Article Text

Statistics from Altmetric.com
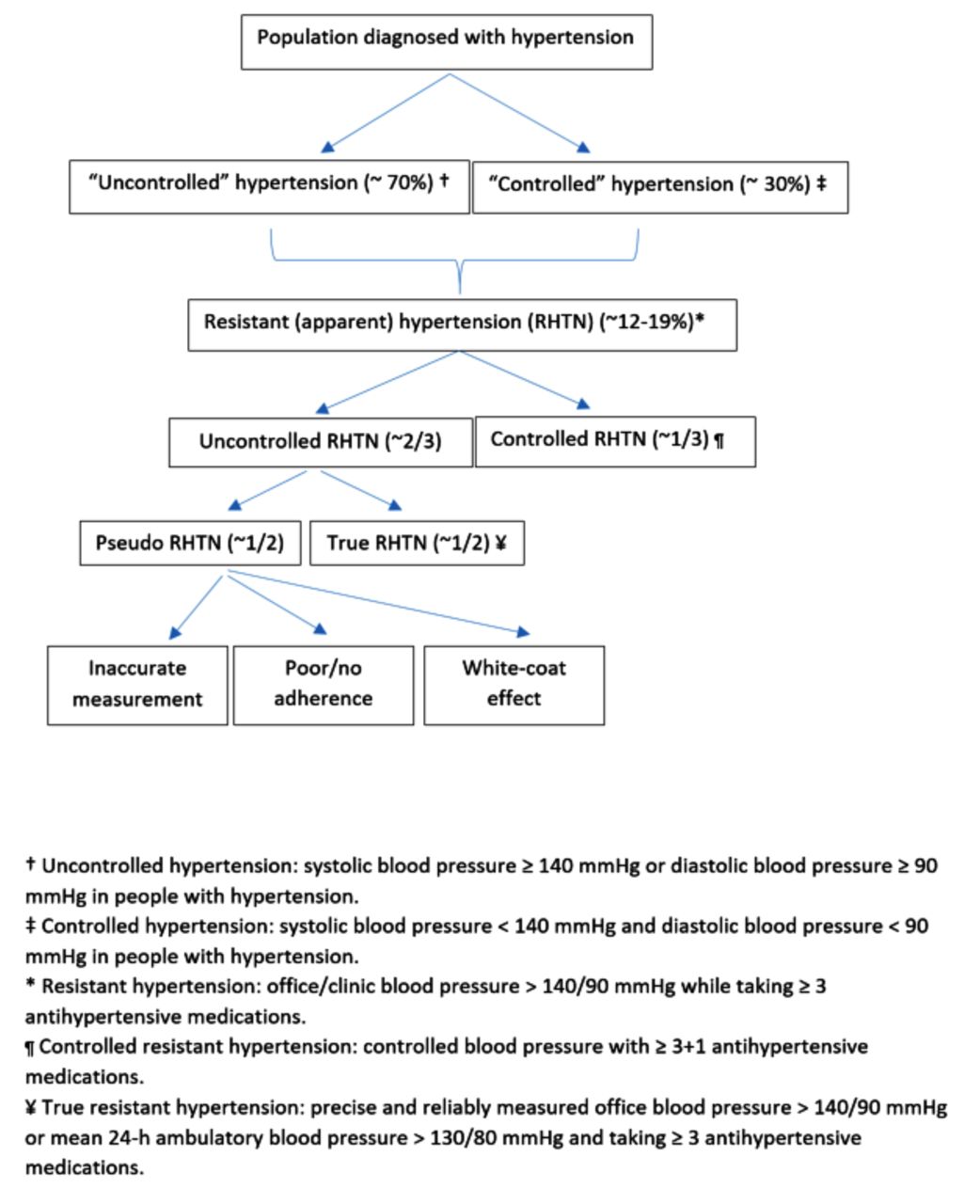
Hypertension is one of the most prevalent conditions in the world. Despite evidence of the beneficial effects of blood pressure (BP)-lowering across a range of patient groups,1 treatment and control rates remain suboptimal in high-income and low-income countries alike.2 To alert physicians to the fact that some patients with hypertension might benefit from specialist assessment for possible underlying causes or more advanced treatment recommendations, clinical practice guidelines introduced a new subcategory of hypertension called resistant hypertension (figure 1). The European Society of Cardiology (ESC) guidelines defined resistant hypertension as the failure to achieve BP ‘control’ to levels below 140/90 mm Hg despite treatment with three antihypertensive medications with complementary mechanisms of action (with at least one diuretic).3 The American Heart Association (AHA) guidelines adopted an extended definition to also include patients with four or more antihypertensive medications, even when BP was controlled.4 To acknowledge the fact that an ‘apparent’ resistant hypertension might turn out to be spurious (because of measurement error, white coat effect or poor patient adherence to treatment), a further subcategorisation into ‘true’ resistant and ‘pseudo’ resistant was made in clinical studies (figure 1).

{kind=link}
Flow chart of the definition of resistant hypertension. Percentages were approximately estimated from epidemiological studies conducted in the UK and the USA.
In their Heart manuscript, Noubiap et al 5 report the findings of a meta-analysis that estimates the prevalence of apparent resistant, true resistant and pseudo-resistant hypertension among patients with treated hypertension. By including 91 cohort or cross-sectional studies with over 3.2 million patients with hypertension in total (most of them from high-income countries), they estimated the prevalence of resistant hypertension across different geographical regions. Overall, the unadjusted prevalences of apparent resistant, true resistant and pseudo-resistant in the entire population of patients with treated hypertension were 14.7%, 10.3% and 10.3%, respectively. However, more important than the absolute estimates reported, the significant and largely unexplained statistical variability in this meta-analysis highlights the challenges of measurement and interpretation of the burden of resistant hypertension.
One of the main challenges is the definition of resistant hypertension itself. As the systematic review by Noubiap et al 5 reveals, the definitions used to classify patients with apparent resistant hypertension varied substantially between studies, with some adopting the AHA and others the ESC definition. Some of the studies were based on selected patient populations and might not have been representative of the treated or total hypertensive population. Thus, it is perhaps not very surprising that estimates for resistant hypertension ranged from 5% to 35% in the identified studies. Relatedly, the overall pooled estimate of 14.7% is likely to be even less reliable when put in the context of the recently changed AHA guidelines, which have lowered the threshold for resistant hypertension to 130/80 mmHg.6 This, together with recent evidence from clinical trials suggesting that a strategy of combining multiple classes of antihypertensives at low doses might yield better BP reductions than the conventional approach of maximum uptitration of fewer agents,7 seems to have made obsolete the concept of labelling patients to have resistant hypertension simply because they are prescribed three or four antihypertensives.
As Noubiap et al 5 point out, it is more important to know the true prevalence of resistant hypertension after pseudo-resistance has been excluded than to have an overall estimate of apparent resistant hypertension. However, only 12 studies involving about 75 000 individuals were identified that had reported the prevalences of true resistant and pseudo-resistant hypertension, and these were mainly hospital-based and relied on office-based BP measurements. Not only was the range of estimates among studies very wide, but the proportion of patients having pseudo-resistant versus true resistant hypertension was very different among the studies included. For instance, in some studies two-thirds of the patients had pseudo-resistant hypertension and in others the proportions were reversed, with over two-thirds having true resistant hypertension (see figure 2 of the paper). Accurate determination in clinical practice and research studies of whether resistant hypertension is actually attributable to ‘a refractory disease or a refractory patient’8 is complex and not always possible. Surveys such as that conducted by Tomaszewski et al 9 using high-performance liquid chromatography-tandem mass spectrometry urine analysis showed that at least a quarter of patients did not comply with BP-lowering treatments. Thus, the prevalence of true treatment resistance is also likely to change as more sophisticated methods for exclusion of pseudo-resistance are adopted.
In conclusion, Noubiap et al 5 remind us that resistant hypertension affects a sizeable proportion of patients with treated hypertension, and about half of them have true resistant hypertension that requires more aggressive BP management to avoid the deleterious consequences of persistently elevated BP. The study also reveals that the concept of resistant hypertension, particularly ‘controlled’ resistant hypertension and the number of drugs used, may deserve to be revised in keeping with the recent decrease in diagnostic thresholds and multidrug low-dose treatment recommendations for hypertension.
Footnotes
Contributors All authors contributed to drafting and have approved the final manuscript.
Funding The authors acknowledge funding by NIHR Oxford BRC and Oxford Martin School.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Commissioned; internally peer reviewed.