Article Text

Statistics from Altmetric.com
The avoidable risk of patient harm from a complication in the cardiac catheterisation laboratory (cath lab) remains too high. The causes are often multifactorial, reflecting the complex interaction between operator, patient, team and procedure. Adverse events are typically preceded by missed opportunities for recognition and prevention by members of the team. Safety in the airline industry has been revolutionised by understanding the importance of human factors, encompassing team leadership, structured communication and resource management. Addressing the role of human factors in the cath lab has the potential to improve safety and clinical outcomes.
Adverse events affect approximately 10% of acute inpatients.1 Repeated analyses indicate that errors are rarely a failure of technical ability, but occur due to breakdown of teamwork and communication. In the surgical operating theatre, there is a relationship between the frequency of communication errors and the incidence of adverse events.2 Safety checklists and team briefing are proven interventions to support communication in safety-critical situations.
Safety checklists: from aviation to healthcare
The safety checklist was developed after the Boeing Model 299 crashed on its maiden test flight in 1935, due to a simple pilot error. It acts as a safeguard against lapses in concentration, a reminder to actively review safety-critical steps. The first systematic study of a healthcare checklist was performed in 2004: implementation of a care bundle which included a checklist dramatically reduced the rate of central line infection in the intensive care unit.3
WHO's Surgical Safety Checklist (SSC) was a landmark checklist in medicine.4 Introduction of the checklist was associated with a reduction in surgical complications and mortality.5 The UK National Patient Safety Agency mandated use of the SSC for patients undergoing a surgical procedure from 2009 onwards, and a number of specialties such as interventional radiology have since produced adapted versions.
The reason for the efficacy of the checklist remains unclear. At the most basic level there is a ‘shopping list effect’—a reminder to check, for example, the patient's haemoglobin result, like picking up the milk. This improves the reliability of a process and sets out an expected standard for practice. Perhaps more importantly, checklists modify team behaviour, bringing a focus to patient safety and communication and empowering junior members.6
Checklists in the cardiac catheterisation laboratory
From a human factors perspective, the cardiac cath lab and surgical operating theatre are similar clinical environments, with similar risks to patients. Teams are established in hierarchical and functional roles. Deviations from a predicted pattern are rare, but in an emergency require a rapid and coordinated response. The benefits of safety checklists seen in the operating theatre should also apply to the cath lab.
We surveyed UK cath labs to assess current checklist practice. The majority have a safety checklist, most commonly the SSC or an adapted inhouse version, but its use is inconsistent. Checklist use varies by procedure and is lower in emergencies (eg, ST elevation myocardial infarction). Centres using the SSC are routinely conducting ‘surgical checks’ (eg, anticipated blood loss), which are of arguable relevance to most cases in the cath lab. Very few operators routinely conducted a team brief, regarded as a key component responsible for the efficacy of the SSC.
In summary, current checklist use is patchy and potentially falsely reassuring. This is a problem of design and operation. First, rather than adapting the SSC for cardiology, we need safety checklists specifically designed for use in the cath lab. Under the auspices of the British Cardiovascular Society we have produced a checklist for core invasive cardiac procedures, primarily diagnostic angiography, coronary/structural intervention, pacing and electrophysiology. In turn we describe its design, development and use.
BCS patient safety checklist
Our design aims were: (A) to identify and incorporate key patient safety steps relevant across core cardiology (B) to permit local flexibility in content and operation and (C) to facilitate efficient and rapid checklist completion without compromising the safety content.
We initially reviewed existing cath lab checklists and literature, then produced a comprehensive list of potential safety checks graded by importance. This list was iterated multiple times with involvement from all professional disciplines comprising the cath lab team. Content and design evolved over two rounds of pilot testing, initially in two cardiology centres and then a wider group of five. Feedback and usability was assessed through direct observation and structured interviews, followed by a more general, internet-based survey seeking anonymised content from all users.
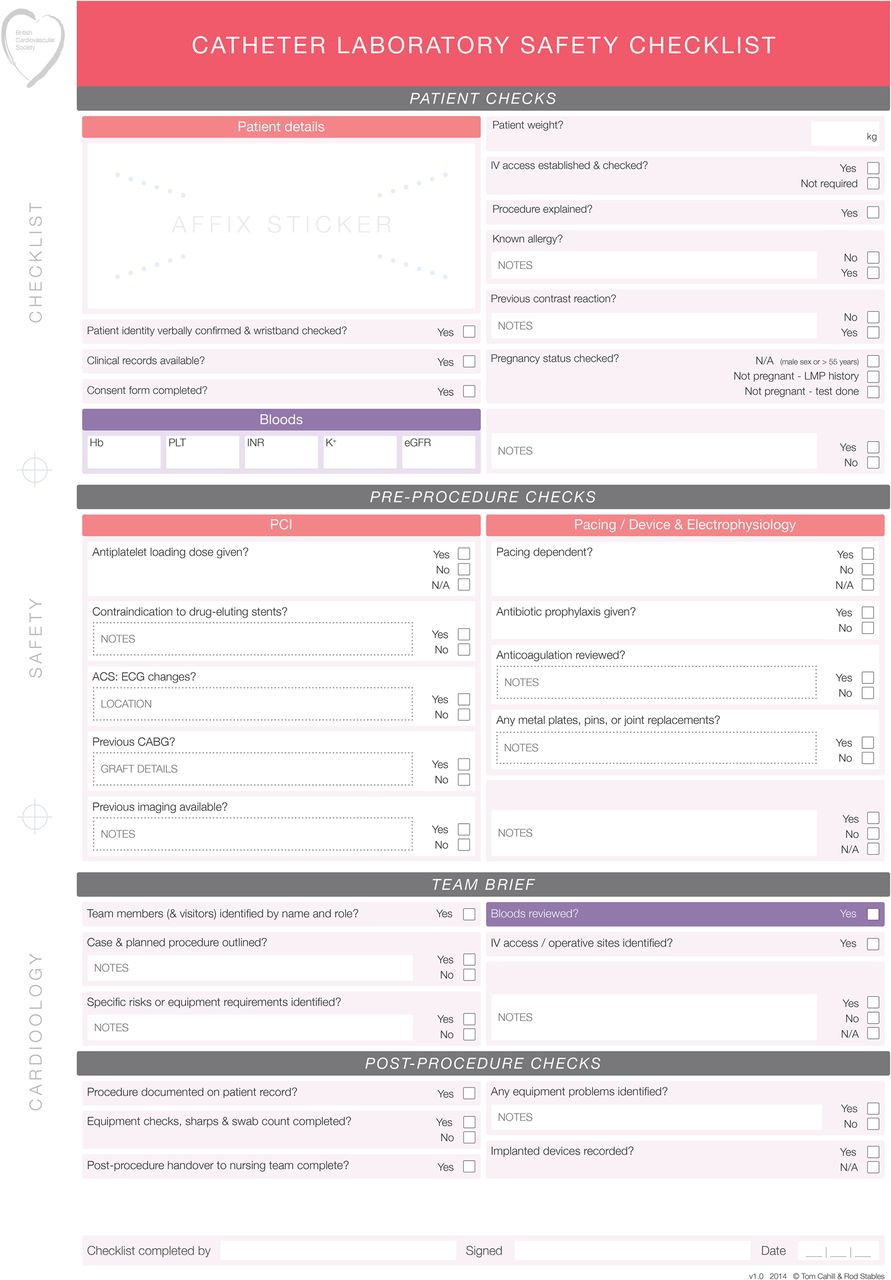
We have produced two variants of the cath lab checklist: stand-alone and integrated, available to download at http://www.bcs.com/checklist. The stand-alone checklist follows the paradigm of the WHO SSC as an area-specific, focused exercise to be initiated immediately preprocedure (figure 1). The integrated checklist includes a systematic approach to preprocedural preparation. The first half is a structured, accessible recording of relevant patient information in the prelab phase on the ward or day unit. This permits a more focused, efficient lab checklist without duplication, which forms the second half.

Stand-alone checklist.
Customised content
Most sections of the British Cardiovascular Society (BCS) cath lab checklist contain discrete boxes which can be modified to include additional questions, allowing it to be customised to local practice. Modifiable boxes appear in blue, labelled ‘Insert additional question here if required’. After editing the file is resaved, to generate a new version of the parent checklist which is optimally set up for the team using it (eg, figure 2).

{kind=link}
{kind=link}
Modified general anaesthetic appendix to include checks for transcatheter aortic valve implantation (TAVI); Permanent pacemaker (PPM).
Team brief
Both versions of the checklist include a team brief. We envisage the team brief being run by the first operator: it ensures all team members have a clear understanding of the proposed procedure and operative site(s), with reference to salient features of the patient, equipment requirements and specific issues or risks. It is a key checkpoint for prevention of ‘wrong procedure’ or ‘wrong site’ errors, which remain a major contributor to adverse events and litigation from surgery. In cardiology this could mean incorrect device implantation or placement, wrong coronary vessel or stent, or attempted access at a contraindicated site. More generally, team briefing reduces communication errors and improves attitudes to safety.7
To assist with running a team brief, we have included a mnemonic on the back of the checklist to guide content, which is not intended to be proscriptive, but may be helpful to operators. Our model is TIP BIG—team present; introductions by name and role (at least once for a session, to be repeated if the team changes); procedure outlined, with specific risks and equipment requirements; bloods reviewed; IV/operative access sites reviewed; group concerns?
Checklist in practice
Our guidance on implementation and practical use is intentionally brief—what works in one hospital may create problems in another. As a guide, however, we have found that the running nurse is well placed to perform the patient checks on arrival and post procedure, while the first operator is the logical person to conduct the team brief. The cath lab nursing team is ideally placed to oversee introduction of the checklist across all labs, prompt the team brief and audit compliance.
The cath lab of the future will undoubtedly be paperless, and we are currently working on versions of the checklist which are fully electronic. These could be displayed and completed in real time on an electronic whiteboard with key patient data on the lab screens or an electronic tablet.
Checklist challenges
The major challenges to checklist use in surgery have been twofold: implementation and compliance. Successful implementation requires a multifaceted approach. At the level of the organisation there must be institutional backing, drive and resource to facilitate change on the ground. Within a department, consistent and universal use is required such that the checklist becomes the expected norm in all labs, rather than the personal choice of some doctors. Among the staff, there needs to be involvement and buy-in from all members of the team, which is where local checklist modification and relevance can help. It is clear that the culture and environment matter. Most can be gained from a checklist when the team believes it has immediate practical value as well as the potential to improve outcomes.
The longer-term challenge is compliance, meaning completion of the checklist for every patient, and ongoing involvement, training and engagement with the underlying safety process. Despite the predominance of human factors errors, the focus of medical and nursing training in procedural specialties, including cardiology, is heavily biased towards technical competence. For effective checklist use in the cardiac cath lab, it is necessary to have a strategy of every patient, every time—including emergencies and primary angioplasty. There are very few circumstances when the team cannot pause for the brief period required for safety checks and an informative briefing.
Conclusions
The importance of human factors in the cath lab is under-recognised, and the potential benefits of safety checklists and team briefing are not being realised. The BCS cath lab safety checklist—a specialised and adaptable checklist designed for use in the cardiac cath lab—is a first step. It is a vehicle to introduce a team brief and to provide a focus on human factors and patient safety.
With appropriate implementation and guarding against complacency or a ‘tick box’ exercise, checklists have the potential to promote a culture of effective team based communication and reform patient safety in the cath lab.
Footnotes
-
Contributors RHS suggested the concept of a checklist for interventional cardiology. TJC and RHS designed the checklist and conducted the pilot evaluations. TJC wrote the original draft of the manuscript, which was revised by SCC, IAS and RHS.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.