Article Text

Statistics from Altmetric.com
Infarction is the most intensively studied medical intervention in the history of clinical investigation, with more than 200 000 patients enrolled in large scale, worldwide trials. The results of these trials have led to an irrevocably altered approach, with routine use of reperfusion treatment. Streptokinase, tissue plasminogen activator (t-PA), and new plasminogen activators have been shown to reduce mortality significantly, and the reduction is inversely proportional to the time that treatment is initiated from symptom onset. For patients treated in the first 60 minutes of symptom onset, the so called “golden hour”, mortality is reduced by more than 50%. Even frank prevention of the event can be assured in many patients treated in this very early time frame. Nevertheless, there are some major obstacles to optimal reperfusion treatment that have been increasingly recognised in recent years, which new directions in this field will hopefully circumvent. This paper will review the substantive progress in the field, including recognition of major pitfalls, and lay the groundwork for future improvements in pharmacologic myocardial reperfusion treatment.
“Patency centric” approaches
With the validation of intravenous thrombolytic treatment versus placebo in the classic GISSI 1 and ISIS 2 trials,1 ,2 the next step was to determine whether a higher level of early infarct vessel patency would result in improved survival. This was the focus of the GUSTO 1 trial which showed that a significant increase in patency at 90 minutes after treatment was initiated, from 30% with streptokinase to 54% with accelerated t-PA, was associated with a 15% reduction in mortality (fig 1).3 The term “patency” refers to brisk flow and clearance of angiographic contrast dye through the affected epicardial artery.

(A) Mortality curves in GUSTO 1 by thrombolytic strategy assignment. For streptokinase (SK) the parentheses indicate the heparin strategy, intravenous (iv) or subcutaneous (sc). (B) Patency of the infarct vessel at 90 minutes of treatment in the GUSTO 1 angiographic trial evaluating the four thrombolytic strategies.
More recently, trials of new plasminogen activators have gone forward using accelerated t-PA as the “gold” standard for comparison. The new plasminogen activators are bioengineered mutants of wild type t-PA. All have longer half lives and are administered as a single or double bolus. Three new agents, reteplase (r-PA), tenectaplase (TNK), and lanetoplase (n-PA) have each been studied in trials of 15 000 to 17 000 patients. None of these trials have shown superior mortality outcomes with the new plasminogen activators compared with t-PA. For TNK, “equivalence” was demonstrated with virtually the same mortality for TNK as with t-PA,2 but for r-PA and n-PA there were very small gaps in mortality compared with t-PA (approximately 0.20 absolute per cent) that pre-empt an unequivocal declaration of “equivalency”. Nevertheless, the field of thrombolytics has widened greatly from 1987 when the initial commercialisation for acute myocardial infarction was granted with the original choice of either streptokinase or t-PA. r-PA is now registered for use in most countries throughout the world and the approval for TNK is imminent.
Although new plasminogen activators have been shown to achieve more rapid or complete infarct vessel patency than t-PA, this has not resulted in an improvement in survival. Figure 2 shows data from the angiographic study known as RAPID 2, which compared r-PA and t-PA, juxtaposed with data from the GUSTO 3 mortality trial which also compared these two agents.4 ,5. Even though RAPID 2 showed better early patency for r-PA, there was not even a trend for less mortality. This strongly suggests that the relation of patency to survival is not as direct and straightforward as had been anticipated.

(A) Patency of the infarct vessel in two angiographic comparative trials. (B) Mortality at 30 days for each thrombolytic strategy.
Unrecognised importance of the microcirculation
A likely explanation for the discrepancy between infarct vessel patency and survival lies in microvascular obstruction. A large number of studies have shown that epicardial artery patency does not assure microvascular flow. Indeed, the classic study by Ito and colleagues using contrast echocardiographic tissue imaging showed that at least one in four patients with TIMI 3 flow (brisk epicardial arterial flow) do not have tissue level perfusion.6 Many groups have independently confirmed these findings and extended the significance of lack of reflow at the tissue level. For example, Porter and colleagues have shown that end systolic cavity size and ejection fraction are impaired in patients with TIMI 3 flow but without tissue level perfusion.7
Beyond contrast echocardiography, other investigators have used imaging modalities such as magnetic resonance or intracoronary Doppler flow velocity to assess microvascular obstruction. During extended follow up of a cohort of patients after myocardial reperfusion treatment,8 the finding of microvascular obstruction carried a fourfold increase in adverse events including death, reinfarction, or the development of congestive heart failure. In a randomised trial of 200 patients undergoing primary stenting for acute myocardial infarction, Doppler assessment of the infarct vessel showed a notable increase in peak velocity with the use of abciximab, a potent platelet glycoprotein IIb/IIIa inhibitor.9
ADMIRAL: Abciximab associateD with priMary angIoplasty and stenting in acute myocaRdiAL infarction
CCF: Cleveland Clinic Foundation
GISSI 1: Gruppo Italiano per lo Studio della Streptochinasi nell'Infarto Miocardico
GUSTO 1: Global Utilization of Streptokinase and t-PA for Occluded coronary arteries
INTRO: INTegrilin and Reduced dOse of thrombolysis
ISIS 2: Second International Study of Infarct Survival
Munich: See reference 9
RAPID 2: Reteplase (r-PA) versus Alteplase Patency Investigation During myocardial infarction
RAPPORT: ReoPro in Acute myocardial infarction and Primary PTCA Organization and Randomized Trial
SPEED: Strategies for Patency Enhancement in the Emergency Department
TIMI 14: Thrombolysis in Myocardial Infarction (with abciximab)
These pivotal findings have revamped our understanding of the reperfusion process. Indeed, rather than achieve complete dissolution of the thrombus, our treatments are likely achieving only partial clot dissolution and potentiating embolisation of part of the thrombus into the microcirculation. This sets up the backdrop for the “illusion” or false sense of achieving reperfusion by improperly focusing on the epicardial artery, when the critical supplier of perfusion to the infarct territory may be obstructed.
Beyond the partial clot dissolution, the constituency of the thrombus is particularly important. Underlying the coronary thrombotic event is a fissured, eroded, or frank atherosclerotic plaque rupture. This breach of the vessel wall first sets up platelet thrombus that is seen angioscopically as “white” thrombus. Quickly surrounding this nidus of platelet aggregation is the “red” thrombus that is fibrin rich. Accordingly, the approach of dissolving the culprit coronary artery thrombus is presently focused on the “red” clot component.
Unfortunately, “thrombolytics” are not really thrombolytics because plasminogen activators are “fibrinolytics”—that is, rather than lysing a coronary thrombus, fibrinolytics can only achieve dissolution of the fibrin strands making up the “red” thrombus (fig 3). This leaves thrombin, previously enmeshed in the “red” clot, exposed and leads to a prothrombotic state. Not only can exposed, activated thrombin beget its own formation via an autocatalytic loop in the extrinsic coagulation pathway, but thrombin is the most potent platelet proaggregatory biologic molecule. Thus, the mainstay of our current approach to myocardial reperfusion is narrowly directed to the fibrin–thrombus component and, unfortunately, induces a prothrombotic state.

Prothrombotic effects of fibrinolytic treatment. Coronary thrombus is composed of a platelet core with fibrin–thrombin admixture (“white” and “red” clot). After fibrinolytic treatment, there is exposure of free thrombin, which autocatalytically begets more thrombin and strongly promotes platelet aggregation (note more platelet mass). Platelets themselves are resistant to fibrinolytic treatment and furthermore secrete large amounts of plasminogen activator inhibitor (PAI-1), which is a potent antagonist to fibrinolysis. Reproduced from Topol EJ. Circulation1998;97:211–18, with permission.
Evidence for the untoward effect of fibrinolytics may also explain part of the discrepancy seen in the large scale mortality reduction trials. In GUSTO 3, where r-PA failed to provide survival benefit compared with t-PA, r-PA was shown to activate platelets more than t-PA.10 This would counter the facilitation of infarct vessel patency of r-PA, and likely would result in some higher proportion of microvascular obstruction.
More comprehensive thrombolysis
A combined strategy of low dose fibrinolytic and full dose platelet-lytic has been proposed.10 The advantages of this “fibrinoplatelet” lysis approach would include the ability to reduce the fibrinolytic dose, thereby potentially avoiding the prothrombotic state and the risk of intracerebral haemorrhage. Second, such a strategy is more comprehensive in addressing both the “red” and “white” components of the coronary artery thrombus. Intravenous platelet glycoprotein IIb/IIIa inhibitors are fully capable of rapid dissolution of platelet “white” thrombus. Even though platelet activation is inevitable with the use of a plasminogen activator, this effect would potentially be overridden by concomitant administration of a potent antiplatelet inhibitor. Of course, a theoretical limitation of the combination strategy is serious bleeding complications, as these patients also receive concurrent anticoagulation and are thus “bombarded” with three different classes of agents simultaneously. Nevertheless, since the early use of pharmacologic reperfusion treatment patients have received combined plasminogen activators, heparin, and aspirin. So the proposed approach can be viewed as refinement of each of the limbs of the fundamental strategy.
Pilot studies have been especially encouraging. Combined t-PA or r-PA with abciximab, or eptifibatide, have yielded very high frequencies of early infarct vessel patency. In fig 4, data at 60 minutes for three different trials are summarised and compared with full dose t-PA, which is still considered to be the “gold” standard. These findings support a near 50% improvement of epicardial infarct vessel patency for combined half dose fibrinolytic and full dose of glycoprotein IIb/IIIa inhibitors.

Angiographic patency (TIMI 3) of the infarct vessel in four sets of patients using the same core angiographic laboratory t-PA is compared with three trials of combined half dose fibrinolysis and full dose glycoprotein IIb/IIIa inhibition.
Perhaps more important than patency of the infarct vessel is the improvement of microvascular perfusion. Although many new imaging modalities may assess this in an elegant fashion, the easiest and most accessible method is to use a 12 lead ECG. A finding of > 70% resolution of ST segment elevation from baseline is highly indicative of restoration of perfusion at the tissue level. Indeed, in the TIMI 14 trial of t-PA and abciximab, there was a more than 50% increase in resolution of ECG ST segment elevation, reflecting relief of microvascular obstruction. Even so, 90 minutes after treatment was initiated 30% of patients with the combined strategy of low dose t-PA and abciximab did not have > 70% ST segment elevation resolution. These findings have been replicated in other phase II studies of combined lytic strategies, and suggest that the combination should be considered a significant step forward for relief of microvascular obstruction but certainly not viewed as a “be all and end all” treatment. The fact that nearly a third of patients are not having tissue level perfusion from a “comprehensive” lytic strategy suggests the need for additional components of an ideal, futuristic reperfusion approach.
Indeed, one of the most important and fundamental obstacles is time. The excessive time that it typically takes for patients to present to an emergency room, or for the healthcare team to deliver rapid treatment, frequently is relatively late for making a difference in salvaging myocardial tissue. When there is extensive damage, the myocardial oedema, leucostasis, and inflammatory reaction in the subtended myocardium may make tissue level perfusion impossible or futile. No matter what strategy is ultimately developed for improved myocardial reperfusion, the issue of timeliness will certainly remain centre stage.
The longstanding feud with catheter based reperfusion
The early trials of immediate coronary angioplasty following t-PA showed higher mortality and reinfarction rates, and the need for emergency bypass surgery. This was not expected at the time (late 1980s). It was known that most patients have a significant underlying atherosclerotic lesion after fibrinolytic treatment. Furthermore, alleviation of the stenosis early on in the course of treatment was expected to be a more definitive strategy. On the other hand, when primary balloon angioplasty was performed as sole treatment (no antecedent lysis), the adverse events appeared to be considerably less than when this procedure followed intravenous t-PA. What was not understood at the time was the pro-thrombotic “dark” side of fibrinolytic treatment. A literal “feud” was engendered between the “balloonatics” and the “thrombolunatics” that has persisted for more than a decade.
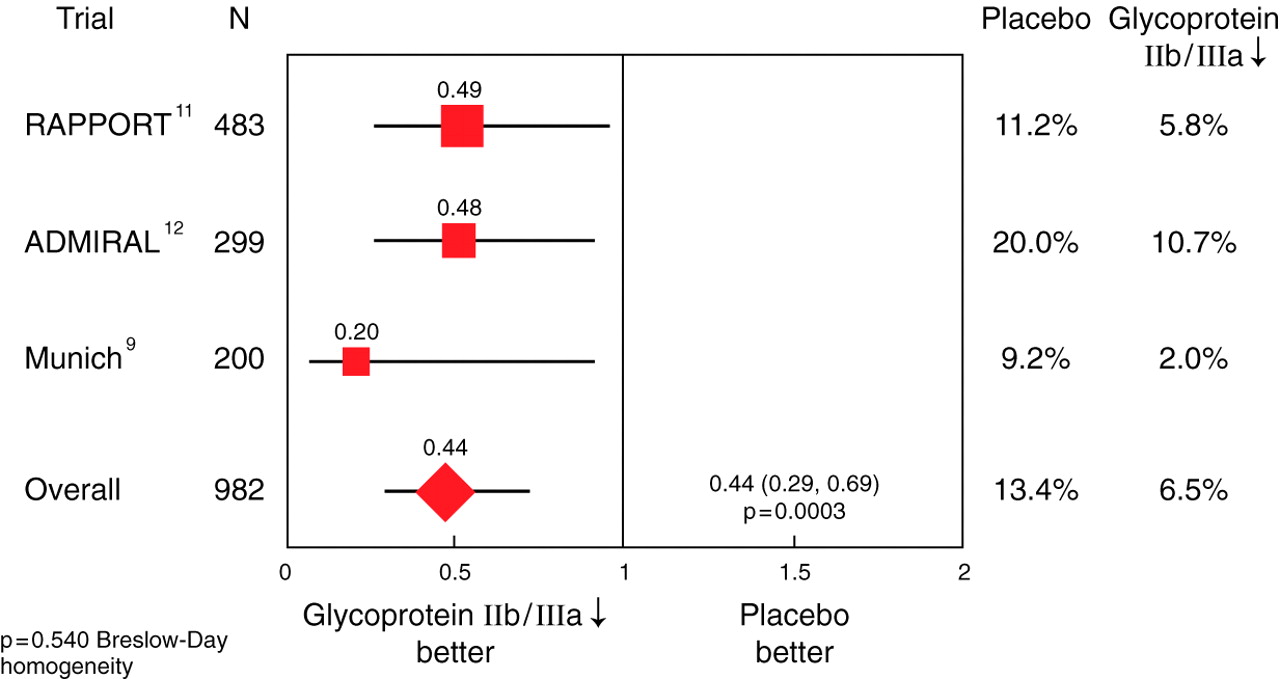
There is no reason for partitioning of the two forms of reperfusion treatment now that we have enhanced understanding of the biological process. Intravenous platelet glycoprotein IIb/IIIa treatment or placebo has been administered on a double blind basis in three catheter based reperfusion trials as summarised in fig 5.9 ,11 ,12In all three trials there was a pronounced reduction of the composite end point of death, reinfarction, or urgent revascularisation. Furthermore, we now know that transcoronary intervention is almost always accompanied by embolisation of atherosclerotic debris, in addition to the dislodgement of thrombotic material. Microvascular obstruction can result as a response to embolisation, and potent platelet glycoprotein IIb/IIIa inhibitor treatment would be expected to relieve or pre-empt the process. The direct Doppler demonstrations of improved microvascular perfusion by Neumann and colleagues strongly support this tenet.9
Summary
The relation of patency to survival is not as direct and straightforward as had been anticipated
The finding of microvascular obstruction carries a fourfold increase in adverse events including death, reinfection, or the development of congestive heart failure
Considerable data are emerging to show the ability of low dose fibrinolytics and glycoprotein IIb/IIIa inhibition to relieve or prevent microvascular obstruction
No matter what strategy is ultimately developed for improved reperfusion, the issue of timeliness will certainly remain centre stage
In order to validate the use of a combined lytic approach and the implications of microvascular perfusion, data for large scale trials will be necessary
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Odds ratio and 95% confidence intervals (CI) for 30 day composite of death, myocardial infarction, and urgent revascularisation in three trials of catheter based reperfusion with abciximab or placebo.
The relation of patYet the simple adjunctive use of a glycoprotein IIb/IIIa inhibitor is not taking advantage of a pharmacologic strategy designed to achieve early reperfusion and foster a successful catheter based intervention. While intravenous glycoprotein IIb/IIIa inhibition by itself can achieve streptokinase like patency results, the ideal situation would be to achieve “macro” and “micro” vessel patency as quickly as possible. The average time from “door to balloon” is nearly 120 minutes, such that a drug treatment that restores patency long before entering the cardiac catheterisation laboratory, in the highest proportion of patients, would be expected to be of considerable value. In fact, fewer patients have even required catheter intervention in our early experience because of the lack of a significant residual stenosis.
“Connecting the dots”
Many of the concepts described in this review are theoretical, based on experimental models, observational studies, or extrapolation. In order to validate the use of a combined lytic approach, and the implications of microvascular perfusion, data from large scale trials will be necessary. One such trial that is currently ongoing is GUSTO, a 17 000 patient trial comparing r-PA (full dose) as a standard fibrinolytic approach with low dose r-PA (half the usual dose) combined with abciximab. This trial should be completed by the end of 2000 with the primary end point of 30 day mortality. As the event rate for intracerebral haemorrhage is very low (< 1%), only in controlled trials of thousands of patients can the safety of the experimental combined strategy be assured. Substudies, such as the use of continuous 12 lead ECG and conventional ECG assessment for resolution of ST segment elevation, will be helpful to show the link between mortality reduction and microvascular perfusion. Other combination approaches of TNK or t-PA with eptifibatide and TNK with tirofiban will incorporate mechanistic studies using contrast echocardiography and magnetic resonance imaging. Ultimately, in the next couple of years we should have ample evidence that a new standard of myocardial reperfusion has been validated, and that a significant mechanism for improving survival relates to better flow at the tissue level. With acute myocardial infarction as the number 1 killer, and awareness of the inadequacies of our current treatment, it is vital to continue to refine our approach to the desired goal—that no one with evolving myocardial infarction actually suffers infarction. To that end, we have quite a long way to go.