Article Text

Statistics from Altmetric.com
Inerventional catheterisation in the treatment of patients with congenital heart disease has expanded dramatically since Rashkind first introduced balloon atrial septostomy in 1966. In many centres up to half of all cardiac catheterisations in congenital heart disease are therapeutic rather than diagnostic. Developments in plastics and alloy engineering have led to improvements in equipment for balloon or stent treatment and these techniques are playing an increasing role in the management of adults with congenital heart disease. The only existing guidelines, which represent the American consensus of opinion, have been published by the American Council on Cardiovascular Disease in the Young.1
Right ventricular outflow obstruction
Pulmonary valve stenosis
Balloon dilatation has proved extraordinarily successful in the treatment of pulmonary stenosis at any age. Improvements in guide wire technology and in balloon design have allowed successful transvenous valvoplasty to be carried out at very low risk even in the premature neonate and, in contrast to treatment of aortic stenosis, ballooning the pulmonary valve is effective even in the presence of cusp calcification in adult life.
There are no absolute indications for intervention in pulmonary stenosis and different centres vary in their threshold for treatment. In general pulmonary stenosis is a well tolerated lesion and the risk of sudden death is much lower than with obstruction to left ventricular outflow. Pulmonary stenosis does not always become more severe with age and may occasionally improve or even resolve spontaneously. Clinical signs and symptoms (usually exercise intolerance if the obstruction is severe), ECG changes, and echocardiographic findings all play a part in timing of intervention. As an approximate generalisation the combination of right ventricular hypertrophy and a peak flow velocity of 4 m/s or greater would encourage most cardiologists in the UK to intervene. Technically pulmonary balloon valvoplasty is usually straightforward,2 with optimum results being obtained with a balloon diameter between 120–150% of the diameter of the valve. It is rarely necessary to resort to surgery whatever the age of the patient, the exception being severe valve dysplasia when elasticity of the deformed cusps prohibits effective valvotomy (surgical resection of the cusps rather than valvotomy may be required). Pulmonary regurgitation induced by balloon valvoplasty is usually mild, appears to be well tolerated even in the long term, and does not appear to be any more severe than regurgitation after surgical valvotomy.
Some degree of infundibular stenosis often occurs with valvar stenosis. This is frequently related to right ventricular hypertrophy and may gradually resolve spontaneously after valve obstruction is treated; a failure of reduction in right ventricular pressure immediately after ballooning does not necessarily indicate failure of the procedure and patience may be required before making a definitive assessment of the results.3
In complex cyanotic heart disease associated with valvar pulmonary stenosis it is sometimes possible to improve pulmonary blood flow by a “limited” valvoplasty, thereby avoiding the need for palliative shunt surgery.4 The major factor in achieving good results is very careful patient selection and careful judgement of balloon diameter to avoid excessive pulmonary blood flow.
Balloon dilatation for pulmonary valve stenosis
Treatment of choice for valvar pulmonary stenosis at any age, even in adults with valve calcification
Main determinant of success is balloon size
- –
- A balloon of up to 150% the diameter of the valve may be required, in contrast to dilatation of the aortic valve, when large balloons are dangerous
- –
- “Limited” balloon valvoplasty may provide good palliation in complex cyanotic heart disease with pulmonary stenosis
Infundibular stenosis caused by right ventricular hypertrophy associated with valvar stenosis often improves spontaneously within a few weeks of ballooning the valve
Pulmonary regurgitation after ballooning is probably no worse than after surgical valvotomy
Balloon dilatation for non-valvar right ventricular outflow obstruction
Ballooning may help in selected patients with tetralogy of Fallot
Balloon expandable stents occasionally useful for infundibular stenosis in poor candidates for surgery
Proximal branch pulmonary artery stenoses may respond to balloon angioplasty but are often elastic and may require stenting
Stenosed right ventricular to pulmonary artery conduits may be dilatable but improvement often short lived; stenting may help but late stent fracture possible
Infundibular stenosis
Infundibular stenosis, because it is usually muscular, is generally treated surgically. However, on rare occasions infundibular stenting can offer effective palliation when surgical “correction” of a complex anomaly is not possible—for example, tetralogy of Fallot with diffuse pulmonary hypoplasia.5 Young children with hypercyanotic attacks associated with tetralogy of Fallot may benefit from balloon dilatation of the right ventricular outflow tract, even when the obstruction is principally infundibular.6 The mechanism for this improvement is not clear, but it seems likely that tearing and subsequent scarring of the infundibular muscle is involved.
Pulmonary atresia
Surgery remains the treatment of choice for tetralogy with pulmonary atresia. There have been some attempts to establish continuity between the right ventricle and the pulmonary trunk by laser or radiofrequency perforation of the atretic outflow tract, but the risk of perforation of the heart (sometimes fatal) is probably unacceptable in patients with long segment atresia. The rarest form of pulmonary atresia, where the ventricular septum is intact and the pulmonary valve is imperforate, is more amenable to transcatheter treatment. Laser or radiofrequency perforation of the valve followed by balloon dilatation may be very successful in selected cases and may be the only treatment necessary. Duct patency may need to be maintained for several weeks after a successful procedure as pulmonary blood supply remains duct dependent until right ventricular hypertrophy has regressed to some extent. Patience is usually rewarded and aortopulmonary shunt surgery is rarely required.7 The choice between laser and radiofrequency perforation of the valve is largely one of resources; the laser tends to burn through the valve faster and laser wires tend to be easier to manipulate. The wires' prices are similar but the laser generator is substantially more expensive than the radiofrequency counterpart.
Pulmonary artery stenoses
Pulmonary artery stenosis occurs most frequently in patients with tetralogy of Fallot. It may be present before surgery or may appear early or late after surgical repair (fig 1). It may be easily missed, particularly in adults and particularly when it is unilateral. Surgical repair of pulmonary artery stenosis may be technically difficult and narrowing may recur because of patch scarring and shrinkage, so when stenosis of a major branch occurs after surgery most centres would try transcatheter treatment before further surgery. Many pulmonary artery stenoses are elastic and recoil after simple balloon angioplasty,8 and some operators choose to proceed directly to stent implantation. Stenting may be technically difficult; it carries risks of stent embolisation, pulmonary artery rupture, and even death. It will not give a good result if the stenosis is too tough to be dilated. It therefore seems wise to try simple ballooning first to ensure that the lesion is dilatable and to be sure that stenting is really required. Experience so far suggests that restenosis caused by intimal proliferation in the stent is uncommon9 and that when it does occur repeat balloon dilatation is usually helpful. When pulmonary artery stenosis occurs postoperatively there is usually extensive fibrosis around the vessel to offer support after angioplasty. This is not the case for “native” artery stenosis and a less aggressive approach, possibly with serial procedures to enlarge the vessel gradually, is needed if pulmonary artery rupture (potentially fatal) is to be avoided.

Severe stenosis of the right pulmonary artery (top) after surgical repair of tetralogy of Fallot. There was no improvement after balloon dilatation because of elastic recoil, but a balloon expandable stent (bottom) has relieved the stenosis and considerably improved blood flow to the right lung.
Multiple peripheral pulmonary artery stenoses are much more difficult to deal with. Surgery rarely produces obvious benefit. There are rare cases where angioplasty or stenting of a prominent stenosis in a large branch might improve pulmonary perfusion, but the benefits may be offset by induction of segmental pulmonary oedema. There are no conclusive data at present to suggest any improvement in survival or objective improvement in symptoms.
Stenosis localised to the pulmonary trunk rather than its branches may also occur after surgery (most commonly after the arterial switch). This tends to be less responsive to ballooning10 and proximity to the pulmonary valve or the pulmonary artery bifurcation makes stent implantation difficult. Surgery is usually required.
Conduit obstruction
Conduits between the right ventricle and the pulmonary trunk eventually become obstructed (and calcified) whether they are allografts, homografts, or synthetic. When the conduit itself is stenosed balloon angioplasty or even stent implantation may help and surgical replacement of the conduit may be deferred in some cases by over two years.11 In some cases obstruction occurs at the proximal or distal anastomosis of the conduit and stenting may be more helpful. There are some concerns over the uneven stresses on stents in such situations (the proximal part of the stent will be within the right ventricular wall) and stent fracture has been reported.11
Balloon dilatation for aortic stenosis
Unclear how results compare to surgical valvotomy; no randomised trials performed
Many, but not all, UK centres balloon as first line treatment for young patients
Good palliation possible even after previous ballooning or surgical valvotomy
Balloons larger than the valve are dangerous
Largely abandoned for calcified valves in older patients because of limited success and high morbidity
Left ventricular outflow obstruction
Valvar aortic stenosis
There is still divided opinion in the UK over whether surgery or balloon valvoplasty is better treatment for aortic stenosis in children. Logic suggests that surgery allows a careful valvotomy under full vision and that this would be unlikely to be matched by the crude inflation of a balloon, yet clinical data have not shown any clear difference between the two approaches.12 Severe regurgitation or important residual stenosis may occur after either procedure but no randomised trial to compare the two has been (or is ever likely to be) performed. In neonates early concerns about vascular damage by balloon catheters have proved unfounded, with improved balloon design and with formal arteriotomy using the axillary or carotid arteries in preference to the femoral artery. In contrast to pulmonary valvoplasty it is important to use a balloon no larger (ideally slightly smaller) than the aortic root if cusp avulsion is to be avoided.
Indications to intervene should be similar whether surgery or catheterisation is employed. In neonates the decision is rarely difficult as the circulation is usually duct dependent with severe stenosis. In older children, however, timing is more difficult; the combination of left ventricular hypertrophy, a left ventricular outflow velocity in excess of 4 m/s, and either ECG repolarisation abnormalities or an abnormal blood pressure response to exercise, would prompt treatment in most centres. The older the patient, the more technically difficult the procedure. This is largely because of difficulty keeping the balloon in a stable position during inflation. Use of a stiff guide wire with a floppy tip curled in the ventricle or injection of adenosine to induce transient ventricular standstill have been advocated. Nonetheless, balloon valvoplasty may produce good palliation in older children,13 even if the patient has previously undergone balloon valvoplasty or surgical valvotomy.14 Complications include arterial damage, cardiac perforation, embolic stroke, and induction of severe aortic regurgitation. Bacterial endocarditis related to ballooning appears to be very rare but most operators give prophylactic antibiotics to cover the procedure. Transcatheter treatment is probably best avoided later in life when the valve has become calcified.15
Coarctation and recoarctation of the aorta
Native coarctation balloon angioplasty
- Neonates
- –
- High incidence of early recoarctation
- –
- A poor substitute for a good surgeon
- Older children and adults
- –
- Controversial because of risk of incomplete relief of obstruction or aneurysm formation
- –
- Stent implantation might improve relief of obstruction and reduce aneurysm formation but data are inconclusive at present
Recoarctation
- Widely accepted as treatment of first choice, low incidence of aneurysm formation.
- –
- But aortic rupture reported if previous surgical repair by patch aortoplasty
Other forms of aortic stenosis
There have been occasional reports of balloon dilatation of discrete, membraneous subaortic stenosis16 and of supravalvar stenosis, but results are not encouraging and surgery remains the treatment of choice.
Coarctation and recoarctation of the aorta
Native (unoperated) coarctation
In neonates balloon dilatation of coarctation rarely provides more than transient benefit and restenosis occurs as the rule rather than the exception because of constriction of ductal tissue; surgery remains the treatment of choice. In infants, older children, and adults there is divided opinion on the optimum form of treatment.17-19Death at surgery for coarctation is very rare now, but it is the associated small risk of spinal cord damage and consequent irreversible paraplegia that has led to balloon angioplasty having some protagonists. Balloon angioplasty works by tearing the intima and media of the aorta, leaving only the adventitia intact. It is not surprising that balloon dilatation of native coarctation is associated with a risk of false aneurysm formation (up to 20% in some series). Some groups have advocated a graduated approach, using repeated procedures to enlarge the stenosis gradually, but as yet there is no clear evidence that graduated ballooning carries any less risk.
A major factor in aneurysm production is the size of the balloon. Various formulae to aid in the choice of balloon size have been suggested, either related to the diameter of the coarctation itself or to the diameter of the descending aorta at the level of the diaphragm. It is clear that for some partially elastic stenoses it is necessary to employ a balloon larger than the required final vessel diameter. This is probably an important factor in aneurysm formation, but it is not yet clear whether using a stent to overcome elastic recoil20 (allowing a smaller balloon to be used) will reduce risk of aneurysm. Covered stents, which might be expected to minimise the effects of tearing the aorta, are not yet widely available. An additional factor which should be taken into account when considering balloon angioplasty is that partial relief of coarctation is really not acceptable! If a severe coarctation is partially treated collateral vessels may regress, thereby potentially increasing the risk of spinal cord damage at operation.
Recoarctation
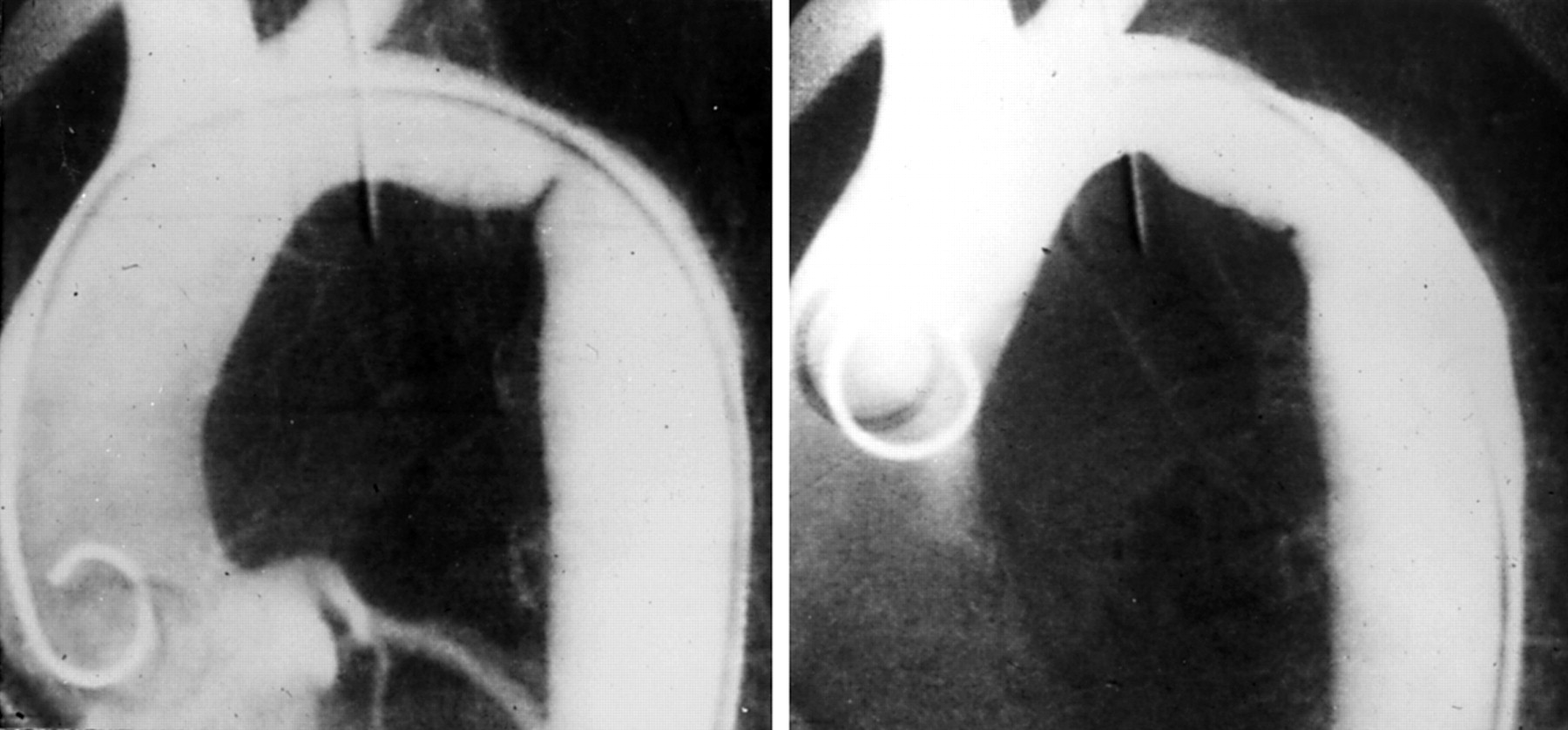
Recoarctation after neonatal surgical repair occurs in up to 10% of cases in most published experience. In contrast to native coarctation, balloon angioplasty is widely favoured for treatment of recoarctation; this is because the aorta is surrounded by supportive fibrous scar tissue and the risk of inducing a false aneurysm is low, particularly if care is taken to avoid oversized balloons (fig 2). Aortic rupture and death caused by disruption of the suture line has been reported after dilatation of recoarctation in patients who have had patch repair (as opposed to subclavian flap or end to end anastomosis). Many centres regard patch repair as an indication for surgical rather than transcatheter treatment.

{kind=link}
{kind=link}
Aortography 14 years after subclavian flap repair of coarctation (left). Although often referred to as recoarctation, this appearance is almost certainly caused by residual rather than recurrent stenosis. Discrete, shelf like lesions like this respond well to balloon dilatation (right), with low risk of aortic aneurysm or rupture in patients who have surrounding scar tissue caused by previous surgery.