Article Text

Statistics from Altmetric.com
Patients with a dilated thoracic aorta are at risk for aortic complications such as aortic dissection or rupture. While these aortic complications result in high mortality rates, aortic dilatation often remains asymptomatic for a long period of time. Therefore, identification and treatment of individuals with a dilated aorta is of paramount importance. This is specifically relevant given that the diagnostic techniques and therapeutic options are available. Currently, the European Society of Cardiology guidelines define an aorta dilated if the diameter exceeds 40 mm. In addition, preventive surgery is indicated for aortic diameters above 55 mm for both women and men.1
Even though thoracic aortic aneurysms are less prevalent in women as compared with men, the consequences are worse for women. Female patients with an aortic dissection have a poorer surgical outcome and die more frequently than men. Also, the growth rate of a thoracic aneurysm is greater in women as compared with men.2
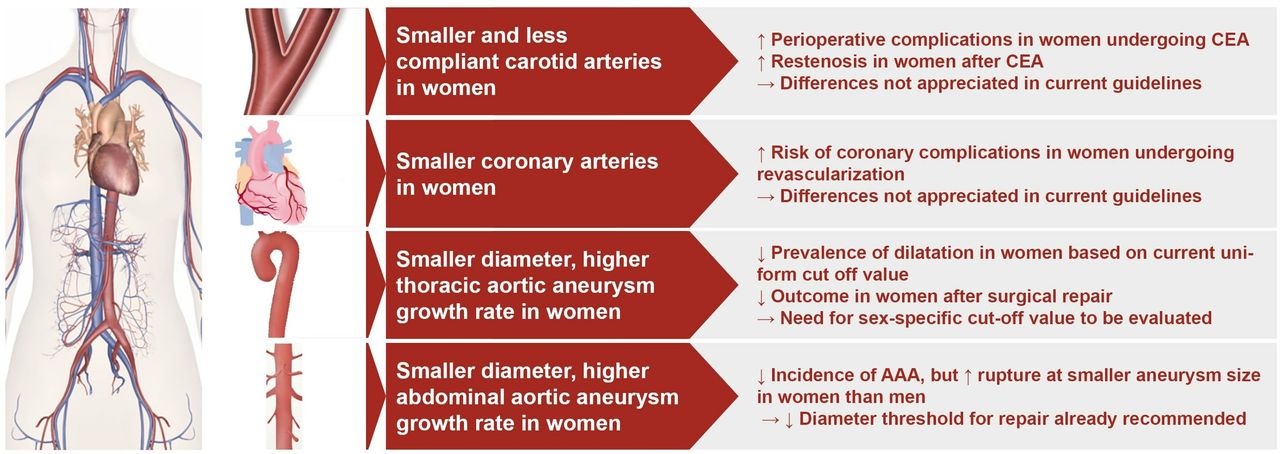
Currently, as medicine advances, personalised medicine has become emerging. The most relevant patient characteristics that have been considered relevant in medicine are age, sex and comorbidities such as diabetes. However, for aortic complications, information on subgroups is limited as data in older patients is sparse, and currently used cut-off values are based on a cohort of relatively young people.3 In addition to lack of data on age, thoracic aortic diameters values have been determined regardless of sex. As a result, one-size fits all cut-off values are used, while the Framingham Heart Study had indicated that age and sex matter for vascular dimensions such as thoracic aortic diameter.4 Since more attention is being paid to sex differences within arterial vascular disease,5 it has been described that women have smaller carotid and coronary arteries6 and have smaller abdominal aortic aneurysms as compared with men (summarised in figure 1). As smaller abdominal aortic aneurysms in women are more prone to rupture,5 the currently used uniform threshold for dilated abdominal aortic aneurysm repair has been under debate.7 For the coronary vasculature, smaller vessels in women have been hypothesised to be one of the underlying reasons for the higher risk of coronary complications in women undergoing coronary artery revascularisation.6 8
{kind=link}
Sex differences in vascular properties and clinical implications.CEA, Carotis endarteriectomy; AAA, Abdominal aortic aneurysm.2 5–8
In their Heart paper, Bons and colleagues report the results of the Rotterdam Study.9 They provide us with population based, sex-specific distributions values of thoracic aortic diameters in the elderly. In addition, they identify relevant determinants for the aortic diameters in men and women. Of the 2505 participants, approximately half is female that allowed for an equally powered study in men and women. The population underwent non-enhanced multidetector computed tomography (CT) to measure ascending and descending aortic diameters. As it is still undecided whether aortic diameters should be evaluated using body surface area (BSA) corrected values or absolute values, the authors assessed both.
The outcome of the study contributes to the overall knowledge on differences between women and men in vascular dimensions. They found absolute values for aortic dimensions to be higher for men as compared with women. These findings are in line with the previously performed study of Rogers et al,4 which evaluated sex-specific aortic diameters by CT values in patients of the Framingham Heart Study and also showed increased absolute diameters in men as compared with women. Interestingly, when BSA-corrected values were assessed, the difference in aortic diameters between women and men reversed with a larger aortic BSA-corrected dimension in women. Therefore, the authors concluded that distribution values should be provided sex-stratified, for both absolute and indexed aortic dimensions. Whether absolute or indexed aortic dimensions are more appropriate to predict aortic complications remains undecided.
Beyond establishment of sex-specific distribution values for aortic dimensions in the Rotterdam Study, the clinical implications are that a dilated ascending aorta, exceeding 40 mm, was common within the elderly of the Rotterdam Study. Even more so in men as compared with women (18.9% in men and 5.9% in women). Yet, a rather low rate of aortic events was observed in both men and women during follow-up, with equal rates. Based on this low event rate in both women and men with dilated thoracic aortic diameters, it is questionable whether the current cut-off value is adequate in elderly and whether sex-specific cut-off values are necessary.
Their findings9 suggest the need to reassess commonly used reference values, considering older age and sex. They provided part of the missing data needed to reassess reference values and inspire future research into the prognostic implications of their findings. In addition, these studies stress the need to carefully stratify data obtained from cardiovascular studies for elderly, women and men. This is a necessary approach to move towards personalised medicine and provide clinical care based on the best available evidence.
Acknowledgments
K.R. Siegersma for provided technical editing of the figure.
Footnotes
Twitter @InnovatieHester
Contributors Conception or design of the work: HMdR and FG. Data collection: FG. Data analysis and interpretation: FG. Drafting the article: FG. Critical revision of the article: FG and HMdR. Final approval of the version to be published: HMdR.
Funding This study was funded by Dutch Heart Foundation (CVON 2017-22 ARGUS).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.
Linked Articles
- Aortic and vascular disease