Article Text

Statistics from Altmetric.com
Mitral valve surgery has changed considerably in the past decades and is now indicated mostly for pure or predominant mitral regurgitation. This is the result of the regression of rheumatic disease, of the efficacy of mitral balloon valvuloplasty for mitral stenosis, and of the aging of the population with increasing degenerative or ischaemic disease causing mitral regurgitation. Mitral regurgitation can be “organic” (that is, caused by intrinsic mitral disease such as rheumatic disease, ruptured chord, perforation of leaflet) or be “functional” (that is, where a normal valve regurgitates because of ventricular dysfunction).
The timing of mitral surgery has remained one of the most vexing problems of clinical cardiology because symptoms can remain absent or minimal despite severe regurgitation caused by adaptive remodelling of left ventricle and atrium, or because of patient adaptation to the disease. However, recent advances in the understanding of the natural history of the disease and of the impact of left ventricular dysfunction on outcome, in the echocardiographic evaluation of mitral diseases and in the risk and success of mitral repair, have resulted in a widespread evolution towards earlier surgery.
POOR OUTCOME OF SEVERE MITRAL REGURGITATION
Mitral regurgitation is a progressive disease
The new quantitative techniques have allowed the progression of mitral regurgitation to be defined. As was clinically suspected, mitral regurgitation is a progressive disease,1 with an increase on average of 7.5 ml per year for regurgitant volume and of 5.9 mm2 per year for the effective regurgitant orifice. The determinants of progression are anatomic changes, with more rapid progression in patients with mitral valve prolapse, in particular new flail leaflet, and in patients with an enlarging mitral annulus.1 Importantly, progression is not uniform and if half of the patients see notable progression, 11% see also spontaneous regression of mitral regurgitation, related to improved loading conditions. The progression of mitral regurgitation also causes progression of left ventricular remodelling leading to the development of left ventricular dysfunction.2
The worrisome natural history of severe mitral regurgitation
Widely disparate estimates of long term survival in patients with mitral regurgitation—between 97–27% at five years—have been reported.3,4 We analysed the natural history of mitral regurgitation caused by flail leaflets because these patients present with severe mitral regurgitation in more than 85% of cases.5 We observed that, in comparison to the expected survival, an excess mortality was noted (6.3% yearly) (fig1). A high morbidity was also present with a 10 year incidence of atrial fibrillation of 30%, and of heart failure of 63%. Furthermore, at 10 years 90% of patients were either dead or had undergone surgery, which means that the operation is almost unavoidable. Patients with New York Heart Association (NYHA) functional class III or IV symptoms, even transient, displayed a considerable mortality (34% yearly) if not operated upon, but even those in class I or II had a notable mortality (4.1% yearly). Patients with ejection fraction < 60% also displayed an excess mortality as compared to those with ejection fraction ≥ 60%, but no group at very low risk under medical treatment could be defined.

Survival in patients with medically treated mitral regurgitation caused by flail mitral leaflets. Note the excess mortality as compared to the expected survival (red screen). Reproduced from Ling et al, N Engl J Med 1996;335:1417–23, with the authorisation of the Massachusetts Medical Society.
Sudden death is a catastrophic event, responsible for approximately a quarter of the deaths occurring under medical treatment.6 The determinants of higher rates of sudden death are mostly severe symptoms and reduced ejection fraction, but most sudden deaths occur in patients with no or minimal symptoms and normal left ventricular function.6 The rate of sudden death is 1.8% per year overall; even in patients without risk factors it is 0.8% per year. These data underscore the serious prognostic implication of severe mitral regurgitation, suggesting that surgery should be considered early in the course of the disease.
Left ventricular dysfunction: frequent and poorly predictable
How to assess left ventricular function in mitral regurgitation is the subject of an ongoing debate and research. The increased diastolic inflow volume increases preload. During systole, the regurgitant flow towards the left atrium suggests a decreased impedance to ejection, but end systolic wall stress is usually normal. Multiple methods of correction of the measured left ventricular function indices have been suggested, showing that there is no wide consensus on how to measure intrinsic left ventricular function in mitral regurgitation.
Clinically, left ventricular dysfunction is a major source of poor outcome under conservative management5 or postoperatively.7 Although it currently represents a rare cause of perioperative death due to the progress of anaesthesia and myocardial protection, it is the most frequent cause of late death after surgery.7 The ejection fraction decreases significantly immediately after surgical correction of mitral regurgitation by approximately 10%.2 Therefore, despite symptomatic improvement, postoperative left ventricular dysfunction (ejection fraction < 50%) is frequent, occurring in close to a third of the patients successfully operated upon for organic mitral regurgitation. Postoperative left ventricular dysfunction is associated with poor survival2,8 and high but delayed incidence of heart failure.9
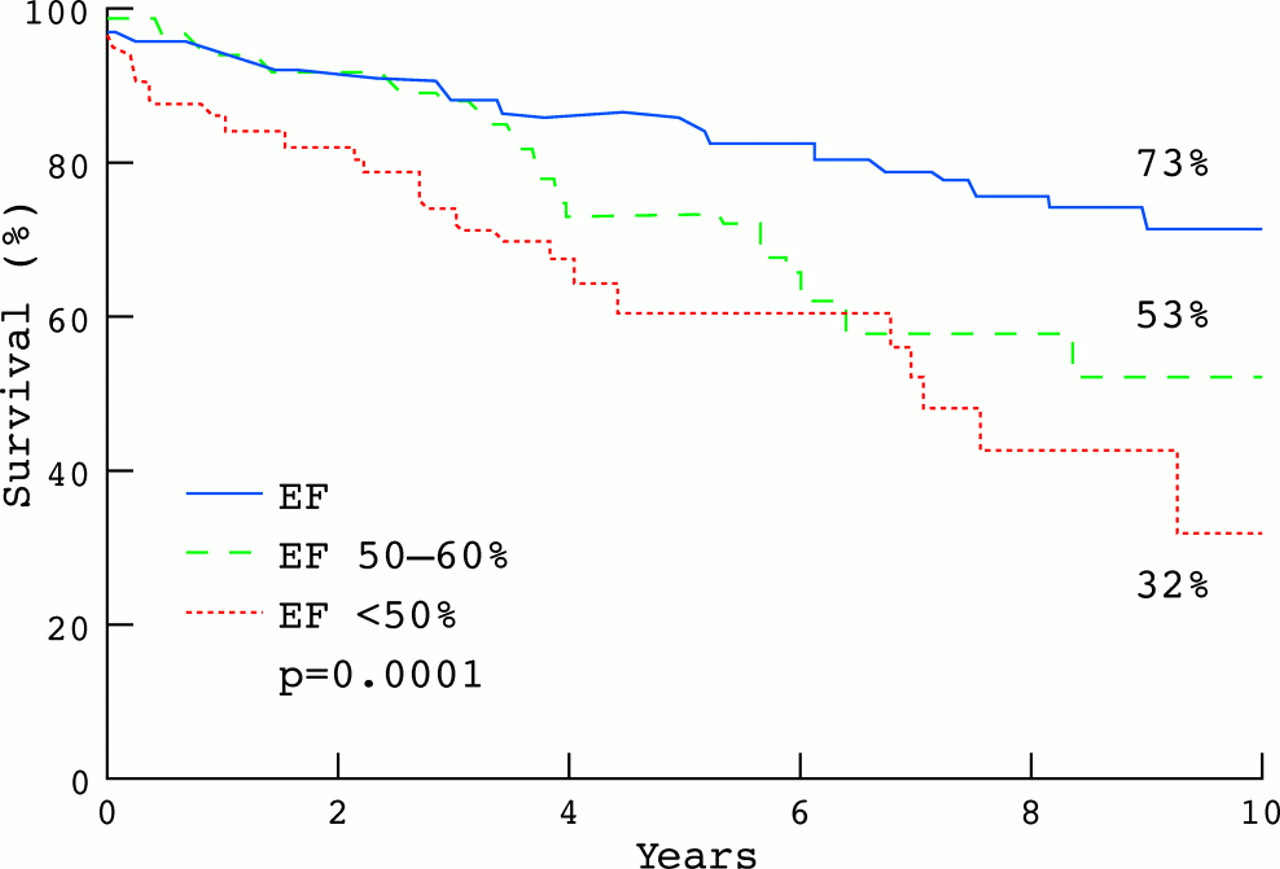
Preoperative ejection fraction is the best predictor of long term mortality under conservative management5 and after surgery7 (fig 2), of congestive heart failure,9 and of postoperative residual left ventricular function.2 The end systolic dimension is also a significant predictor of the postoperative left ventricular function.2 Therefore, either an ejection fraction < 60% or an end systolic diameter ≥ 45 mm are considered as demonstrating overt left ventricular dysfunction and should be immediately considered for surgery in the absence of major comorbidities.10

Long term postoperative survival according to the preoperative echocardiographic ejection fraction. Note the excess mortality in patients with ejection fraction < 50% but also with “low normal” ejection fraction 50–59%. Reproduced with the authorisation of the American Heart Association.
However, reduced left ventricular function, even pronounced, should not be considered as a contraindication to surgery in patients with organic mitral regurgitation, because operative mortality is not excessive is these patients7 and because the postoperative clinical complications are often delayed after surgery. Also, the precision of the prediction of outcome is imperfect, with a relatively wide range of error for the prediction of postoperative left ventricular function.2,8,11 As the best outcome is observed in patients with an ejection fraction ≥ 60%, this stage of the disease appears to represent the best opportunity for surgery. Therefore, the concept of waiting for signs of early decline of left ventricular function is rigged with a notable risk of “unexpected” left ventricular dysfunction,2 and appears defensible mostly when the mitral regurgitation is not severe enough to warrant immediate surgery, the operative risk is high, or the chances of a valve repair are low.
Ischaemic mitral regurgitation: a group at high risk
The high risk associated with ruptured papillary muscle is well known.12 After a myocardial infarction, mitral regurgitation can develop without ruptured papillary muscle as a consequence of left ventricular remodelling, due to the apical and inferior displacement of the papillary muscles leading to incomplete coaptation of tenting leaflets.13 The strong impact of this “functional” mitral regurgitation on the outcome postmyocardial infarction has been underscored in two recent studies, showing that its mere presence is associated with poor survival.14,15 Quantitative measurements show that higher degrees of regurgitation are associated with worse outcome independently of the ejection fraction.15 Therefore, even though the murmur may not be loud,16 an aggressive surgical approach should be considered in these patients.
MITRAL SURGERY: RECENT PROGRESS
The operative risks, results, and improvements are essential considerations in the appraisal of the timing of surgery.
The operative mortality is of considerable importance but was too high to consider surgery in asymptomatic patients in the past. However, for patients with organic mitral regurgitation, operative mortality has considerably decreased recently,17 and in our institution is currently around 1% in patients younger than 75 years whether repair or replacement is performed.7 Conversely, the operative mortality in patients ≥ 75 years old, or in patients operated on for ischaemic mitral regurgitation, although improved recently, remains relatively high, between 3.5–12% depending on the preoperative presentation.18
The availability of valve repair is of crucial importance. Previous studies suggested a lower operative mortality and a better long term survival after valve repair than replacement,19–21 but it was unclear whether this was due to a better preoperative condition of patients undergoing valve repair or to the procedure itself. In our experience, taking into account all differences at baseline between valve repairs and replacements, valve repair is indeed an independent predictor of a better outcome after surgery for mitral regurgitation, with a lower operative mortality and a better long term survival than valve replacement.22 This benefit is noted whether or not an associated coronary bypass surgery is performed.22 A major reason for the improved outcome after valve repair is a better left ventricular function than after valve replacement.22 The conservation of the subvalvar apparatus certainly plays a role in the preserved left ventricular function after valve repair, as it does after valve replacement without transsection of chordae. The improved survival after valve repair is not accomplished at the expense of an increased risk of reoperation.22
Intraoperative transoesophageal echocardiography is an essential component of the success of valve repair and should be performed by experienced physicians, to monitor the repair procedure and help with intraoperative decisions.23
Therefore, valve repair has become extremely popular24 and currently a successful repair can be performed in 85–90% of patients with isolated mitral regurgitation. This high percentage of repair has been achievable after the initial learning phase of this difficult procedure through the utilisation of special techniques, such as the transposition of chordae or insertion of artificial cords, in particular for the rupture chords of the anterior leaflet.25,26 However, the repairability of rheumatic lesions is not as consistent as that of degenerative lesions.27 Despite these high feasibility rates, the repair of the mitral valve should not be considered as a panacea and does not eliminate the risk of myocardial dysfunction. In patients with an ejection fraction < 60%, an excess mortality is noted whether repair or replacement is performed.22 Therefore, the ability to perform repair in a high percentage of patients should be considered as an incentive to perform surgery because of its low risk and good survival, and not as an incentive to delay surgery and encounter the risk of more left ventricular dysfunction.
OUTCOME AFTER SURGICAL CORRECTION OF MITRAL REGURGITATION
To make appropriate decisions, it is important to analyse the postoperative outcome, in particular the implications of delaying surgery until overt alterations occur.
Waiting for left ventricular dysfunction (ejection fraction < 60%, end systolic diameter ≥ 45 mm) imposes an excess rate of mortality7 and of heart failure9 compared to patients with more normal function at surgery.
Waiting for severe symptoms to occur before surgery is also not benign. In the Mayo experience, the more severe the preoperative symptoms were, the lower the postoperative ejection fraction2 and the higher the incidence of congestive heart failure9 were during follow up. Adjusting for age at surgery and all other determinants of outcome, severe preoperative symptoms are associated with a worse long term survival18,28 and excess incidence of heart failure.9 Even in the privileged subgroup of patients with an ejection fraction ≥ 60% where the survival is not different from the expected survival, patients operated at an early stage with minimal symptoms have a better survival than patients with severe symptoms.7 Therefore, waiting for severe symptoms is associated with a higher incidence of complications after the surgery is performed (fig 3)
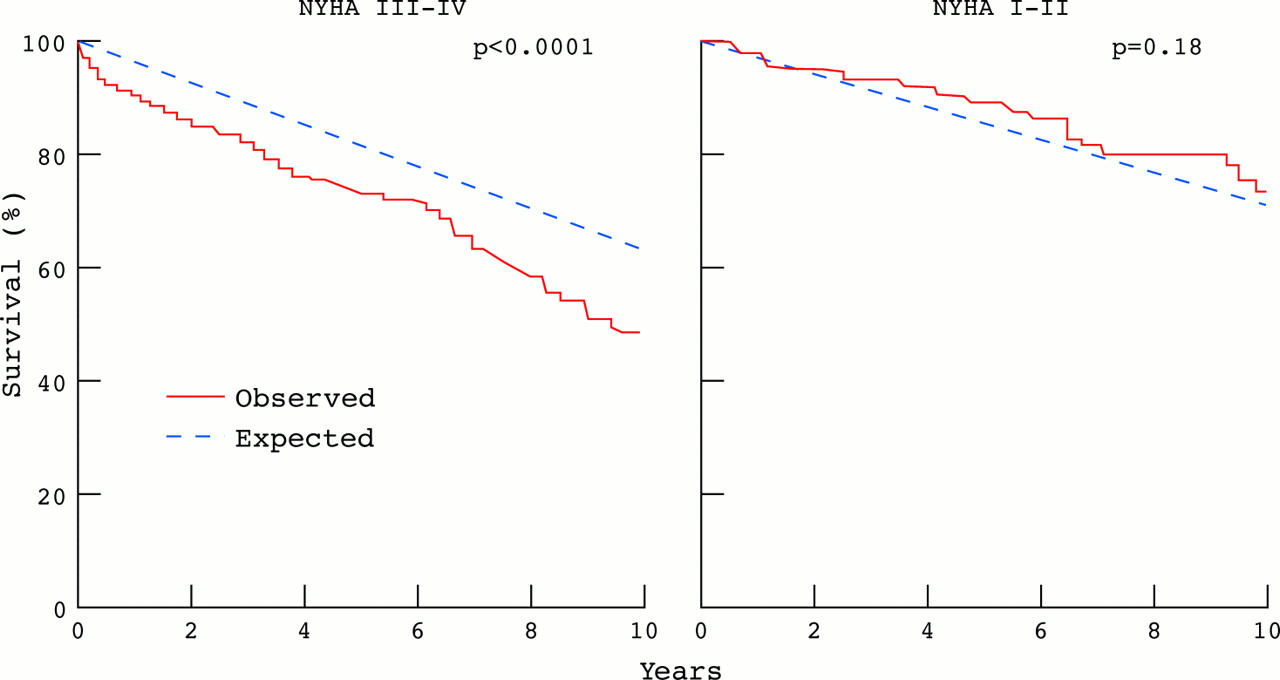
Comparison of observed and expected survival after surgical correction of mitral regurgitation separately in patients preoperatively with severe symptoms (left graph) and no or minimal symptoms (right graph). There is excess mortality in patients operated on with severe symptoms but no excess mortality in patients who had no or minimal symptoms, suggesting that in the latter group the long term consequences of mitral regurgitation have been suppressed. Reproduced with the authorisation of the American Heart Association.
Waiting for atrial fibrillation to occur and persist more than three months before surgery was associated with a high risk of postoperative persistence of atrial fibrillation and therefore of requiring long term anticoagulation. Conversely, recent atrial fibrillation tends to revert to sinus rhythm postoperatively.29 Therefore, waiting for chronic atrial fibrillation preoperatively is associated with residual postoperative morbidity.
There is no randomised trial comparing the outcome after early surgery for organic mitral regurgitation to the outcome with medical management. In patients with flail mitral leaflets the long term outcome after early surgery was compared to that of patients managed conservatively and operated on whenever it was judged necessary. Although many patients initially treated conservatively eventually underwent surgery, the early surgical approach was associated with an improved long term survival through a pronounced reduction in cardiac mortality, and a decreased morbidity (less heart failure and less atrial fibrillation) during follow up.30 These results underline the potential for eliminating most of the cardiac complications caused by mitral regurgitation through an early surgical approach as long as the operative mortality remains low (< 2%).
WHAT INFORMATION IS NEEDED TO DEFINE THE TIMING OF MITRAL SURGERY?
Symptoms
The severity of symptoms is defined by history but as many patients limit progressively their physical activity, performing exercise testing in “asymptomatic” patients,31 in particular with oxygen consumption measurement, may unveil unexpected exercise limitations.
Left ventricular function
Left ventricular function is usually assessed by echocardiography. An ejection fraction < 60% or left ventricular end systolic diameter ≥ 45 mm are considered as signs of overt left ventricular dysfunction.
Degree of mitral regurgitation–haemodynamics
Although the extent of the jet of mitral regurgitation by colour flow imaging or the density of dye in the left atrium by angiography are useful to observe, these methods have numerous pitfalls.32,33 The comprehensive assessment of the degree of mitral regurgitation can be performed by quantitative Doppler echocardiography. The most widely used method of quantitation of mitral regurgitation is the PISA method, based on the analysis of flow convergence region proximal to the regurgitant orifice.34,35 The Doppler measurement of mitral and aortic stroke volumes is also useful but more cumbersome to master.36 Both methods allow calculation of the regurgitant volume (RVol) and effective regurgitant orifice (ERO).37 The respective thresholds for severe mitral regurgitation are ≥ 60 ml for RVol and ≥ 40 mm2 for ERO. Haemodynamics can also be characterised by measuring the cardiac output by Doppler and the right ventricular systolic pressure by use of the tricuspid regurgitant velocity.
Aetiology–repairability
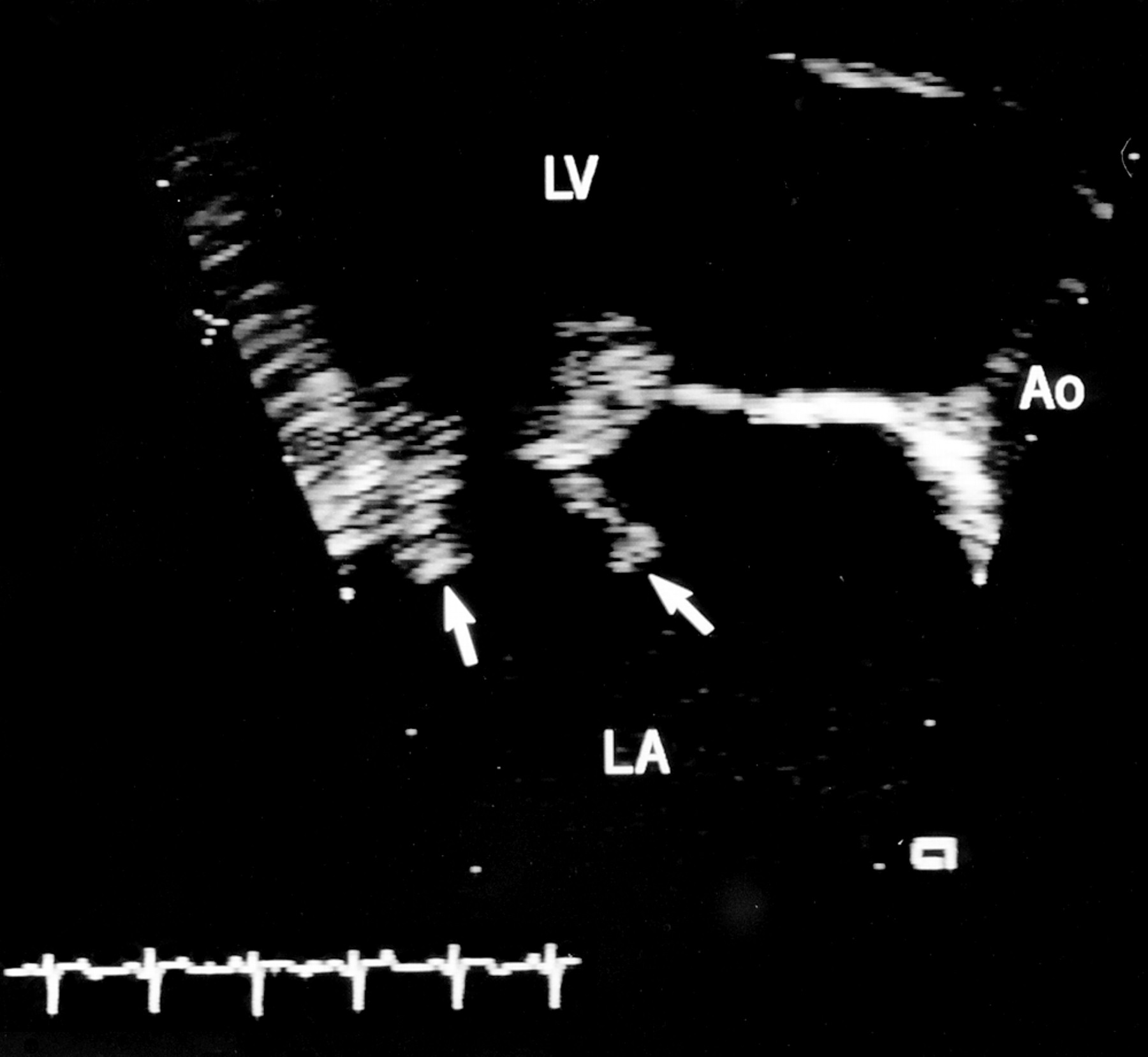
The mitral lesions can be reliably defined by echocardiography (fig 4),38 and usually transthoracic echocardiography is sufficient but when imaging is mediocre, transoesophageal echocardiography can be helpful (fig 5).38 Rheumatic lesion or massive calcifications of the valve or annulus are often difficult to repair and in the vast majority of cases mitral prolapse is repairable. The repairability is highly dependent on the skills and experience of the surgeon and should be defined based on both patient and institution based criteria. New methods have extended the field of application of repair, particularly with anterior leaflet flail segments,26 but if local experience is limited, it is important to refer patients to centres with more extensive experience.

Echocardiographic long axis apical view of the left atrium with colour flow imaging of the jet of mitral regurgitation in a patient with flail posterior leaflet. Note the eccentric jet occupying only a portion of the left atrium despite the severe regurgitation with a large proximal flow convergence.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Transoesophageal echocardiographic view of the left atrium (LA), left ventricle (LV) and aorta (Ao) in a patient with bileaflet mitral valve flail segments (arrows) and ruptured chordae.
Information needed to determine timing of mitral surgery
-
Symptoms or signs of heart failure, if unclear exercise test
-
Left ventricle:
-
left ventricular function (ejection fraction, end systolic diameter)
-
-
Left atrium:
-
atrial fibrillation?
-
size
-
-
Haemodynamics:
-
pulmonary hypertension (Doppler—rarely catheterisation needed)
-
-
Degree of mitral regurgitation:
-
clinical examination: intensity of murmur, thrill, S3
-
quantitative Doppler echocardiography, if inconclusive
-
transoesophageal echocardiography or angiography
-
-
Repairability:
-
aetiology, mechanism
-
calcifications, anterior leaflet involvement
-
surgeon's skills
-
-
Surgical risk:
-
age
-
heart failure
-
comorbidity
-
Surgical risk
The operative risk is mostly determined by age ≥ 75 years,7 by the presence of severe preoperative heart failure,18 by the presence of coronary disease,39 and by the severity of comorbid conditions. A composite assessment of the risk is essential for clinical decision making, but the risk in asymptomatic patients ≤ 75 years old is usually low—between 0.1–0.2% in most advanced centres.
TIMING OF SURGICAL CORRECTION OF MITRAL REGURGITATION
The timing of mitral surgery translates into a simple categorical answer when the patient is seen—that is, should we advise the patient to have mitral surgery promptly or should we advise follow up with conservative management? This process can be stratified according to aetiology and severity of mitral regurgitation.
Organic mitral regurgitation
Severe mitral regurgitation: patient has overt symptoms or left ventricular dysfunction
These patients with severe mitral regurgitation with overt severe consequences should be offered surgery, even in relatively high risk patients and irrespective of repairability of the mitral valve. Although surgery performed with this type of presentation results in symptomatic improvement, it is associated with notable excess postoperative risk,7,18 but the postoperative outcome is far better than the outcome under medical treatment.5
Severe mitral regurgitation: patient has neither overt symptoms nor left ventricular dysfunction
Irrespective of repairability, some recent events before the visit are a strong incentive to propose surgery immediately: atrial fibrillation, even paroxysmal, ventricular tachycardia at rest or during exercise, or the observation of pulmonary hypertension by echocardiography are such events.10
With low probability of repair, patients are usually not referred to surgery if there are no clinical risk factors. However, patients with a massive degree of mitral regurgitation (regurgitant volume ≥ 100 ml/beat) or with pronounced left atrial enlargement may be considered for surgery if at low risk for surgery.
With high probability of valve repair, our approach,30 and the current guidelines,10 have become much more aggressive towards surgery, even if there are no symptoms or signs of left ventricular dysfunction, if the operative risk is low. This aggressive approach will require a randomised clinical trial in the future to define the magnitude of its benefit.
Mitral regurgitation not severe
For regurgitant volumes < 45 ml/beat there is almost never a need for surgery; furthermore, there is concern that a failed repair attempted during another cardiac operation (such as bypass surgery needed for angina) may result in worse mitral regurgitation than originally present.
For regurgitant volumes 45–60 ml/beat, there is usually no need for immediate surgery but in certain rare circumstances mitral surgery may be indicated. These involve valves that are repairable and patients who need a cardiac operation for a MAZE procedure, or bypass surgery or another valve operation. In some patients with mitral valve prolapse and ventricular tachycardia at rest or with exertion we have indicated a mitral valve repair to suppress the volume overload. The comparison of a surgical approach to medical treatment and even the determination of the benefit of medical treatment under those circumstances remains to be defined.10
Ischaemic mitral regurgitation
The timing of surgery in ischaemic mitral regurgitation is more complicated than in organic mitral regurgitation because the definition of what is severe mitral regurgitation (that is, mitral regurgitation with severe vital consequences) is different from organic mitral regurgitation. Indeed, patients with an ERO ≥ 20 mm2 (and not ≥ 40 mm2 as in organic mitral regurgitation) incur a notable excess mortality.15 Also, despite the fact that repair is often possible, the risk of surgery is higher than in organic mitral regurgitation and still represents a limitation to early surgery.
When coronary bypass grafting surgery is deemed necessary and mitral regurgitation is present, recent data suggest that patients with ERO ≥ 20 mm2 should be offered mitral repair. It is uncertain whether patients with trace mitral regurgitation but ERO < 20 mm2 may benefit from repair.
When coronary bypass grafting surgery is deemed not indispensable but possible, a previous history of heart failure, the presence of viable myocardium, and mitral regurgitation ≥ 20 mm2 all argue in favour of mitral surgery combined with revascularisation.
When coronary bypass grafting surgery is deemed not to be feasible, the indications of mitral surgery are more restrictive and frank symptoms, lack of diffuse myocardial scars, and a frank volume overload with regurgitant volume ≥ 45–50 ml appear all minimal considerations for mitral surgery. The choice of performing cardiac transplantation is to be discussed.
Therefore, the timing of mitral surgery has changed considerably from a relatively passive response to the development of severe symptoms, to an early surgery concept preceding the signs of left ventricular dysfunction. The early surgery approach requires a high repair rate and a low operative mortality; therefore currently not all patients and not all institutions are candidates to apply the early indications of surgical correction of mitral regurgitation. Nevertheless, considerable progresses have recently been accomplished for the assessment and treatment of mitral regurgitation and surgery should be considered early in the course of the disease, when severe regurgitation has been diagnosed.
Aetiology and mechanism of mitral regurgitation
Timing of surgery in organic mitral regurgitation
Timing of surgery in ischaemic mitral regurgitation
REFERENCES
Footnotes
-
Copyright 2002 Mayo Foundation
Linked Articles
- Miscellanea
- Miscellanea
- Miscellanea