Article Text

Statistics from Altmetric.com
- BNP, brain natriuretic peptide
- LV, left ventricular
- LVEF, left ventricular ejection fraction
- LVSD, left ventricular systolic dysfunction
- NT BNP, N terminal pro-brain natriuretic peptide
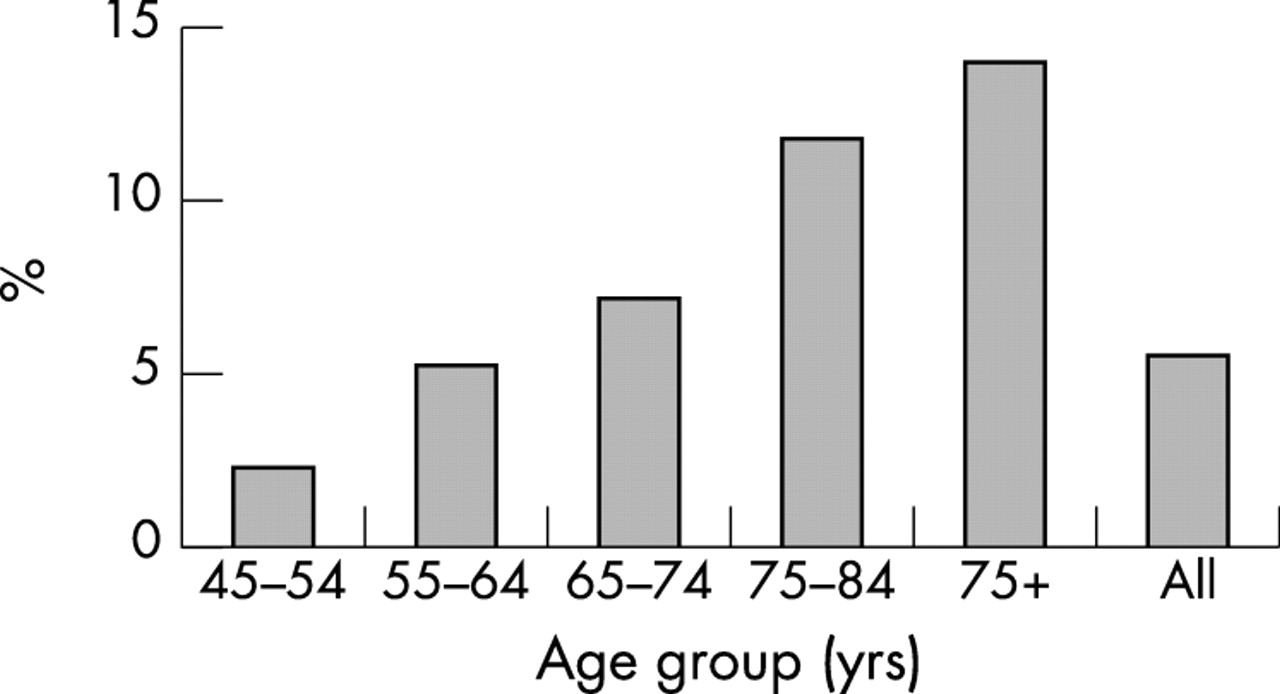
Heart failure is a growing and increasingly important chronic disease of the western world, occurring in at least 2% of the adult population and rising to 3% in those aged over 75 years.1,2 In a recently conducted study in Harrow of 1400 subjects who were invited to undergo echocardiography for assessment of left ventricular (LV) function the overall prevalence of symptomatic and asymptomatic LV dysfunction was 2% and rising to 8% above the age of 65 years (fig 1).3 Although the incidence of most cardiovascular diseases has declined over the past 20 years, the incidence of heart failure has continued to rise, due to the fact that more people are surviving after acute myocardial infarction and also to the increasing number of elderly people.4 A diagnosis of heart failure is associated with high mortality, morbidity, and cost.5 It has a worse prognosis than breast cancer or prostate cancer and is second only to stroke in terms of health care costs.6 Heart failure costs the USA over $8 billion (£5 billion) each year and 5% of all admissions in the UK have a diagnosis of heart failure.7 Indeed, hospital admission accounts for 70% of the cost of heart failure due to the number of day beds that are occupied.5

Prevalence of left ventricular systolic dysfunction (left ventricular ejection fraction < 50%), according to age group.3
Early detection of heart failure caused by left ventricular systolic dysfunction (LVSD) is important as early initiation of drug treatment, including angiotensin converting enzyme inhibitors, β blockers, and aldosterone receptor antagonists, has been shown to reduce mortality, morbidity, and hospitalisation.8,9 Indeed, it has been shown that early initiation of treatment in asymptomatic left ventricular dysfunction will prevent or retard progression to heart failure.10 However, the key to reduction of mortality, morbidity, and cost of heart failure is accurate and early diagnosis of LVSD. Unfortunately, heart failure is difficult to diagnose accurately on clinical grounds.11–14 The heavy community burden, difficulty in diagnosis, response to early treatment, and presence of significant asymptomatic LVSD have led to a call for programmes for screening and treating symptomatic and asymptomatic LVSD.15
DIAGNOSIS OF HEART FAILURE
Heart failure is commonly misdiagnosed despite symptomatology, mainly because of the non-specificity of the clinical symptoms and the non-sensitivity of the clinical signs.11–14 Not surprisingly, the validity of a clinical diagnosis of heart failure in primary care is poor. Rates of misdiagnosis when patients are assessed against objective criteria range from 25–50%.12 In another series only 26% of patients with suspected heart failure had a diagnosis of LVSD.14 Caruana and colleagues reported that of the 159 patients referred to hospital with suspected heart failure, 109 had preserved LV function of which only seven did not have an alternative explanation for their significance of heart failure.16 Thus, to establish positively a diagnosis of heart failure in primary care, patients must be referred for cardiac imaging. Are there alternatives to cardiac imaging in primary care for the diagnosis of left ventricular dysfunction? Although a normal ECG usually excludes left ventricular dysfunction,17 an abnormal ECG has a low predictive value for LVSD. In addition to this, ECGs are not widely available in primary care and changes may be subtle and may not be recognised by primary care physicians. All of these factors ultimately mean that referral for cardiac imaging is still required for the majority of patients.
Echocardiography
Despite the availability of many cardiac imaging techniques, echocardiography is currently the most widely used and cost effective diagnostic imaging test to assess LVSD. On the basis of this, echocardiography has been proposed to be the screening method of choice15,18 However, a recent survey of a random sample of primary care physicians across six European countries reported only 5% (Netherlands) to 37% (UK) of general practitioners had direct access to echocardiography.19 This poor access is partially caused by lack of trained staff to run clinics and partially due to availability of funding to run such clinics.20 In a study, conducted at Harrow in a high risk population to screen for LVSD, the prevalence of symptomatic LVSD was 8%, or approximately 10 000 subjects.3 This would mean an establishment of a dedicated echocardiographic service in the hospital to screen these patients which will be costly even if a high risk population were targeted.
Recent advances in ultrasound technology have led to miniaturisation of the echocardiography system, resulting in fully portable and truly hand held imaging systems. These systems are small, lightweight, battery operated, and capable of producing image quality comparable to that seen on high end echocardiographic systems.21,22 Although most of these devices have only rudimentary colour flow Doppler and lack sophisticated Doppler, they can provide diagnostic two dimensional information on chamber size, estimation of left ventricular hypertrophy, left atrial size and left ventricular ejection fraction (LVEF), size and dynamics of inferior vena cava, and address questions on pericardial disease compared to that obtained using the more expensive, non-portable standard echocardiographic platforms. In a recent study, we compared image quality of a hand held ultrasound system to that of a standard echocardiography system in 562 subjects. The hand held device failed to visualise only 7% of the myocardial segments.22 An LVEF could be estimated visually in 97% of the subjects undergoing hand held echocardiography in this study.21 With further development in computer technology, tissue harmonic imaging has now been incorporated in many hand held systems allowing even better visualisation of the myocardial segments.22 The hand held devices have already found roles on coronary care units, on ward rounds, in outpatient clinics, postoperatively, and in intensive care units in the hospital setting.22–27
HAND HELD ECHOCARDIOGRAPHY SYSTEM FOR SCREENING FOR LVSD IN THE COMMUNITY
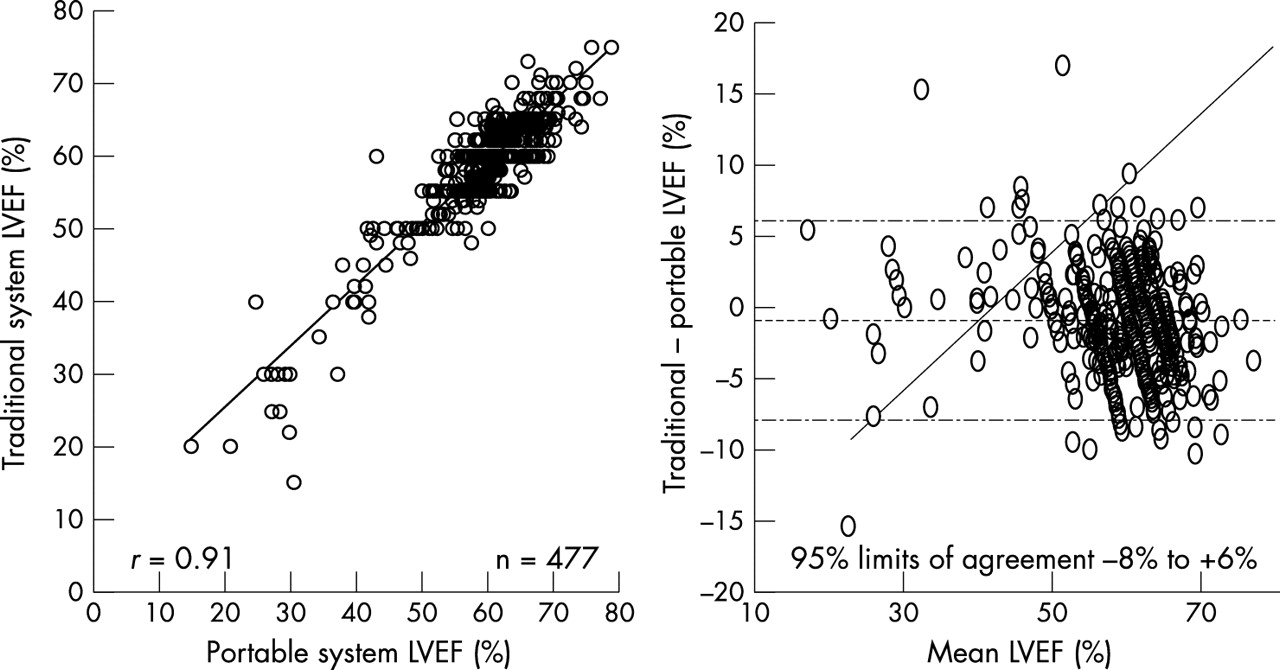
Hand held systems allow realistic opportunity for a screening service outside the hospital setting. This would potentially allow easier access to screening for LVSD, improving response rates and cost savings compared to hospital based programme. We conducted a study to validate the accuracy of a hand held system in screening for LVSD both in low risk and high risk members of the community for potential future community based screening programmes using such devices.21 We compared the hand held system with the standard echocardiography system for assessment of LVEF. This study found that hand held echocardiography accurately discriminated normal from abnormal left ventricular systolic function, correctly diagnosing 96% of cases of mild LVSD and 100% of cases of significant LVSD at the expense of over-diagnosing in only 2% of the population screened (table 1, fig 2). It also showed very good inter-observer variability, with reproducibility a prerequisite of any screening modality (fig 3). Thus, hand held echocardiography systems are an accurate and reproducible screening technique for the assessment of LVSD in the community. However, all hand held studies with a suspicion of LVSD should be referred for full echocardiography by a standard system. Are there more cost effective alternatives to point-of-care echocardiography in the primary setting?
Comparison between portable and traditional echocardiography systems for assessment of left ventricular function
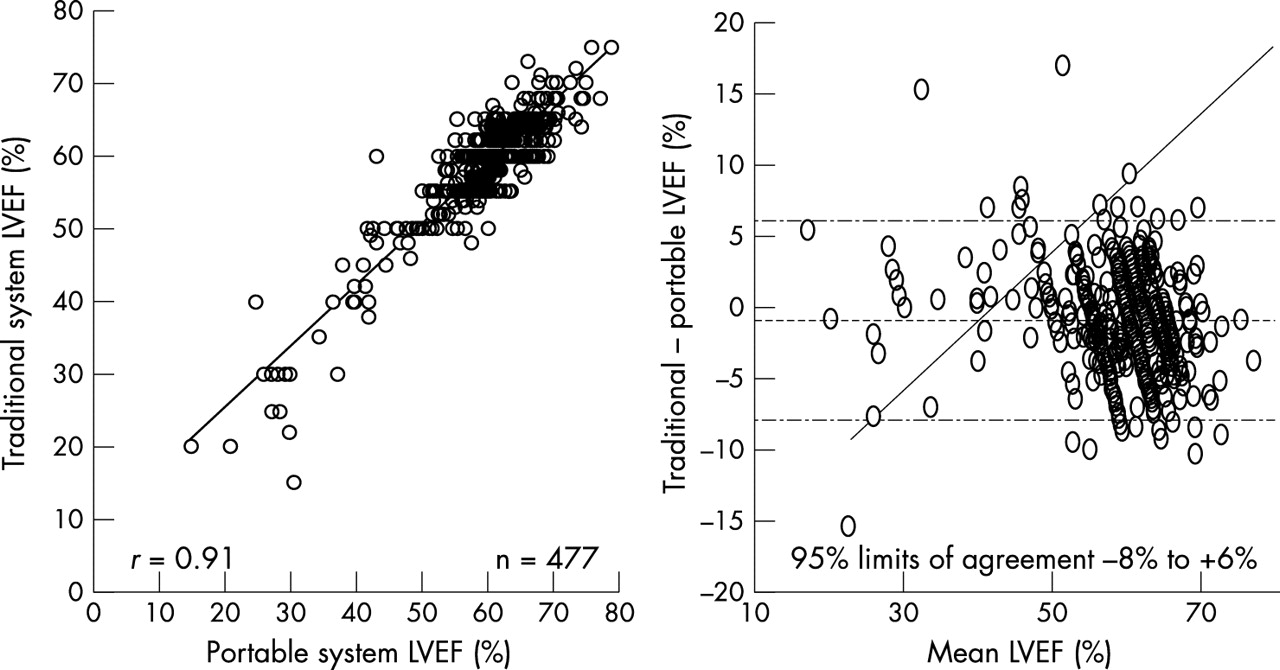
Scatter plot (left panel) and Bland-Altman plot (right panel) comparing portable echocardiography with traditional echocardiography in assessing left ventricular ejection fraction.21

Scatter plot (left panel) and Bland-Altman Plot (right panel) showing inter-observer reproducibility for hand held echocardiography device.21
NATRIURETIC PEPTIDES FOR SCREENING FOR LVSD IN THE COMMUNITY
Plasma natriuretic peptides have been advocated for screening for LVSD12–13,15; this is because they are released from the myocardium in response to myocardial stretch,28,29 as occurs in LVSD and heart failure. Indeed, plasma concentrations of both brain natriuretic peptide (BNP) and its co-release peptide N terminal pro-brain natriuretic peptide (NT BNP) have been shown to increase dramatically in subjects with both LVSD and heart failure.30,31 BNP testing had a sensitivity of 97%, a specificity of 84%, a positive predictive value of 70%, and a negative predictive value of 98% in 106 patients with symptoms of recent onset of heart failure who were referred to a rapid access heart failure clinic.31 Similar figures were reported in a population of 1653 adults aged between 25–75 years who were screened in Glasgow13 and in 155 patients aged over 75 years who were screened in primary care.32 Advances in biochemical assays have led to commercially available bedside and laboratory testing for serum or plasma natriuretic peptide levels.33,34
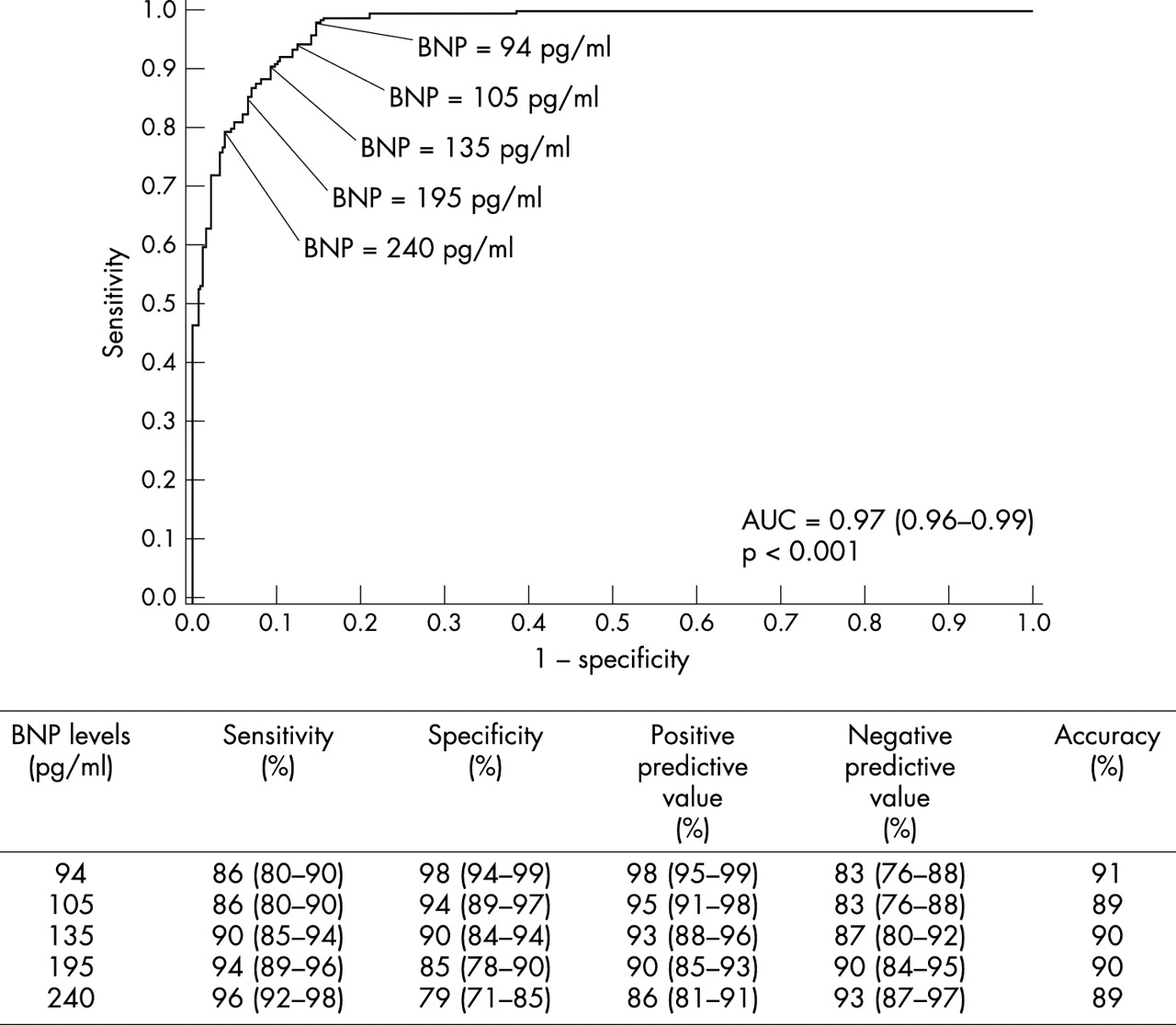
What should be the cut-off for BNP value to optimally diagnose heart failure. In a study by Morrison and colleagues, the authors obtained BNP values in 321 patients presenting to the emergency department with acute dyspnoea. The area under ROC curve was 0.96 for diagnosing heart failure.34 Figure 4 summarises the various cut-off values of BNP values for diagnosis of heart failure. A value of 94 pg/ml and 240 pg/ml patients gave negative predictive values of 83% and 91%, respectively, and a positive predictive value of 98% and 86%, respectively.34 In another study where NT BNP was estimated in community screening for LVSD assessed by echocardiography, the cut-off of 33 pg/ml provided a negative and positive predictive value of 99% and 8%, respectively.35 In other words, a value < 33 pg/ml effectively ruled out LVSD, in subjects being screened for LVSD.
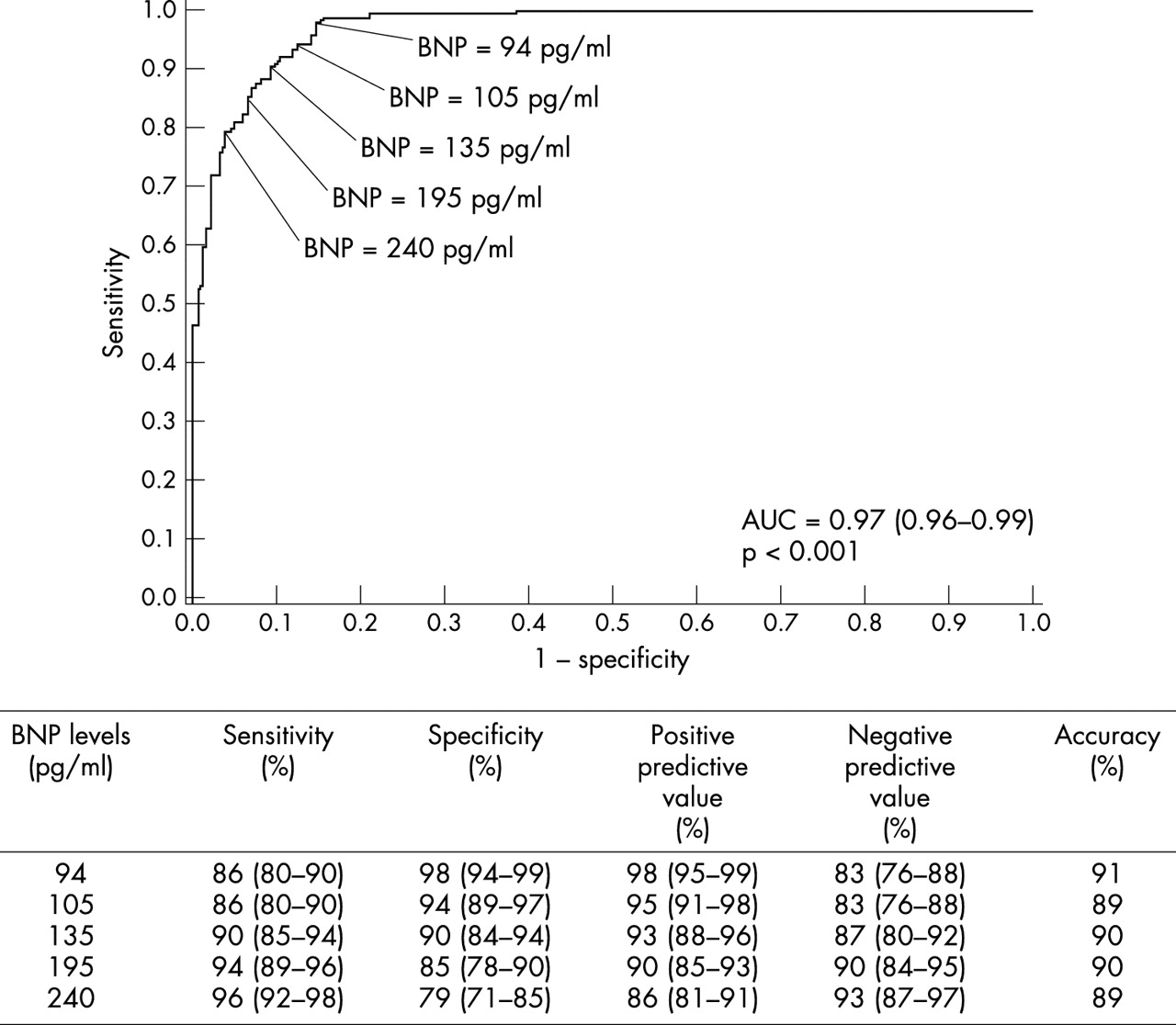
ROC comparing sensitivity and specificity of brain natriuretic peptide (BNP) differentiating chronic cardiac failure (CCF) versus non-CCF.34
RELATIVE DISADVANTAGES OF HAND HELD ECHOCARDIOGRAPHY AND PLASMA BNP FOR SCREENING FOR LVSD
Performing and interpreting echocardiography requires training. The degree of training required for point-of-care physicians to reliably assess LVSD using a hand held echocardiography device has not been systematically addressed. This issue is now being discussed by the British Society of Echocardiography. The examination is also relatively time consuming and a hand held echocardiography device entails at least a capital cost of £10 000. On the other hand, estimation of plasma BNP requires only a blood test and at present may be reliably assessed using a bedside kit.35 However, there are factors confounding interpretation of the results. Both BNP and NT BNP appear to rise with plasma creatinine, female sex, and age independently of LVEF36; thus, age and sex specification cut-off may be required and renal failure ruled out before development of large scale screening programmes. Furthermore, other studies have found natriuretic peptides to be less useful in differentiating normal from abnormal LVSD in high risk patients compared to the population as a whole.39 McClure and colleagues found that although plasma BNP values did predict severe LVSD following acute myocardial infarction, it only poorly predicted those with mild but definite LVSD who would have benefited from treatment.37 Loop diuretics may also confound plasma BNP estimation to predict LVSD.38 Finally, for cost effective screening for LVSD, a test in addition to having a high negative predictive value should also have good positive predictive values. The positive predictive value of plasma BNP is low for screening a general population for LVSD.35,39 On the other hand, hand held echocardiography has excellent negative and positive predictive values for both low and high risk populations for screening of LVSD.21
However, studies are required to assess the relative cost effectiveness of hand held echocardiography and plasma BNP to screen low and high risk subjects for LV systolic dysfunction in the community. Figure 5 summarises various approaches to establishing LVSD in a high risk patient. However, it may be hypothesised that the most cost effective strategy would be initial plasma BNP estimation which may rule out LVSD, but those with high BNP values may undergo hand held echocardiography to establish the presence of LVSD. A study from our team is ongoing to address this hypothesis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient pathways for diagnosis of left ventricular systolic dysfunction. BNP, brain natriuretic peptide; MI, myocardial infarction; NT BNP, N terminal pro-brain natriuretic peptide.