Article Text

Statistics from Altmetric.com
Despite advances in prevention and treatment of cardiovascular disease, sudden cardiac death (SCD) remains a major public health issue with profound impact on total and premature mortality. SCD is responsible for almost 15% of all cardiac deaths as well as for 40%–50% of years of potential life lost from heart disease, exceeding the respective premature death burden of all individual cancers and most other leading causes of death.1 What is often unappreciated is that the sudden loss of a loved one also poses an unprecedented psychological burden on the victim’s family and friends, leading to anxiety, prolonged grief and even post-traumatic stress symptoms.
SCD is defined as a non-traumatic, unexpected fatal event occurring within 1 hour of symptom onset in an apparently healthy subject, while if death is unwitnessed, the victim must have been in good health 24 hours before the event. Its diagnosis is challenging due to inherent caveats in case ascertainment. The availability of sufficient clinical information to determine the mode and timing of death is important for a valid documentation of SCD and for calculating the respective incidence accurately. In most studies, determination of SCD is based on death certificate data where subjects, having died out of hospital environment, are classified under specific diagnostic codes from the International Classification of Diseases. This methodology, however, results in overestimation of SCD incidence due to inaccuracies in death certificate diagnoses.2 3
Ågesen et al 4 have evaluated the incidence, sex differences and temporal trends of SCD in a longitudinal community-based cohort in Copenhagen with a follow-up of 23 years. The authors should be congratulated for their meticulous analysis of information from multiple sources to achieve rigorous adjudication of the cause of death. SCD documentation was based not only on retrospective assessment of death certificates but also on data retrieved from registered inpatient activity and outpatient visits, medical records and autopsy reports. Additional information was also derived from a specific supplementary field available in Danish death certificates expanding on the circumstances of death. This methodology of case ascertainment increases the credibility of the reported findings.
On the other hand, pertinent limitations need to be commented. Autopsy was considerably underused despite the fact that it remains the most accurate method of determining the cause of death and in half of cases produces findings unsuspected before death.5 In addition, almost 60% of enrolled cases in this study were defined as ‘possible SCD’ due to inability to demonstrate that the person was seen alive and functioning normally within the last 24 hours before being found dead. Therefore, one could assume that a proportion of those ‘possible’ cases might not satisfy the timing criteria for SCD definition, resulting in erroneous classification and overestimation of SCD incidence. Furthermore, the possibility of sampling bias due to non-response may have affected the external validity of the reported results.
SCD: we need to do better
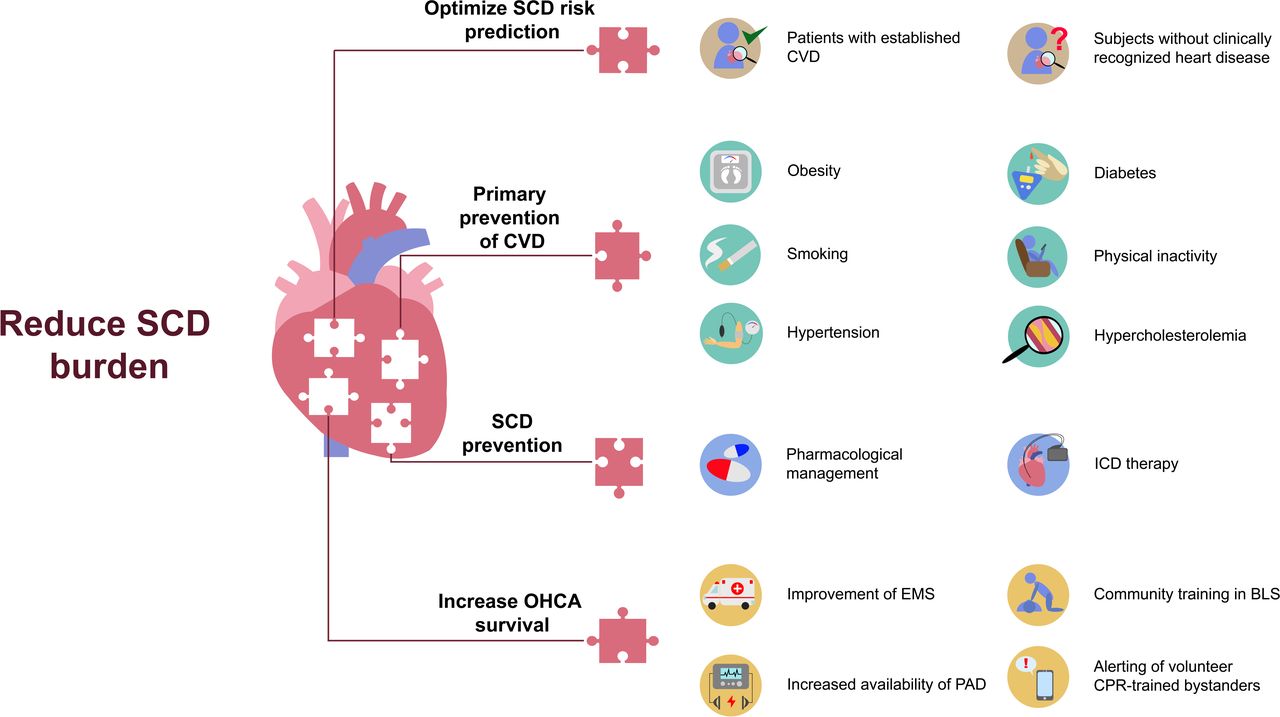
The key finding of Ågesen et al is that the incidence of SCD has decreased significantly over a 23-year period by 41% in individuals aged 40–90 years. This is in line with other data from retrospective cohort studies supporting a decreasing trend in SCD incidence.6 However, SCD still remains a leading cause of death, and the reduction of its burden should be set as a first-line goal of public health practice and policy. The complexity of this task and the diversity of contributing factors stress the need for multifaceted actions (figure 1).
{kind=link}
Priority areas and relevant actions needed to reduce the burden of SCD. BLS, basic life support, CPR, cardiopulmonary resuscitation, CVD, cardiovascular disease, EMS, emergency medical service, ICD, implantable cardioverter defibrillator, OHCA, out-of-hospital cardiac arrest, PAD, public access defibrillator, SCD, sudden cardiac death.
SCD risk prediction needs to be improved in order to accurately identify high-risk subgroups and subsequently enable focused interventions that will prevent SCD. Identification of novel risk markers from different fields (clinical, biomarkers, imaging and genetic) and their integration in stratification schemas and risk scores should be a priority not only in patients with established cardiovascular disease but also, and most importantly, in subjects without clinically recognised heart disease comprising the base of the risk pyramid. In this context, machine learning (ML) can prove useful in the development of novel prediction modelling tools due to its ability to identify predictive patterns from large datasets, including multiple, even heterogeneous variables without predefined associations. In the future, ML-based algorithms could be implemented through electronic health records for risk stratification and event prediction in everyday clinical practice.
Further actions should aim to reduce the rate of SCD by focusing on two priority areas. The first one is prevention of cardiovascular disease by promoting the adoption of healthy lifestyle and behavioural habits and by implementing comprehensive intervention programmes to tackle cardiovascular risk factors. The second priority area is primary and secondary prevention of SCD. This can be achieved by increasing the use and maximising the dosage of pharmacological agents that reduce the SCD rate. Over the last two decades, the SCD rate in patients with heart failure with reduced ejection fraction exhibited a significant decline which paralleled the increasing use of guideline-recommended pharmacotherapies.7 In addition to pharmacological treatment, implantable cardioverter defibrillators are essential for secondary prevention of SCD and can also provide survival benefit, in terms of primary SCD prevention, in specific patient subgroups.
Finally, focus should be placed on improving the survival of patients experiencing out-of-hospital cardiac arrest (OHCA). The performance of emergency medical systems (EMS) needs to be improved, because shortening of ambulance response time is associated with increased survival after OHCA.8 Prompt implementation of resuscitative interventions by bystanders, even before EMS arrival, has also been shown to improve postdischarge neurological status and to reduce mortality of patients with OHCA. Therefore, basic life support training should be promoted in the community, and public access defibrillators should be widely available for use by trained laypersons. Furthermore, mobile phone-based alerting of cardiopulmonary resuscitation trained volunteers, located within a small distance from OHCA victims, should be promoted to reduce resuscitation-free interval and to improve patient outcome.9
Epidemiological surveillance of SCD
The reported absolute values of SCD incidence differ substantially. Ågesen et al found that the standardised incidence rate for SCD in persons aged 40–90 years has fallen to a value of 237 per 100 000 person-years, while the respective value in patients aged 35–74 years in Canada was 42.4 per 100 000 person-years.6 The variability in the reported SCD incidence is attributed to multiple differences in case definition, ascertainment methods, study populations and autopsy rates. Therefore, we are in need of high-quality surveillance systems of SCD that will bridge this ‘epidemiological gap’ and confer multiple benefits such as
Collection, analysis and interpretation of accurate data on SCD incidence.
Assessment of the need for interventions with potential focus on targeted subpopulations (eg, low-risk subgroups, specific age groups, races or ethnicities).
Evidence-based decision making on development and implementation of preventive strategies.
Targeted allocation of healthcare resources.
Availability of performance metrics to appraise the efficacy of implemented measures.
Therefore, healthcare policy makers and planners should prioritise the evaluation of SCD incidence through prospective large-scale population studies or even national surveillance systems using standardised definitions and methodology.
At the end of the day, we should keep in mind that…
What gets measured, gets managed.
Ethics statements
Footnotes
Contributors ST drafted and wrote the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Arrhythmias and sudden death