Article Text

Statistics from Altmetric.com
- ACS, acute coronary syndrome
- BSE, British Society of Echocardiography
- CAD, coronary artery disease
- DTI, Doppler tissue imaging
- LBBB, left bundle branch block
- LV, left ventricular
- MRI, magnetic resonance imaging
The British Society of Echocardiography (BSE) procedure guidelines for the clinical application of stress echocardiography, recommendations for performance and interpretation of stress echocardiography are presented here.
1. BACKGROUND
The objective of guidelines is to enhance appropriateness of practice, improve quality of care, lead to better patient outcomes, and help authorities to decide on the approval of diagnostic or therapeutic procedures. For patients with coronary artery disease (CAD), one of the greatest challenges of our heath care system, a variety of diagnostic procedures is available at varying financial burdens. In order to improve cost effectiveness precise guidelines are needed to advise physicians.1
Stress echocardiography has become a valuable method for cardiovascular stress testing. It plays a crucial role in the initial detection of coronary artery disease, in determining prognosis and in therapeutic decision making.2,3 These recommendations refer to the use of stress echocardiography to assess myocardial ischaemia or viability in patients with coronary artery disease. Evaluation of valvar heart disease or cardiomyopathies is not included but the BSE will provide separate guidelines for these indications in the future.
Stress echocardiography is part of a diagnostic process, which often includes several diagnostic modalities, some of them complementary (for example, stress ECG), others competitive (for example, myocardial scintigraphy or magnetic resonance imaging (MRI)). This is reflected in this document, which outlines the indications and contraindications for stress echocardiography, the recommended methodology, and the clinical use of this technique. This document is intended to supplement other guidelines for cardiovascular stress testing, including the recently published guidelines for myocardial scintigraphy.4,5
Guidelines have to reflect the specific situation of the local health system and have to be updated to reflect the technical developments of the procedure and the developments of competing procedures. In particular there has been an increasing use of new imaging technologies for stress echocardiography such as contrast echocardiography and Doppler tissue imaging (DTI). There are no comprehensive documents available on how to implement these recent technologies in clinical stress echocardiography. The Policy Committee of the BSE established a working group to prepare this document and address this issue.
All recommendations are based on evidence from clinical studies, previous published guidelines of other societies such as the American Society of Echocardiography, or expert consensus of the writing and advisory groups.6–9 A writing group was composed of clinicians from BSE members all with subspecialty expertise in stress echocardiography. The advisory group consisted of nominated representatives of the BSE. Every effort was made to avoid conflict of interest from non-clinical relationships. All members of the writing group are asked to provide disclosure statements of such relationships, which might be perceived as real or potential conflicts of interest.
The guidelines are intended to establish standards for the clinical use of stress echocardiography. Therefore all applications/protocols refer to currently available technology and protocols, which are licensed for assessment of left ventricular (LV) wall motion alone. However, since simultaneous assessment of perfusion is also possible with these protocols and available contrast agents, these methodologies are also described. Protocols which exclusively make the diagnosis from perfusion images are excluded, although this may be an option in the future with broader evidence of the value of this approach.
The guidelines have been assembled from the knowledge available at the time of writing. The authors cannot assume liability for changes of dose regimens, machine settings, etc, due to advancing technology. However, regular review by the BSE Policy Committee will be undertaken to implement clinically relevant advances.
This document will be available on the homepage of the BSE (www.bcs.com/restricted/affiliates/bse.html).
2.INDICATIONS
Stress electrocardiography (ECG) has been the most frequently used initial stress test to evaluate patients with suspected coronary artery disease (CAD).1,2–12 Stress echocardiography can be used in addition to stress ECG or as the initial diagnostic tool.2 In both situations stress echocardiography or myocardial perfusion scintigraphy may be used.13–17 The techniques have similar sensitivity and specificity and the decision for one or the other test will depend on the local availabilities and expertise. Therefore, the indications for stress echocardiography widely overlap with the indications for myocardial scintigraphy. There are, however, clinical situations where myocardial scintigraphy is relatively contraindicated according to the procedure guideline for myocardial perfusion imaging. Dynamic exercise should not be used in patients with left bundle branch block (LBBB), bifascicular block, and ventricular paced rhythms, because dynamic exercise leads to perfusion abnormalities of the septum and adjacent walls in the absence of obstructive coronary disease but this may be less a problem with adenosine stress.4,18
2.1. To assess the presence and degree of coronary obstruction in patients with suspected coronary artery disease
2.1.1. Stress echocardiography following stress ECG
As part of an investigational strategy for the diagnosis of patients in whom stress ECG is non-conclusive.
2.1.2. Stress echocardiography as the initial diagnostic tool
For people for whom treadmill exercise is difficult or impossible because of poor mobility or inability to perform dynamic exercise.
For people with a lower likelihood of CAD and future cardiac events (intermediate pretest probability). The likelihood of CAD will be based on the assessment of a number of risk factors including age, sex, ethnic group, family history, associated co-morbidities, clinical presentation, physical examination and results from other investigations (for example, blood cholesterol values or resting ECG).
For people for whom stress ECG poses particular problems of poor sensitivity or difficulties in interpretation, including women, patients with cardiac conduction defects (for instance left bundle branch block and resting ST segment abnormalities), hypertensive heart disease, and diabetes.
2.2. To aid the management of patients with known or suspected coronary disease
To determine the likelihood of future coronary events—for example, after myocardial infarction or risk assessment for proposed non-cardiac surgery.19
To guide strategies of myocardial revascularisation by determining the haemodynamic significance of known coronary lesions.
To assess the adequacy of percutaneous and surgical revascularisation.
2.3. To assess myocardial viability and hibernation, particularly with reference to planned myocardial revascularisation
Dobutamine stress echocardiography (DSE) is one of four clinical imaging methods for assessment of viability/hibernation.20 Magnetic resonance imaging, myocardial scintigraphy, and positron emission tomography are alternative methods. Currently there is no consensus as to whether one of these methods is superior and therefore the decision for one or the other test will depend on the local availabilities and expertise.
3. CONTRAINDICATIONS
3.1. Absolute contraindications for all stress modalities
In patients presenting with an acute coronary syndrome (ACS), stress echo should be deferred for a period of time commensurate with the extent of ischaemia and infarction. This ranges from 24 hours for troponin negative ACS to seven days for the use of high dose dobutamine stress echo following substantial ST elevation infarction, especially when not revascularised acutely.
Left ventricular failure with symptoms at rest (in tertiary centres viability may be assessed using low dose dobutamine stress).
Recent history (within the last week) of life threatening arrhythmias.
Severe dynamic or fixed left ventricular outflow tract obstruction (aortic stenosis and obstructive hypertrophic cardiomyopathy). In low gradient aortic stenosis low dose dobutamine protocols may be used for assessment of the severity of the stenosis and operative risk stratification.
Severe systemic hypertension (systolic blood pressure > 220 mm Hg and/or diastolic blood pressure > 120 mm Hg).
Recent pulmonary embolism or infarction.
Thrombophlebitis or active deep vein thrombosis.
Known hypokalaemia (particularly for Dobutamine stress)
Active endocarditis, myocarditis, or pericarditis.
3.2. Absolute contraindications for vasodilator stress echocardiography
Suspected or known severe bronchospasm.
Second and third degree atrioventricular block in the absence of a functioning pacemaker.
Sick sinus syndrome in the absence of a functioning pacemaker.
Hypotension (systolic blood pressure < 90 mm Hg).
Xanthines taken in the last 12 hours, or dipyridamole use in the last 24 hours.
3.3. Relative contraindications to vasodilator stress
Bradycardia of less than 40 beats/min. Initial dynamic exercise normally increases the rate sufficiently to start the infusion.
Left main coronary artery stenosis in cases with equivocal degrees of stenoses on angiography. Significant stenoses represent an absolute contraindication.
Recent cerebral ischaemia or infarction.
4. METHODOLOGY
4.1. Imaging techniques
Native or contrast enhanced two dimensional echocardiographic recordings are used and CAD is evaluated by changes in global/regional wall motion and thickening of the left ventricle.7,8 Normal myocardium contracts at rest and increases its contractility and thickening during stress. Doppler tissue profiles, which reflect global and regional parameters of either systolic or diastolic function, can be employed but only in conjunction with two dimensional echocardiographic recordings. The rationale for the diagnosis of myocardial ischaemia is a relative reduction in myocardial blood flow sufficient to cause a decrease in myocardial contraction.1 Direct assessment of myocardial perfusion by assessment of myocardial contrast enhancement may be used as an add on in particular to confirm the findings of wall motion analysis. It may be used as an alternative, as soon as contrast agents are licensed for perfusion imaging.
The basis for the diagnosis of myocardial viability is contraction of the myocardium either spontaneously or after inotropic stimulation by activating contractile reserve.20 Contrast echocardiography provides adequate endocardial border definition in those patients in whom native images are suboptimal, and is useful for evaluation of myocardial perfusion. The presence of myocardial contrast indicates microvascular integrity, which implies viability. In the future, this technique may be used for viability studies in addition to, or instead of, low dose dobutamine.
4.2 Required ultrasound equipment
Because analysis of wall motion abnormalities is difficult and not reliable in the presence of poor quality images, every effort has to be made to optimise visualisation of the endocardial border and the myocardium. An appropriate scanner should provide tissue harmonic imaging and a contrast specific imaging modality in order to be applicable in the majority of patients. Doppler tissue imaging is optional and its clinical utility remains to be proven. Use of digital frame grabbers and split or “quad-screen” displays allows side-by-side comparison of rest and stress images using the same echo views and is obligatory for performing stress echocardiograms. These systems facilitate detection of subtle wall motion abnormalities and are recommended for all laboratories undertaking stress echocardiography.
4.3. Use of ultrasound contrast agents
Since image quality is crucial for reliable stress echocardiography, baseline images have to be reviewed before beginning the stress procedure.21 If image quality is suboptimal—for example, endocardial borders are barely or not visible in two or more myocardial segments—application of ultrasound contrast agents should be considered or the patient should be referred for another imaging test like myocardial scintigraphy or MRI.22 In the UK two contrast agents (SonoVue and Optison) are licensed for improving endocardial definition.23,24 When ultrasound contrast agents are used, contrast specific imaging modalities should be employed and it should be used both during baseline investigations and during (peak) stress. The stress protocols and image analysis are not different from those used for native stress echocardiography.
4.4. Personnel required
Two persons are required to record and monitor stress echocardiography—one of them having substantial experience in the evaluation of patients with ischaemic heart disease and in analysis of wall motion/thickening abnormalities. The recordings should be performed by a skilled echocardiographer (technician or physician). The personnel requirements and the level of monitoring required will vary with local standards of care and the type of stress being employed. If a physician is not participating in the study, one should be available in the immediate locality in case of acute problems. One of the personnel present should be qualified in advanced life support, the other in basic life support. Personnel should be sufficiently trained in contrast echocardiography when contrast is given; the possibility of hypersensitivity should be anticipated.
Recording and interpretation of stress echocardiograms requires extensive experience in echocardiography and should be performed only by technicians and physicians with specific training in the technique. Ideally full BSE accreditation or comparable certificate supplemented by passing specific training courses for stress echocardiography should be achieved. The BSE Policy Committee recommends that physicians have performed and interpreted a minimum of 100 studies under supervision before they can perform stress echocardiography independently.8 Learning curves of 100 investigations for performing and interpreting stress echos seem reasonable and reflect our current practice.
5. STRESS PROTOCOLS
Table 1 lists the protocols for stress echocardiography.
Protocols for stress echocardiography
The selection of the stress modality is mostly determined by the patient’s capacity to exercise, the local experience and by the indication.
5.1. Exercise echocardiography
Very useful and perhaps the most physiological stressor for assessment of myocardial ischaemia in patients able to exercise.
Imaging can be performed pre- and immediately post-treadmill exercise, upright or supine bicycle ergometry. The protocols are the same as for stress electrocardiography.10–12 Because ischaemia induced wall motion abnormalities may resolve quickly, post-exercise imaging should be accomplished within 60–90 seconds of termination of exercise.
Supine bicycle ergometry on a special bed, which can be rotated, allows imaging at incremental levels of stress including peak exercise. While treadmill exercise echocardiography is terminated at traditional end points such as arrhythmias and cardiovascular symptoms, bicycle exercise provides additional echocardiographic end points because it allows continuous visualisation of wall motion.8 It is recommended that exercise echocardiography with on-line monitoring during bicycle stress be terminated at traditional end points as well as at the time of development of wall motion abnormalities corresponding to two or more coronary segments, or wall motion abnormalities associated with ventricular dilation and/or global reduction of systolic function. Supine and upright bicycle exercise appears to have equivalent degrees of accuracy.
5.2. Non-exercise echocardiography
5.2.1. Dobutamine stress echocardiography
Two dimensional echocardiography combined with dobutamine infusion can be used for assessment of myocardial ischaemia and myocardial viability.25,26 For the diagnosis of myocardial ischaemia, there appears to be no difference in the accuracy and prognostic information of dobutamine stress echo compared to exercise stress echo, although it is possible that for milder forms of coronary artery disease, treadmill may be advantageous.27 However, exercise stress echo is more challenging in terms of acquiring good quality recordings. For patients unable to exercise, dobutamine stress echo is indicated unless there is a contraindication to dobutamine (in which case dypyridamole, adenosine, or pacing may be used). For risk assessment before non-cardiac surgery dobutamine stress echocardiography has been proven to prognosticate patients at risk.16
For assessment of myocardial viability use of low and high dose dobutamine seems to be the best stress method for echocardiography.20
5.2.1.1. Dobutamine protocol for assessment of myocardial ischaemia
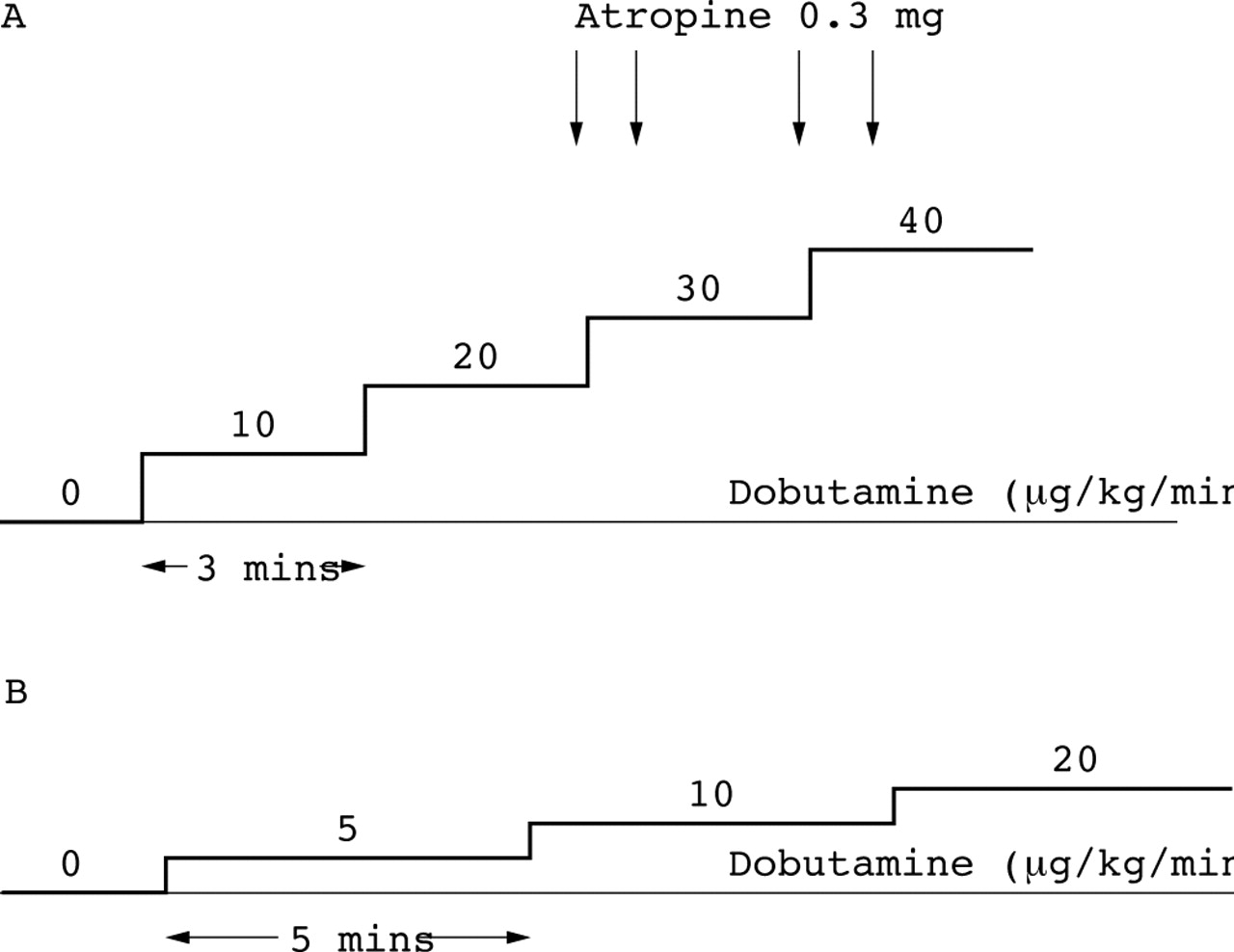
Myocardial ischaemia is assessed by graded dobutamine infusion (starting with 5 or 10 μg/kg/min, followed by 20, 30 and 40 μg/kg/min in three minute stages) which increases myocardial oxygen demand in a fashion analogous to staged exercise (fig 1A). When assessing only ischaemia, it is advisable to omit the 5 μg/kg/min stage thus reducing the time of the test. Contractility, heart rate, and systolic blood pressure are all increased. An advantage of dobutamine is that it has a rapid onset and cessation of action, and its effects can be reversed by β blocker administration (as antidote any β blocker can be given, although we recommend esmolol 0.5 mg/kg). In patients who have an “inadequate” heart rate response to dobutamine, atropine can be used to increase heart rate. Atropine should be used at the minimum effective dose (typically ⩽1.2 mg) and administered in 0.3 mg increments every 60 seconds until the desired heart rate response is seen. Atropine administration should be considered when heart rate has not increased after the 20 μg/kg/min dobutamine level.

Dobutamine stress echocardiography: protocol A for assessment of myocardial ischaemia; protocol B for assessment of myocardial viability. It is recommended that baseline and peak images always be captured for digital comparison. Based on clinical necessity and laboratory preference, the remaining two images may be a combination of low stress, intermediate stress, post-atropine, or recovery images.
In patients with ongoing β blocker treatment a reduced sensitivity for reversible ischaemia has been found even if target heart rate was reached with additional atropine injections, caused by the negative inotropic effect of β blockers.28 Therefore stopping β blocker treatment 48 hours before the test is useful to increase sensitivity of the test. However, if this may not be possible, patients still can be accepted for exercise or dobutamine stress with atropine. In these cases the clinical relevance of the underlying ischaemia should be judged under the given treatment.
During dobutamine echocardiography, images can be recorded at baseline, low stress (10% increase in heart rate), intermediate stage (70% of the age predicted heart rate), at peak stress (85% of the age predicted heart rate), and sometimes during recovery. Currently available digital imaging software is configured for capture of four or more different time points. It is recommended that baseline and peak images always be captured for digital comparison. Based on clinical necessity and laboratory preference the remaining two images may be a combination of low stress, intermediate stress, post-atropine, or recovery images. Dobutamine stress echocardiography, like bicycle echocardiography, allows on-line monitoring of ventricular function. Termination of the test should occur at both traditional end points and for development of major wall motion abnormalities with systolic dysfunction as described for bicycle exercise (see 7).
5.2.1.2. Dobutamine protocol for assessment of myocardial viability
Low dose dobutamine stress should be used for assessment of contractile reserve. The patient will undergo the DSE using standardised incremental infusions of 5, 10, and 20 μg/kg/min (fig 1B). Each dose may to be given for up to five minutes. Mandatory image acquisition using all available views is required at the end of each stage. If a 10% increase in heart rate is achieved, the protocol is completed. If the operator feels that there may be an overshooting of the heart rate, a 15 mug/kg/min stage may be added. After completing the low dose protocol higher dosages of dobutamine (30 and 40 μg/kg/min) may be given to look for biphasic response (reversal of contractile function). The presence of a biphasic response (improved contraction at low dose followed by reduced contraction at peak) indicates inducible myocardial ischaemia and is perhaps the strongest predictor for recovery of myocardial dysfunction following revascularisation. It indicates a viable but jeopardised myocardial region.
5.2.2. Vasodilator stress echocardiography
In patients with significant coronary stenoses, dipyridamole or adenosine infusion results in regional redistribution of coronary blood flow.29–31 Regional wall motion/thickening abnormalities resulting from diminished flow distal to coronary stenoses can be assessed by simultaneous two dimensional echocardiography. The regional flow mismatch caused by dipyridamole or adenosine is due to a twofold or more increase of myocardial blood flow in those myocardial segments supplied by normal coronary arteries, whereas in segments supplied by stenotic arteries the flow often is unchanged or decreased. However, as long as the oxygen demand is not increased in these segments there is no ischaemia and consequently no wall motion abnormality. Vasodilator stress echocardiography needs only baseline recordings and recordings at hyperaemia. Therefore recording and reading is shorter than with exercise or dobutamine stress. Since vasodilators often result in minor increase of heart rate and blood pressure, atropine may be added to increase sensitivity of vasodilator stress echo. Therefore vasodilator stress seems to be more suitable for direct assessment of myocardial perfusion using contrast echocardiography. This indication is not yet licensed in the UK. Vasodilator stress echo using two dimensional echocardiography should only be considered when physical stress is not possible and there are contraindications to dobutamine, because its sensitivity to assess mild to moderate coronary artery disease is reduced.9,32
5.2.2.1. Dipyridamole protocol for assessment of myocardial ischaemia
The currently recommended protocol for dipyridamole echocardiography includes continuous electrocardiographic and echocardiographic monitoring during a two stage infusion. The first stage consists of 0.56 mg/kg dipyridamole over four minutes (fig 2). Monitoring continues for four minutes. If there is no adverse effect, clinical or echocardiographic end point occurs, then an additional 0.28 mg/kg is infused over two minutes. As with dobutamine, atropine can be used to increase heart rate. Typically, imaging is performed continuously, and if digital capturing is used, images are captured at baseline, at the termination of phase one, termination of phase two, and at recovery. As in the case of dobutamine, atropine can be added after the second stage to increase heart rate and improve sensitivity. Aminophylline (240 mg intravenously) should be available for immediate use in case of an adverse dipyridamole related event.

Dipyridamole stress echocardiography, protocol for assessment of myocardial ischaemia. *If there is no adverse effect, clinical or echocardiographic end point occurs, then an additional 0.28 mg/kg is infused over two minutes. As with dobutamine, atropine can be used to increase heart rate.
5.2.2.2. Adenosine protocol for assessment of myocardial ischaemia
Adenosine can be used in a similar manner and is typically infused at a maximum dose of 140 μg/kg/min over six minutes (fig 2). Imaging is performed before and three minutes after starting adenosine infusion.
5.2.3. Pacing
In most paced patients exercise, dobutamine, and vasodilator stress protocols are applicable. Pacing, preferably by atrial leads, may be considered in patients with permanent pacemakers if the required increase in heart rate cannot be achieved by exercise or dobutamine. An intravenous access is mandatory. Pacing by temporary intravascular or oesophageal leads is usually not needed for clinically indicated stress echocardiography. Since pacing alone only produces chronotropic stress, it is usually considered to have lower sensitivity than the inotropic + chronotropic stress achieved by pharmacological stress testing. Since some patients may develop a Wenckebach phenomenon with increasing atrial rates atropine injections may be needed to provide 1:1 atrioventricular (AV) conduction.
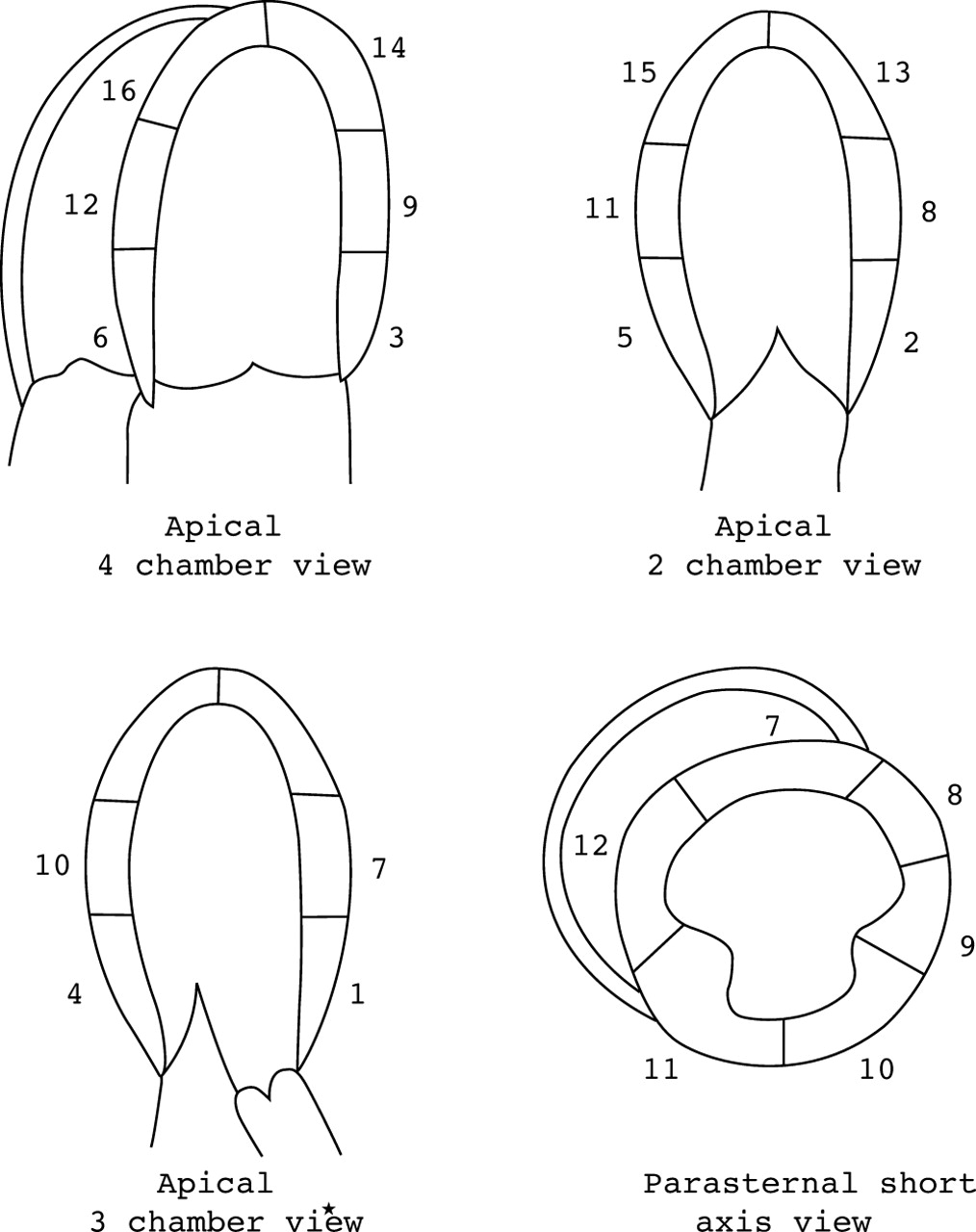
6. IMAGING PROCEDURE
Multiple views have to be recorded to ensure visualisation of left ventricular segments supplied by each of the three major coronary distributions.8,33 Four views are usually sufficient (fig 3): apical four chamber and two chamber views, parasternal short axis and long axis (or apical long axis). Subcostal or additional short axis views can be substituted when necessary or when more appropriate for visualisation of specific anatomy. The imaging procedure is the same for standard harmonic imaging and contrast echocardiography. When using contrast, both baseline and stress images should be enhanced. Two dimensional echocardiograms are individually optimised according to established standards. For contrast echocardiography the contrast presets of the ultrasound scanners are recommended. The frame rate should be at least 25 frames per second. However with heart rate > 140 beats/min, acquisition may be enhanced with frame rates > 30 frames per second. For Doppler tissue recordings higher frame rates may be useful. The number of frames captured can vary from eight per cardiac cycle, which captures only systole, to >25 frames to capture of the entire cardiac. No clinical advantage to either scheme has been demonstrated. Additional storage on videotape may be performed as back up and to acquire non-standard views and multiple cardiac cycles if the digital archiving system does not provide these capabilities.
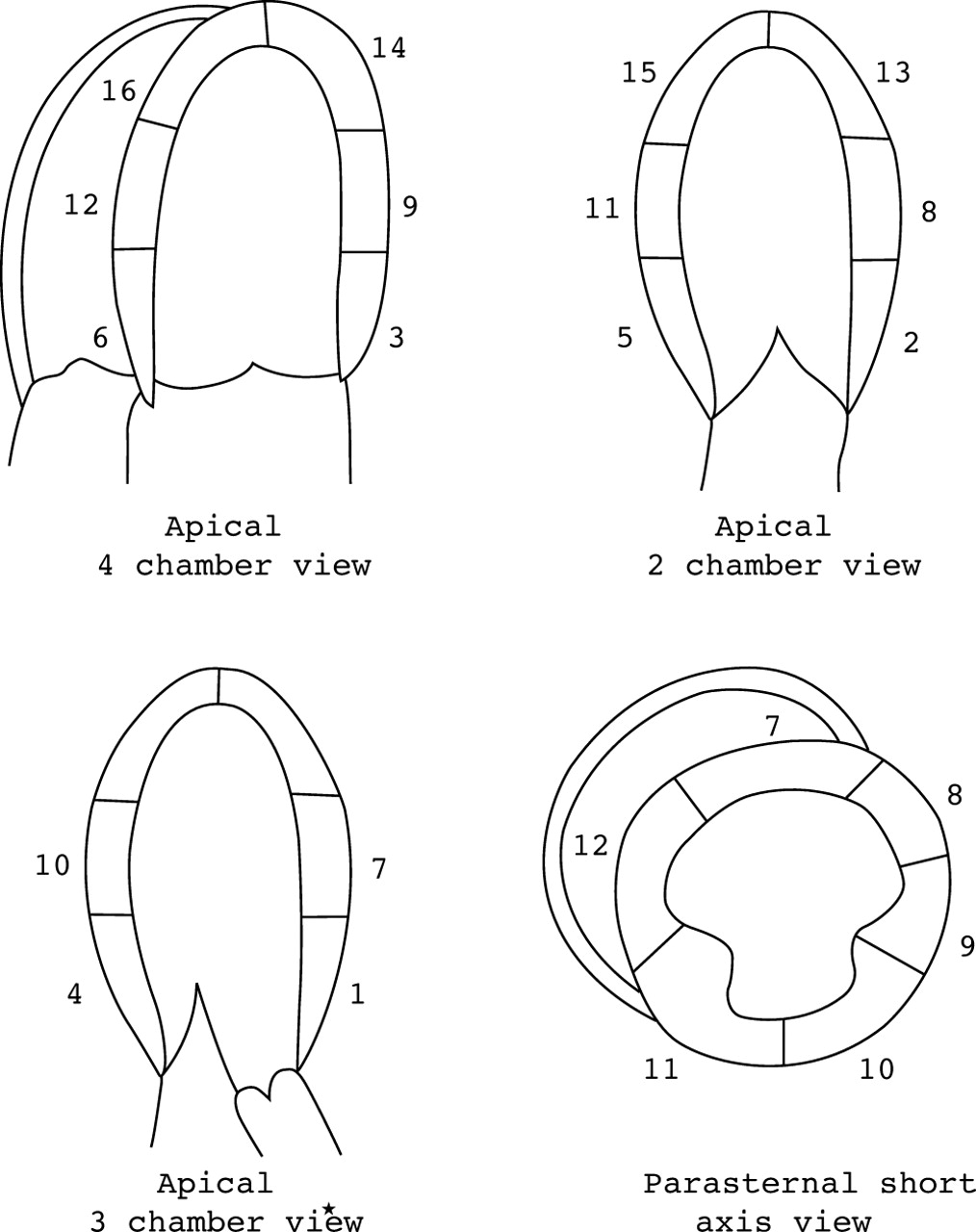
Sixteen segment model showing the relevant echo-tomographic views with: 1, basal anterior septal; 2, basal anterior; 3, basal lateral; 4, basal posterior; 5, basal inferior; 6, basal septal; 7, mid anterior septal; 8, mid anterior; 9, mid lateral; 10, mid posterior; 11, mid inferior; 12, mid septal; 13, apical anterior; 14, apical lateral; 15, apical inferior; 16, apical septal. *A parasternal long axis view may be used in alternatively or in addition.
7. MONITORING REQUIREMENTS AND TERMINATION CRITERIA
As with other forms of stress testing, standard electrocardiographic and blood pressure monitoring is also performed (table 2). This may provide ancillary diagnostic and prognostic information during exercise studies. Electrocardiographic monitoring has limited diagnostic value during pharmacologic stress and ECG recording is only needed to ensure recording of single loops and to monitor for arrhythmias. However, if a 12 lead ECG is not performed during pharmacological stress, a 12 lead ECG recorder should be readily available.
Monitoring requirements for stress echocardiography
The monitoring requirements are listed in table 2. While treadmill exercise echocardiography is terminated at traditional end points such as attainment of target heart rates and cardiovascular symptoms, bicycle exercise and pharmacologic stress provide additional echocardiographic end points because they allow on-line, continuous visualisation of wall motion and thickening. It is recommended that stress echocardiography with on-line monitoring be terminated at traditional end points as well as at the time of development of wall motion abnormalities corresponding to two or more myocardial segments, or wall motion abnormalities associated with ventricular dilation and/or global reduction of systolic function (table 3). Because of the time constraints this decision is usually made by visual judgement.
Termination criteria
8. ANALYSIS METHODS
Usually a comprehensive assessment is made after the stress test with side by side comparisons of recordings captured at baseline and stress.8 During bicycle and pharmacological stress the recordings have to be visually assessed for development of new wall motion abnormalities and LV dilation in order to terminate the test. Stress echocardiograms can be analysed on several planes of complexity, which range from a qualitative assessment of segmental wall motion in response to stress to highly detailed schemes for quantitative analysis. The manner in which stress echocardiograms are analysed is dependent on prevailing local preferences and the need for detailed investigational data versus clinical data. An algorithm commonly used for detection of ischaemia is shown in table 4.
Classifications and clinical implications of stress echo responses. Modified from the American Society of Echocardiography guidelines8
For image interpretation, multiple cine loop display is recommended. This can show up to four different stress levels for each imaging plane simultaneously. It is useful to further review the recordings on the videotape, in particular when the scanplane was very unstable during the recording. Analysis is carried out according to the standards of the American Society of Echocardiography.8
A systematic review is recommended, starting with assessment of the image quality. Endocardial border definition can be used as an indicator of image quality: if endocardial border is not seen or is barely visible, wall motion and thickening cannot be reliably assessed in this segment. Image quality is graded as good, acceptable, or poor and non-diagnostic segments are identified. On resting images, global function is assessed by LV ejection fraction using visual estimate or from measuring end diastolic or end systolic volumes in two apical views. Analysis of DTI recordings may supplement interpretation. Rest and stress images are then compared for the development of global LV dysfunction (left ventricular enlargement and shape changes) and regional dysfunction.
Segmental evaluation of wall motion using a 16 or 17 segment model is recommended.8,33 Wall motion is evaluated in every assessable segment using a four step visual score ranging from normal (1), hypokinetic (2), akinetic (3), to dyskinetic (4). Calculation of a wall motion score may be performed in order to facilitate serial comparison. The sum of the segmental wall motion scores is the (global) wall motion score; the wall motion score index is calculated by dividing the wall motion score by the number of segments. Normal contraction results in a wall motion score index of 1; a higher score is indicative of wall motion abnormalities. For assessment of myocardial viability assessment of wall thickness is useful. Diastolic wall thickness ⩽ 5 mm at rest indicates non-viability and increases diagnostic confidence in combination with absent contractile response to dobutamine. After analysis of global and regional function at rest, corresponding assessment is recommended for each stage of stress, including comparison of baseline to stress recordings. Ischaemia may be considered as present when there is a worsening of wall motion in two or more segments. Whether the development of dyskinesia in an akinetic segment represents ischaemia is still a matter of debate, as is the absence of a hyperdynamic response. Viability may be considered as present when there is an improvement of wall motion in two or more segments—for example, from akinesia to hypokinesia. A biphasic response is a strong predictor for recovery of myocardial dysfunction following revascularisation (see 5.2.1.2). The adequacy of stress should be noted, as well as the exercise time, symptoms, haemodynamic observations, and ECG changes.
In contrast echocardiograms, wall motion is assessed in the same way as in native echocardiograms. The contrast agents are not yet licensed for assessment of myocardial perfusion. With current knowledge the results of perfusion imaging should be used in conjunction with the findings of visual LV wall motion analysis.34 Generally, concordance of wall motion analysis and perfusion imaging increases the diagnostic confidence.
9. REPORTING
The patient’s personal demographic details should be included at the start of the report. Any hospital/clinic identification number and source of referral should also be included (fig 4). The clinical indications for the study should be stated, including any relevant clinical history and concurrent medications. This provides justification for the study, summarises clinical information that may have been gleaned from a number of sources, and focuses the final conclusion.35

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Template for report of stress echocardiography.
The date of the study, stress protocol, and imaging technique should be specified, including the name and dosage of contrast agents. Changes of blood pressure and heart rate should be described briefly; reporting the resting and peak stress blood pressure is usually sufficient. In patients who underwent treadmill or bicycle stress the exercise capacity should be included since it of prognostic value. For exercise and dobutamine stress echocardiography the age, sex, and specific target heart rate should also be included. Further measurements or details of ECG changes are included if relevant.
The findings section should include a statement on the completeness and image quality, since diagnostic confidence heavily depends on high quality recordings. The non-diagnostic segments should be specified. Then the results of the analysis of baseline are presented. If global and/or regional left ventricular function is abnormal, the segments involved and the degree of abnormality (hypokinetic, akinetic, dyskinetic) have to be listed. Schematics of the single views may be helpful to illustrate the distribution of wall motion abnormalities. The results of analysing stress recordings can be recorded briefly: normal response to stress if there is hyperdynamic contraction in all segments or abnormal response with worsening wall motion, listing the segments involved and degree of abnormality. In viability studies it is important to evaluate whether the akinetic segments show improvement during stress.
10. MAINTAINING QUALITY
The BSE Policy Committee recommends that physicians interpret a minimum of 10 stress echocardiograms per month to maintain interpretational skills. It is recommended that sonographers perform a minimum of 10 stress echocardiograms per month to maintain an appropriate level of skill.8,36
Regular audits are useful to review the quality and accuracy of the stress echocardiograms. This audit should include the total number of stress echocardiograms performed per month for the time period audited: the number of procedures per sonographer and reads per physician; indications, imaging technology; use of contrast; stress protocols; quality of the studies; termination criteria; results (negative or positive for assessment of ischaemia, viable or non-viable for viability studies); and complications. For those patients undergoing coronary angiography, it would be ideal to have the results of coronary angiography for quality control. This may be difficult to achieve for some stress echo units. However, reviewing false positive and negative findings should be an integral part of regular audit.
11. SAFETY-RISK/BENEFIT CONSIDERATIONS
Stressing of the patient and inducing myocardial ischaemia carries a low risk of complications. For exercise echocardiography the risk is similar to that of a stress ECG, for dobutamine stress echocardiography a 1 in 14000 risk of death and 0.19–0.3% life threatening events—for example, arrhythmias have been reported.37 For ultrasound, contrast media side effects have been reported but they are usually mild. However, rare allergic and potentially life threatening reactions may occur and the investigators have to prepared for such an event with appropriate drugs stored in the echo department. The indications for stress echocardiography listed in section 2 reflect the risks of the procedure and consider the benefits of an accurate diagnosis on further patient management.9
12. CONCLUSION
Stress echocardiography is a clinically valuable technique for evaluating patients with known or suspected ischaemic heart disease. The indications are based on evidence from numerous clinical trials and expert opinion. The stress protocols, imaging procedures, and training have been standardised. In experienced hands, accuracy is equivalent to that of radionuclide techniques.38 Recent developments in the field like perfusion imaging or Doppler tissue/strain imaging are expected to further increase accuracy and feasibility.
APPENDIX
Chronic coronary artery disease—level of evidence for stress echocardiography, modified American College of Cardiology/American Heart Association (ACC/AHA) practice guidelines.7 The BSE indications include class I and IIa indications (see chapter 2).
Class I (test is useful)
Diagnosis of myocardial ischaemia in symptomatic patients.
Assessment of myocardial viability (hibernating myocardium) for planning revascularisation.
Assessment of functional significance of coronary lesions in planning percutaneous transluminal coronary angioplasty.
Assessment for restenosis after revascularisation in patients with atypical recurrent symptoms.
Class IIA (weight of evidence/opinion is in favour of usefulness of the test)
Assessment for restenosis after revascularisation in patients with typical recurrent symptoms.
Assessment of prognosis in selected patients unable to exercise or in whom ECG is less reliable (with the following abnormalities: pre-excitation syndrome, paced ventricular rhythm, LV hypertrophy, more than 1 mm of ST segment depression at rest, complete LBBB).
Detection of coronary arteriopathy in patients who have undergone cardiac transplantation.
Detection of myocardial ischaemia in women with intermediate pretest likelihood of CAD.
Class IIb (usefulness of the test less well established by evidence/opinion)
Assessment of asymptomatic patient with positive results form screening exercise ECG.
Class III (test is not useful based on current evidence/opinion)
Screening of asymptomatic persons with low likelihood of CAD.
Routine periodic reassessment of stable patients for whom no change in therapy is contemplated.
Routine reassessment of asymptomatic patients after revascularisation.