Article Text

Statistics from Altmetric.com
According to the United Nations High Commissioner for Refugees (UNHCR), there are more than 80 million forcibly displaced persons worldwide as of 2020. This number creates numerous challenges, including the management of patients with chronic cardiovascular disease (CVD) and the associated complications. Despite recognition of the health disparities and policy mandates by the US government to slowly eliminate these barriers, the refugee, immigrant and migrant (RIM) communities continue to experience poor access to preventive healthcare. An analysis of the 2010–2016 US National Health Interview Survey found that RIMs from South America and the Asian and African continents were disproportionately affected by risk factors for CVD, such as hypertension (HTN), diabetes mellitus (DM) and hyperlipidaemia (HLD), compared with their European counterparts. The study found that the highest multivariable adjusted prevalence of diagnosed HTN was 23.5% in Southeast Asian immigrants and for DM the prevalence was measured to be 9.6% among immigrants from Mexico, Central America and the Caribbean. In contrast, the prevalence of HTN was measured to be 22.4% and DM was 6.6% among the European cohort.1 Understanding the unique risk factors in conjunction with addressing the physical, mental and psychological burden of RIMs is imperative in creating comprehensive changes that can be implemented to decrease the disparities within this community.
Per the UNHCR, a forcibly displaced person, which falls within the category of RIM, is a person that ‘has been forced to flee his or her country because of persecution, war, or violence’. These factors can impact their ability to obtain healthcare in their new country of residence. A study conducted on RIM’s access to healthcare demonstrated this population has inadequate access to primary care and preventive services as a consequence of a constellation of social determinants of health, including low-income status, lack of insurance, racial and ethnic background, and/or limited or no English proficiency.2 Compared with those born in the USA, immigrants are more likely to be unaware of their CVD risk factors, causing them to be less motivated to seek treatment and modify their behaviour to prevent negative outcomes. With a sample size of 12 124, the per cent prevalence of HTN and HLD among foreign-born, non-English-speaking participants unaware of their condition was determined to be 36.0% and 48.1%, respectively. In comparison, those same medical diseases had a per cent prevalence of 24.9% and 30.5%, respectively, for those born in the USA.3 These factors, combined with a decreased ability to embrace the utility of preventive care, disadvantage RIMs and increase their risk of developing chronic diseases.
The WHO describes CVD as the leading cause of death worldwide, accounting for 31% of the total disease burden. RIMs carry a higher burden than other groups aggravated by other circumstances, such as torture, exposure to human rights violations, persecution and the stress of acculturation after resettlement into a new country. A study of Syrian RIMs being treated in Jordanian hospitals revealed that chronic war-related stressors and traumatic events significantly contributed to the development and severity of myocardial infarction and coronary artery disease.4 The association emphasises the vulnerability of a population living through severe stress and trauma.
Language barriers pose a significant challenge in the creation of a patient–physician relationship. The inability to establish/maintain a formal relationship, compounded by varying levels of health literacy, decreases compliance among RIMs. A descriptive cross-sectional survey that evaluated CVD among Syrian RIMs found that out of 514 patients with atherosclerotic cardiovascular disease (ASCVD), the lack of follow-up with primary healthcare providers was prevalent and overall adherence to drug therapy was suboptimal. In the study, the most commonly cited cause of patients not taking medication as prescribed was ‘did not understand prescription’.5 In RIMs at risk or having already developed ASCVD, these medications can include antihypertensives, diabetic and antilipidaemic medications.
On resettlement in the USA for example, RIMs slowly integrate into the culture of their surroundings, ranging from changes in diet to daily activities of living. The more sedentary Western lifestyle along with RIM’s unequal access to healthcare increases the development of CVD in these communities. In conjunction with the constrained physician–patient relationships, language and cultural barriers, and a refugee patient’s lack of health literacy and/or knowledge of what they are being told, the need for CVD prevention is urgent to improve health outcomes for RIM populations. A study to assess the efficacy of secondary prevention programmes on behavioural risk factors demonstrated that physical activity, diet modifications, and decreased smoking or alcohol consumption brought about positive change at a community level and provided beneficial effects on RIM’s blood pressure, total cholesterol and mental health.6
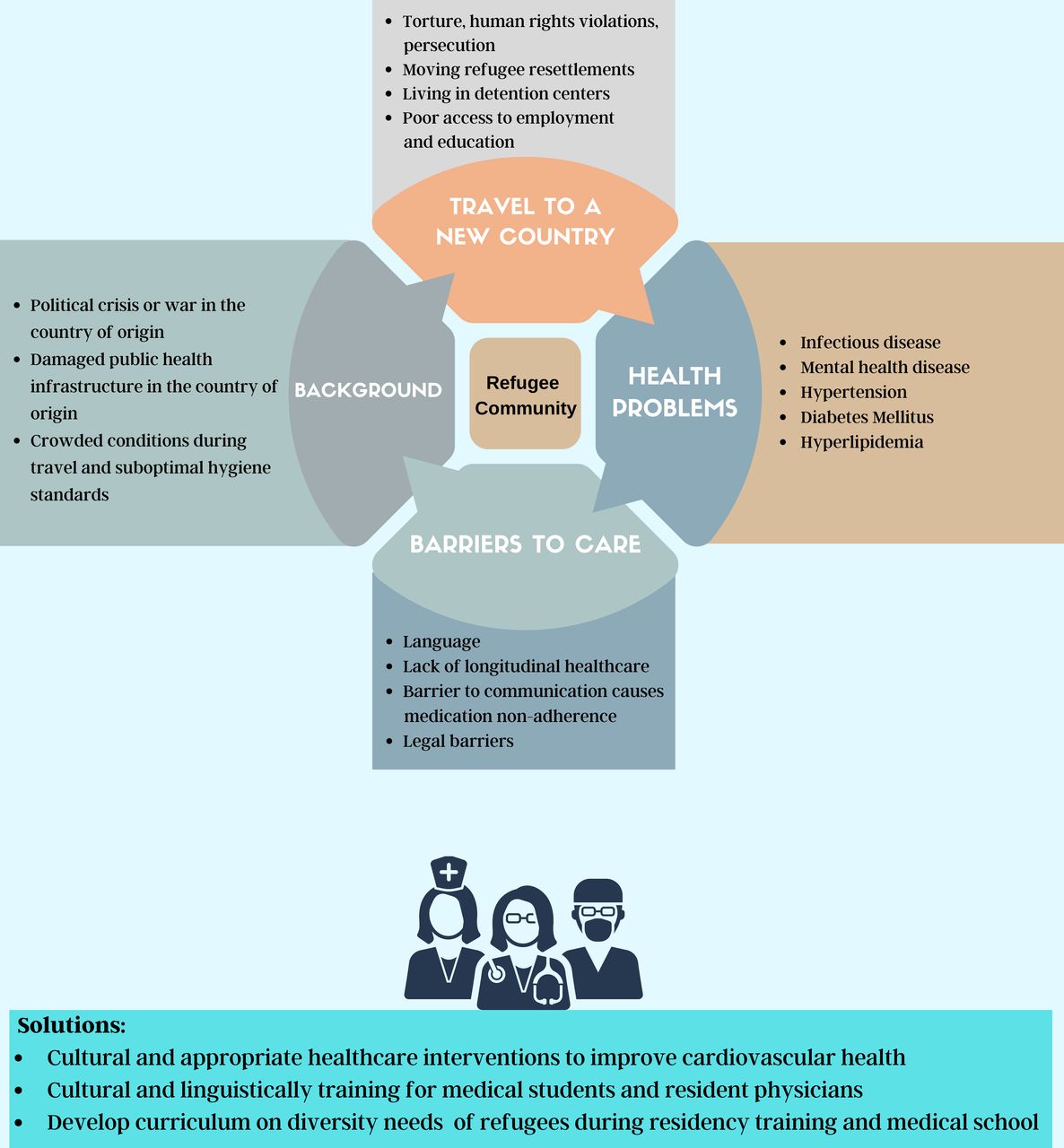
RIMs are predisposed to countless stressors, which influence their decision to migrate. Given their disposition and the social/global determinants of health that limit their ability to be treated with preventive medicine, RIMs will continue to be diagnosed with one or more of these lifestyle diseases. Preventive interventions are the primary means to minimise the impact of these diseases on the lives of RIMs. Simple, inexpensive interventions, such as community education and preventive campaigns among healthcare providers, can significantly impact RIM’s overall health. Collaboration among the RIM community, social service and healthcare providers is critical for bridging the gap and mitigating the extra burden of CVD on already traumatised and stressed RIM community members.(figure 1)
{kind=link}
Risk factors for cardiovascular disease in refugee communities.
Ethics statements
Footnotes
Twitter @hevalkelliMD
Contributors All persons who meet the authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in Heart.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Commissioned; internally peer reviewed.