Article Text

Statistics from Altmetric.com
In this issue of Heart we have the opportunity to enjoy the results of a study on sudden cardiac arrhythmic death coming from a group with a longstanding experience in the diagnosis and treatment of this condition.1 Since the recognition of the genetically determined disease now known as “Brugada syndrome”,2 a lot of effort has been dedicated to understanding the pathophysiologic basis and prognosis of this and other primary electrical diseases of the heart. Viskin and colleagues now provide us with an additional and very important piece of information. By comparing a group of patients with the disease to a sufficiently large control group of individuals, they show that the ECG is a powerful tool to recognise patients with this syndrome. Because this disease causes sudden arrhythmic death, the consequences of the diagnosis are very important.
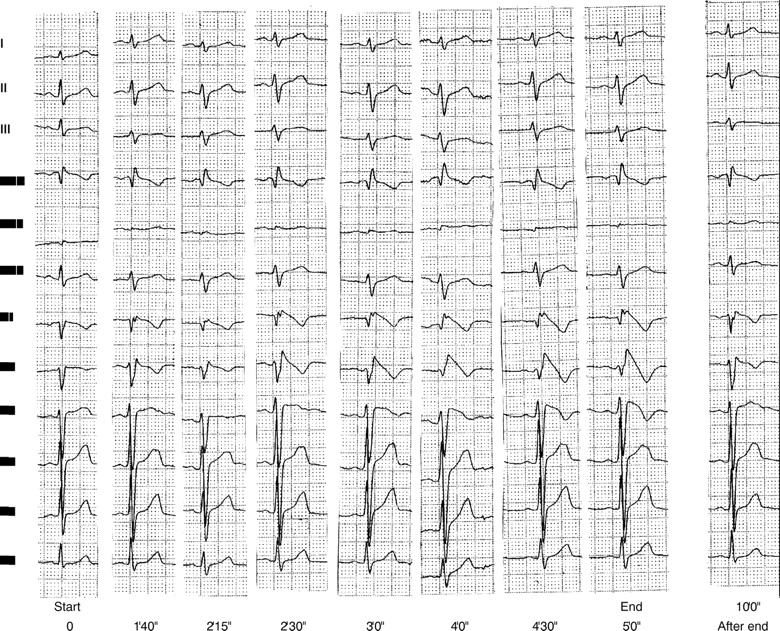
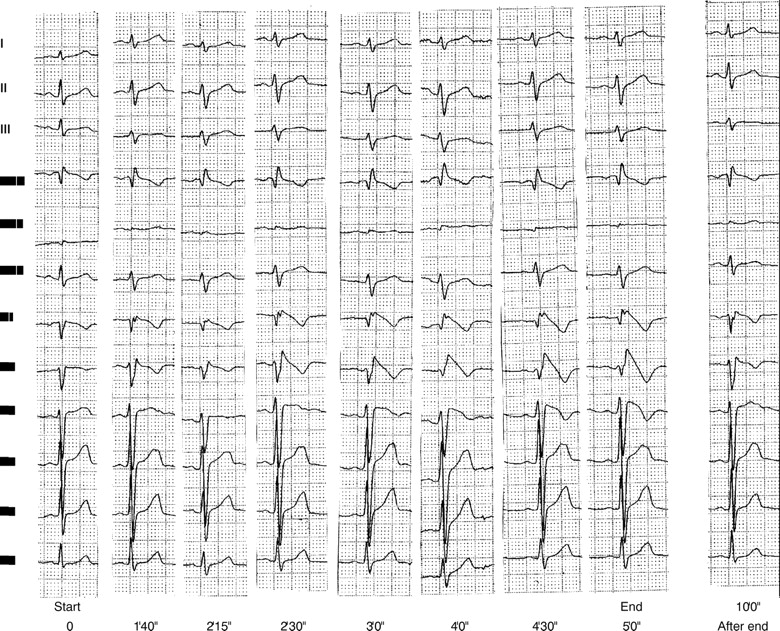
Symptomatic individuals must be protected with an implantable cardioverter defibrillator (ICD). No other proven effective treatment is known. Asymptomatic individuals who carry the disease remain a very difficult problem. At present, we recommend invasive investigation and implantation of an ICD in inducible patients. This is based on the fact that asymptomatic individuals may become symptomatic during follow up,3 and also on the observation that many symptomatic individuals have been found to have an abnormal ECG years before the symptoms developed. Thus, whether a patient is classified as symptomatic or asymptomatic seems more a question of the timing of the diagnosis than of the disease itself. Relatives have to be screened for the syndrome. A normal 12 lead ECG is not sufficient to exclude the diagnosis. The individuals have to be screened by means of pharmacologic testing with an intravenous sodium channel blocker like ajmaline (fig 1) or flecainide. The disease is inherited as an autosomal dominant trait in about 30% of families. In 20% of cases no clear pattern of inheritance can be defined. The remaining 50% of cases are sporadic, suggesting a “de novo” mutation (P Brugada, unpublished observations, 2000). Blood samples must be drawn for genetic analysis.
{kind=link}
Effects of intravenous administration of 50 mg ajmaline over a five minute period in a patient with the concealed form of the Brugada syndrome. Note the rapid appearance of the typical ECG in leads V1–V3. Ten minutes after stopping the injection the ECG has almost returned to normal. Paper speed 25 mm/s.
Because of these hereditary aspects, missing the diagnosis in a symptomatic individual also has important consequences. Classifying someone as having “idiopathic” ventricular fibrillation means that family members will not be screened for Brugada syndrome, which may result in medicolegal complications if another (near) sudden death occurs in the family.
The most important conclusion of the study by Viskin and colleagues is, however, that patients with syncope of unknown origin should be pharmacologically tested for Brugada syndrome, a suggestion made by the authors on the basis of their results.1 We have long ago incorporated pharmacologic challenge with a sodium channel blocker as one of the studies performed in patients with syncope of unknown cause. The same holds for idiopathic atrial fibrillation, because up to one third of patients with the Brugada syndrome may manifest paroxysmal atrial fibrillation alone or in combination with episodes of ventricular fibrillation.4
Whether spontaneously abnormal, or only abnormal after the administration of a sodium channel blocker, a “Brugada ECG” is a marker for sudden cardiac death. This diagnosis should not be missed.
Acknowledgments
Supported in part and equally by the Cardiovascular Research and Teaching Institute Aalst, Belgium, the Mapfre Medicine Foundation, Spain, and the Ramon Brugada Senior Foundation, Belgium, Spain, and USA.