Article Text

Statistics from Altmetric.com
A 65 year old man was referred because of an episode of syncope preceded by palpitations. He had a four month history of chest pain and palpitations unrelated to exercise. On admission, ECG showed sinus rhythm without repolarisation abnormalities. Echocardiography Doppler evaluation was normal. In an exercise thallium-201 test the patient achieved 76% of the predicted maximal heart rate with a 4.6 Mets workload. A 2 mm ST segment depression was observed in the anterolateral leads without chest pain. A thallium-201 scan showed myocardial perfusion abnormalities involving the anterior segment. The Holter recording revealed two runs of non-sustained monomorphic ventricular tachycardia (VT) at 160 beats/min, which the patient felt as palpitations but without angina. Programmed stimulation with ventricular pacing and extrastimuli did not induce VT. Left coronary angiography showed a significant systolic milking effect in the second portion of the left anterior descending coronary artery (fig1A), which appeared normal during diastole (fig 1B). There was no associated arteriosclerotic coronary disease. The patient was discharged and prescribed atenolol.
{kind=link}
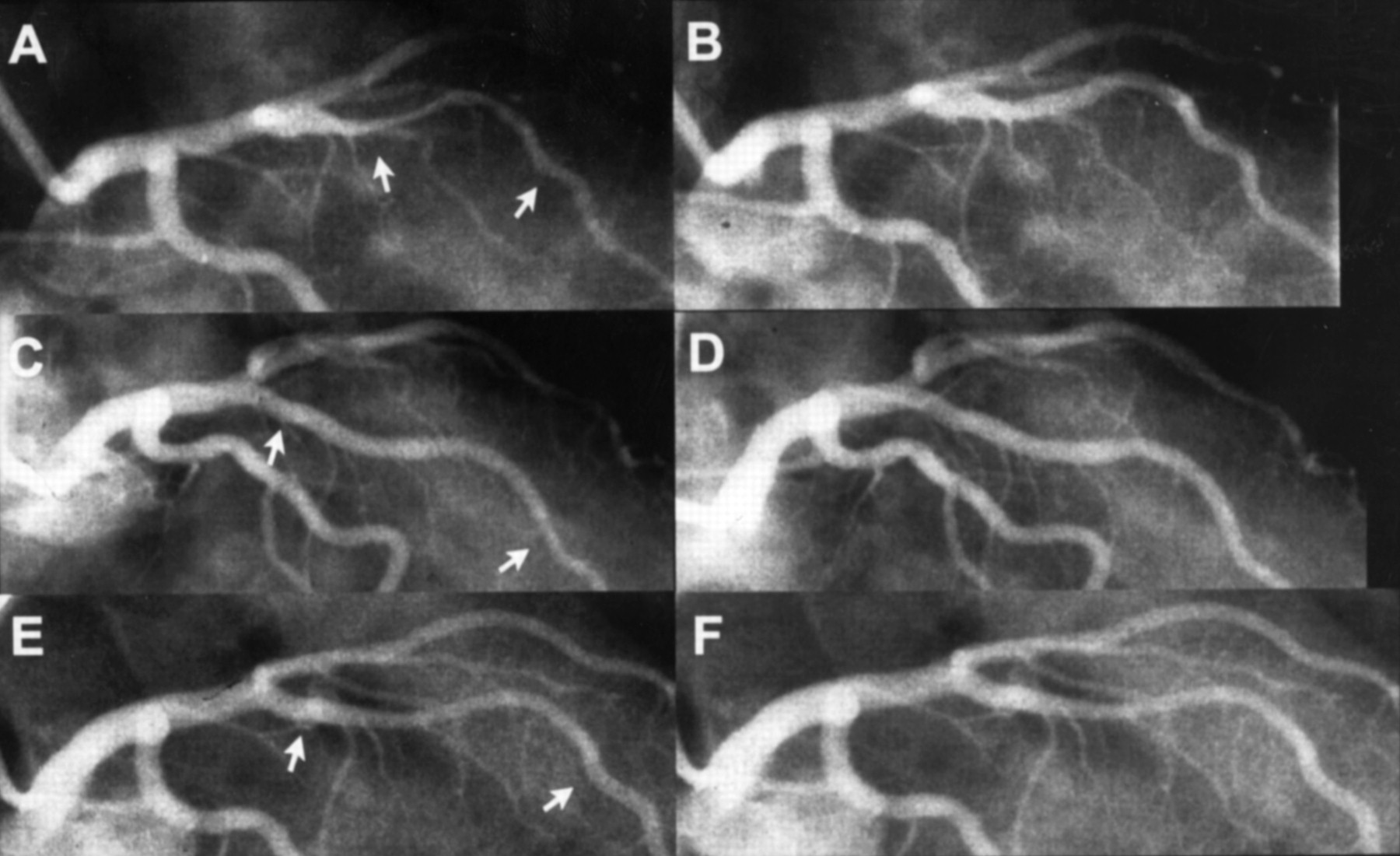
Angiographic changes observed in the bridged segment of the left anterior descending coronary artery (LAD) before and after coronary stenting and at six months’ follow up. Milking effect of the medium segment of the LAD (arrows) during systole (A), which disappeared during diastole (B). Angiograms in systole (C) and diastole (D) after the implantation of two consecutive Multilink stents (arrows). Selective left coronary angiograms in systole (E) and diastole (F) at six months’ follow up.
Six weeks later, the patient was readmitted for angina without arrhythmias. A percutaneous interventional approach was used to implant two Multilink stents (Advanced Cardiovascular Systems, Santa Clara, California, USA) of 3.0 × 25 mm and 3.5 × 15 mm in the bridging segment, and the systolic luminal narrowing disappeared (figs1C and D). The stent delivery system tracked easily through the bridged area and both stents were deployed at 11 atm. No balloon predilatation was performed. After the procedure atenolol was withdrawn and the patient received antiplatelet treatment with aspirin and ticlopidine.
A second exercise thallium test performed five weeks later was normal at maximum theoretical heart rate. Control angiography at six months showed a mild minimum luminal diameter loss without restenosis (figs 1E and F). The patient remains free from angina and arrhythmias.
The incidence of myocardial bridging ranges from 5% to 85% in necropsy studies, while the reported angiographic prevalence is from 0.5% to 1.6%.1 The course is usually benign with a five year survival of 97.5%; however, myocardial ischaemia, infarction, arrhythmias, and sudden death have been reported.2
To our knowledge, coronary stent implantation in myocardial bridging without angiographic evidence of arteriosclerotic lesions has been reported in only two patients who had acute myocardial infarction caused by the bridge.3 ,4 In both patients, a Palmaz-Schatz coronary stent (Johnson & Johnson Interventional Systems, Warren, New Jersey, USA) was successfully implanted in the LAD. One patient was asymptomatic six months after the procedure, but no angiographic follow up was available.3 In the other patient, angiography performed six weeks after the procedure for atypical chest pain did not show systolic compression at the stented segment.4 In our patient the systolic bridging of the LAD was associated with angina and possibly non-sustained monomorphic VT. Despite medical treatment the angina persisted; it stopped after the implantation of two coronary stents in the intramyocardial segment. Thallium-201 scintigraphy after stenting showed normalisation of myocardial distribution images. The stented bridging segment was longer than that previously described.3 ,4 The implantation of two coronary stents, covering a total length of 40 mm of coronary artery, was needed. We chose the Multilink stent because of its good trackability, flexibility, and resistance to external radial compression.5 This report is the first to show long term angiographic follow up after stenting of a myocardial bridge. No angiographic restenosis was observed six months after the procedure. However, coronary stent implantation may be ineffective in relieving angina in patients with widespread coronary bridging that involves the septal branches of the LAD artery. In addition, angina may recur because of luminal narrowing as a result of the proliferative response to endothelium damage during angioplasty, or because of shrinking of the scaffolding of the stent caused by external compression of the myocardial bridge.