UK and the USA, as well as in the European Society for Cardiology,12 13 it is recommended that individuals ≥40 years of age have their CVD risk reviewed on a regular basis by means of assessment tools such as the SCORE or the QRISK2. Such risk assessments include the measurement of blood pressure and lipids.30 31
Atrial fibrillation
Screening for AF has been the subject of much debate due to the increasing prevalence of AF-related stroke and the potential to prevent this condition with appropriate anticoagulation. In a cohort study of 5555 asymptomatic patients with AF or with incidentally detected AF, antithrombotic therapy was compared with no antithrombotic therapy, showing an absolute 3% reduced risk of both stroke and death within 1.5 years.32 Several cost-effectiveness analyses have been published, which conclude that AF screening is cost-effective. Unfortunately, all these studies rely on critical assumptions regarding the natural history of AF as well as the treatment effect, which has yet to be established in a randomised setting. Several ongoing RCTs are currently underway internationally, the results of which will inform the effect of AF screening.
Abdominal aortic aneurysms
A meta-analysis of four randomised trials showed that screening halves the mortality from AAA and reduces total mortality by 1%–2%.33–35 One of the most recent health economic studies concluded that it is highly cost-effective to screen 65-year-old Danish men for AAA, as a QALY can be gained for approximately Danish Krone 5000 (£550/US$750).36 37 This cost is less than one-tenth of a QALY gained by colorectal cancer screening.38
Consequently, the USPSTF and the UK NSC recommend a one-time screening of men at the age of 65 years; in the USA, however, this screening is restricted to prior and current smokers. National screening programmes have been implemented in Sweden, England, Scotland, Wales, Northern Ireland, Ireland, the USA and Germany.
Coronary artery calcification
Solitary screening for coronary artery calcification using none-contrast CT (nCT) scanning have been suggested by many including recommendations in current guidelines weighing the non-trial evidence of improved risk prediction and could be used for opportunistic screening, but when considered by the USPSTF for systematic screening, they found the evidence of the balance between benefits and harms insufficient (table 3). The only way to clarify would be by randomised trials, but after the NLST and NELSON trials of screening lung cancer have proved its benefits, it is unlikely to be ethically acceptable only to examine the heart in a CT scan. Screening and treatment of increased CAC carries a risk of harm regarding screening-induced cancers by radiation, psychological distress, muscle pain by statins and intracerebral bleeding by antiplatelets. Consequently, RCTs are needed.
Multiple (or multiphasic) cardiovascular screening
In 1968, Wilson and Jungner defined the term multiple screening. ‘This procedure has evolved by combining single screening tests and is the logical corollary of mass screening. Where much time and effort has been spent by a population in attending for a single test, it is natural to consider the economy of offering other tests at the same time. Multiple (or multiphasic) screening has been defined as “the application of two or more screening tests in combination to large groups of people”’.22
Many of the proposed CVD topics for screening are unsupported by evidence derived from RCTs. Solitary screening trials must often be very large, and thus it is expensive to achieve the required statistical power to demonstrate relevant benefits, especially if the prevalence is small. Even if such trials were conducted and solitary screening were proven beneficial, solitary screening offers would remain unlikely because they could be combined to prevent multiple appointments, disutility and costs to participants and healthcare. In addition, combined offers may prove to be both effective and cost-effective overall, even if solitary programmes provide only marginal benefits. Thus, from a public health point of view, multiple CVD screening approaches seem attractive despite the academic challenge of establishing evidence for each of the individual components.
The Viborg Vascular (VIVA) screening trial
The first trial that testing multifaceted CVD screening was the Danish VIVA trial, which combined screening for AAA (by ultrasound scanning), peripheral artery disease (PAD) and hypertension (by measurement of ABI). More than 50 000 men aged 65–74 years were randomised 1:1. After 5 years, overall mortality was significantly reduced by 7%.37 The consequences to Qol were followed both overall and for individuals who tested positive, with no significant harm detected. The costs of an additional life year or QALY was well within what is considered acceptable, at approximately one-tenth of the cost of many cancer screening programmes.38
The VIVA study represents the first time that a reduction in overall mortality by a population-based screening offer has been demonstrated in a single trial. Thus, there is obvious academic interest in disentangling the effect of the three combined screening tests. In the UK, where screening for AAA is already implemented on a national scale, plans to inform this line of inquiry are already in place, where it has been suggested to randomise individuals who have already been invited to abdominal aortic screenings into groups that would or would not have supplementary ABI measurements.
The Danish Cardiovascular (DANCAVAS) screening trial
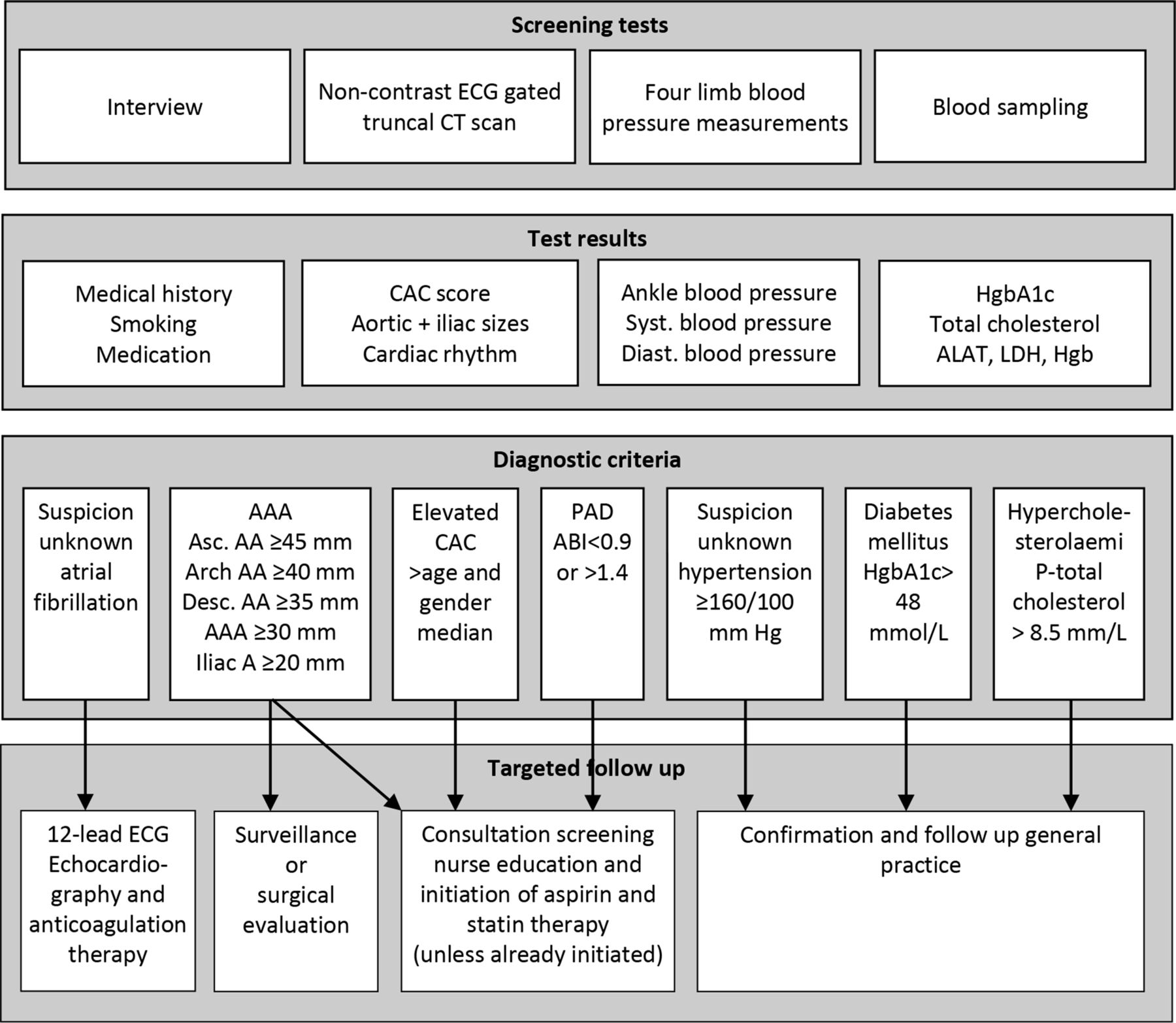
The most recent and sophisticated proposal for multiple CVD screening is another Danish trial, the DANCAVAS trial, in which nearly 50 000 men aged 65–74 years were randomised 1:2. The screening test included: (1) low-dose nCT scanning to detect and quantify CAC score and aortic/iliac aneurysms; (2) AF; (3) brachial and ankle blood pressure measurements to detect PAD and hypertension and (4) blood levels of cholesterol and haemoglobin A1c to detect diabetes and hypercholesterolaemia. Web-based self-booking and data management was used to enhance participant flexibility and to reduce the administrative burden. The complex digitalised algorithm used in this study is illustrated in figure 1, which includes the number of positive findings. In total, more than one-third of all screened initiated preventive medication (statins, aspirin, antidiabetics and anticoagulants) excluding hypertensives. The direct costs for screening and handling of the results were €80 per invited.39
{kind=link}
Flow chart of the DANCAVAS trial illustrating that complex multiple CVD screening is feasible with use of modern digital solutions. AAA, abdominal aortic aneurysm; ABI, ankle–brachial index; ALAT,alanineaminotransferase; Asc,ascending; CAC, coronary artery calcium; CVD, cardiovascular disease; DANCAVAS,Danish Cardiovascular; Diast., diastolic; Desc, descending; HgbA1c, haemoglobin A1c; LDH, lactatedehydrogenase; PAD, peripheral arterial disease; Syst, systolic.
Thus far, the trial shows that complex multiple cardiovascular general population-based screening programmes are feasible and that the programme cost is moderate relative to the health benefit potential. Only 3%–4% initiated similar prevention in the VIVA trial, which nonetheless demonstrated a relative reduction in overall mortality by 7%, and the DANCAVAS proposal provides a potential breakthrough for improving public health and life expectancy in men.
Summary
Ischaemic events in the brain, heart and legs remain among the top causes of death and disability, yet the current preventive efforts largely ignore screening as a public health strategy. The inter-relatedness and uniform pathogenesis of CVDs present opportunities for screening that are distinctly different from prior findings, for example, cancer. Screening for more than one condition spares the participant time, effort and possibly anxiety, while possibly enhancing the efficiency and cost-effectiveness of the system. However, such approaches represent complex public health strategies in which complex criteria should be satisfied before screening is legitimised. 21–24 28 29
Key messages
Cardiovascular disease remains a top cause of death and disability, and although its incidence is declining, nonetheless its prevalence is expected to increase because of the fraction of ageing adults in the population.
Influential bodies such as the US Preventive Services Task Force and the UK National Screening Committee have evaluated a number of proposals for cardiovascular screening and, as a result, recommend screening for abdominal aortic aneurysm, type 2 diabetes, hypertension and dyslipidaemia in selected target groups.
The inter-relatedness yet uniform pathogenesis of cardiovascular diseases present opportunities for screening that are distinctly different from what is known for, for example, cancer.
Combined screening for more than one condition because the indicated interventions in case of positive findings overlap may be overall more effective and cost-effective than conducting multiple individual screening programmes.
The most recent proposition for combined screening includes screening for coronary artery disease, aortic/iliac aneurysms, peripheral artery disease, hypertension, diabetes and hypercholesterolaemia.
Combined screening challenges the academic interest in individual causal links between test and outcome but is actually a targeted public health decision-making strategy in which a causal link between decision and outcome is required.
CME credits for Education in Heart
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the ‘Take the Test’ link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Data availability statement
There are no data in this work
References
Footnotes
Contributors Both authors contributed equally to this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.
Author note References which include a * are considered to be key references.