Article Text

Statistics from Altmetric.com
Risk stratification in acute coronary syndromes aims to identify those patients at greatest risk of recurrent ischaemic events who might benefit prognostically from further investigation and treatment. Unfortunately, however, none of the clinical or investigative markers currently available has sufficient diagnostic power to identify all high risk patients while excluding those at negligible risk. Moreover, for patients judged to be at high risk, the value of specific treatment may be poorly defined. Nevertheless, high event rates and finite facilities for invasive management emphasise the clinical and logistical importance of risk stratification which should play a central role in the management of acute coronary syndromes.
What is the risk and when is it greatest?
Our own database in east London shows that about 30% of patients with acute myocardial infarction and 20% with unstable angina experience a major event (death or non-fatal coronary syndrome) during the first year after hospital admission. Risk, however, is not a linear function of time, and as fig 1 shows, 66% of all major events during the first six months after myocardial infarction occur in the first 30 days. Moreover, the determinants of risk may change with time, acute phase arrhythmias and myocardial rupture in the first 48 hours giving way to reinfarction, heart failure, and secondary arrhythmias later after presentation. Thus assessment of risk, using strategies tailored to address its changing determinants, is an essential part of the management of acute coronary syndromes and must be applied at an early stage to identify successfully patients with most to benefit. Recognition of this fact has rendered obsolete old arguments about the appropriate timing of stress testing and other non-invasive tests which must be performed as early as possible (certainly before discharge) to be of significant value for risk stratification.

Recurrent ischaemic events in the first six months after acute myocardial infarction (unpublished data of 1829 patients on Newham General Hospital database). Among 1829 patients with acute myocardial infarction, recurrent ischaemic events (death, non-fatal acute coronary syndromes) occurred in 481 patients during the first six months. Of these recurrent events, 66% occurred in the first 30 days.
Determinants of risk
The major determinant of risk in the acute phase of ischaemic syndromes is ventricular fibrillation, which probably accounts for > 80% of out of hospital deaths. For hospital populations, risk is determined by the cumulative impact of a variety of clinical, pathophysiological, and coronary anatomical factors. Most important are advanced age and ventricular dysfunction (fig 2), with residual myocardial ischaemia and cardiac arrhythmias also contributing significantly.1 Thus, the mortality risk within one year of acute myocardial infarction is 14.8 times greater in men aged ⩾ 70 years with heart failure than in men aged < 60 years without heart failure.2 Clinical factors variably related to advanced ventricular dysfunction include diabetes, heart failure, Q wave development, and bundle branch block, while ongoing chest pain and fluctuating ST segment change usually reflect important residual ischaemia.
Major determinants of risk in acute coronary syndrome
Electrical instability
Advanced age
Left ventricular dysfunction
Residual ischaemia

Kaplan–Meier overall and event free survival by age for 1225 patients with acute myocardial infarction surviving to hospital discharge. LVF, left ventricular failure. Reproduced from Barakat et al2 with permission of The Lancet.
Making risk assessments
Faced with these multiple determinants of risk, the clinician must decide which to measure and which to apply in the stratification process. Clinical determinants are, of course, readily available and are often sufficient to define risk and management options without the need for additional tests. Cardiac chest pain that fails to settle, for example, indicates that the risk of further ventricular injury is high and provides clear indication for angiography with a view to revascularisation. Similarly, intractable heart failure confirms a high level of risk, and additional tests aimed merely at refining risk status will not always provide significant incremental information. In many patients, however, particularly those who make an uncomplicated initial recovery, risk status is difficult to define based solely on clinical criteria and in this group further tests are necessary. These will usually include an evaluation of left ventricular function, or residual myocardial ischaemia, or both. Interpretation of these tests should take account of clinical, electrocardiographic, and biochemical data already available, recognising that risk stratification is an incremental process and the predictive value of non-invasive investigation is influenced importantly by the pretest assessment of risk.
Risk stratification in the acute phase of coronary syndromes
Ventricular fibrillation, the major determinant of risk in the acute phase, requires immediate electrical cardioversion to avoid death. Because it is largely unpredictable, electrocardiographic monitoring and ready access to a defibrillator are the most important management strategies for saving lives in acute coronary syndromes. Also important is antithrombotic treatment which should be given to all patients acutely, with daily aspirin continuing thereafter. In other respects, management in the acute phase of coronary syndromes is largely determined by the perceived risk as judged by clinical, electrocardiographic, metabolic, and biochemical factors.
Clinical factors
Severe hypertension in the acute phase that does not respond promptly to opiate analgesia, heightens risk by intensifying ischaemia and predisposing to myocardial rupture. Intravenous β blockade may protect against rupture and should be used in acute infarction if systolic blood pressure is > 160 mm Hg. Heart failure also heightens risk and identifies a group that may benefit prognostically from angiotensin converting enzyme inhibition and β blockade. The risk is particularly high in cardiogenic shock which remains the leading cause of hospital death despite reperfusion treatment; primary angioplasty does not appear to offer any short term benefit but may improve survival in the longer term. For most patients, emergency cardiac catheterisation is reserved for patients with ongoing or recurrent chest pain, although this policy is largely pragmatic and may be overly conservative, particularly for patients with unstable angina.3
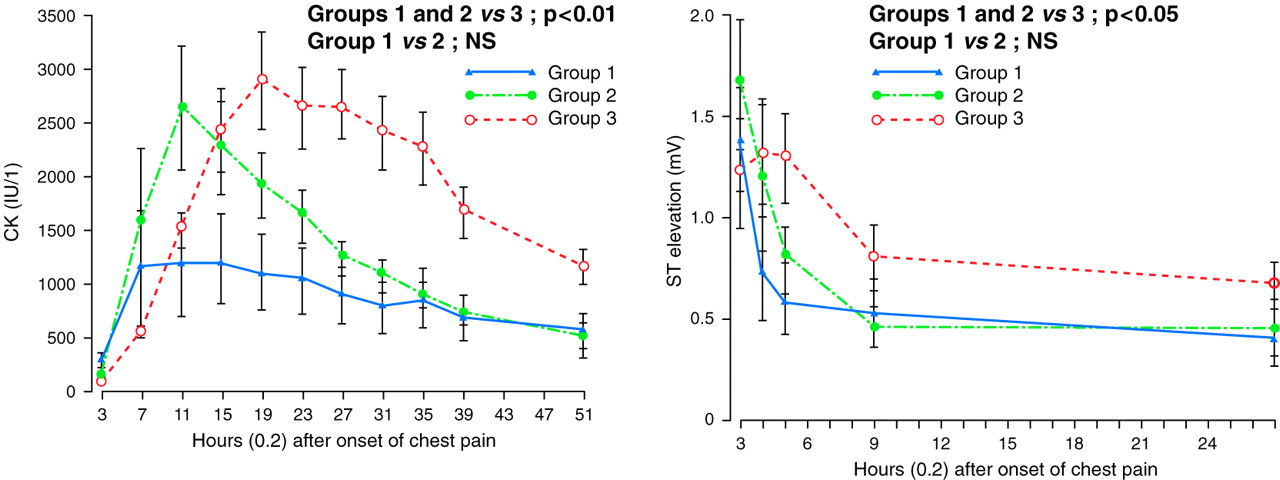
Electrocardiographic factors
When regional ischaemia is sufficiently severe to produce ST segment depression or elevation, risk increases significantly.4 Thus, in unstable angina ST depression, particularly when recurrent, identifies a group at risk of infarction and provides indication for urgent cardiac catheterisation.5 In myocardial infarction, ST elevation increases risk substantially but its prompt resolution, either spontaneously or in response to thrombolytic treatment and aspirin (fig3), may reflect successful reperfusion and is a good prognostic sign, particularly if Q waves do not develop.6 Failure of ST resolution, on the other hand, or recurrent episodes of ST elevation indicate failed reperfusion or coronary reocclusion, which increase risk and may provide indication for urgent angiography with a view to rescue angioplasty. Risk also increases progressively with increasing degrees of atrioventricular block, and is particularly high when advanced bundle branch block complicates anterior infarction, probably reflecting the adverse consequences of extensive myocardial injury. Primary ventricular arrhythmias in the first 48 hours of acute coronary syndromes do increase the risk of hospital death although there is no evidence that prophylactic antiarrhythmic treatment is helpful. Secondary arrhythmias later after admission are commonly associated with advanced left ventricular dysfunction and identify a group at high risk of death in the first year. If secondary arrhythmias fail to respond to treatment cardiac catheterisation is recommended to define revascularisation options, with electrophysiological investigation in reserve for tailored antiarrhythmic treatment or deployment of an implantable defibrillator.
Electrocardiographic determinants of risk in acute coronary syndromes
ST elevation or depression
Failure of prompt ST resolution in response to treatment
Q wave development
Intraventricular conduction defects
Secondary arrhythmias

Kinetics of creatine kinase (CK) release (left) and ST resolution (right) in response to coronary reperfusion. Sequential coronary arteriograms 90 minutes apart in 41 patients presenting with acute coronary syndromes and ST elevation permitted identification of three groups: group 1—patency of infarct related artery at first arteriogram before thrombolytic treatment (n = 12); group 2—early recanalisation of the infarct related artery within 90 minutes of thrombolytic treatment (n = 10); group 3—persistent occlusion of infarct related artery (n = 19). Serial CK analysis showed early peaking in groups with coronary recanalisation (groups 1 and 2). Cumulative CK release was considerably greater in patients with failed recanalisation (group 3). Serial ECGs showed rapid resolution of ST segment elevation in patients in groups 1 and 2, while in those patients with persistent coronary occlusion (group 3), ST elevation persisted considerably longer. Reproduced from Timmis et al6 with permission of BMJ Publishing Group.
Metabolic factors
The heightened risk associated with diabetes requires measurement of blood glucose concentration. Patients known to be diabetic or with a blood glucose concentration > 11 mmol/l should receive insulin and glucose infusion during the acute phase which improves prognosis in acute myocardial infarction, although whether similar benefit occurs in unstable angina is not known. Hypercholesterolaemia also increases long term risk and lipid profiles should be measured at the time of admission, patients with a total cholesterol ⩾ 5.0 mmol/l benefiting from treatment with statins.
Biochemical factors
Enzymes released from cardiac myocytes have long been used as markers of injury to confirm myocardial infarction in patients presenting with acute coronary syndromes (fig 3). Creatine kinase and its more specific MB fraction remain widely used, but in recent years a number of novel biochemical markers (myoglobin, troponin I and T) have been developed that are more sensitive and appear in the blood earlier after the onset of symptoms. Almost regardless of which biochemical marker is used, increased concentrations are associated with an increased risk of recurrent ischaemic events. Myoglobin peaks particularly early and is reliably detected within four hours of injury, making it potentially useful for very early diagnosis. However, myoglobin is relatively non-specific and it is troponin I and T (regulatory proteins with isoforms found only in cardiac myocytes) that have emerged as the most useful biochemical markers for diagnostic and prognostic purposes. Raised concentrations of troponins are reliably detected within 12 hours of injury, and are highly specific for myocardial infarction and for the “minimal myocardial damage” that may occur following transient or subocclusive thrombus formation in unstable angina.
Minimal damage of this type is now recognised as a powerful predictor of subsequent ischaemic events. Troponins are therefore finding special application for risk stratification in unstable angina.7 A recent study found that troponin T ⩾ 0.10 μg/l in patients with acute coronary syndromes was associated with a 30 day mortality rate of 10.4% compared with only 3.2% in troponin negative patients.8 Similarly, troponin positivity in acute myocardial infarction is associated with a substantially higher risk of future events. These findings are consistent with those of other investigators and have led to recommendations for troponin based risk management in acute coronary syndromes, with troponin positive patients a target for more aggressive strategies.
Predischarge risk stratification
Many high risk patients with coronary syndromes can be clearly identified in the acute phase, but there remains a group that makes a largely uncomplicated early recovery, some of whom remain at high risk. This group, therefore, should be a target for predischarge risk stratification, although identification of high risk individuals may not be easy. Strategies for predischarge risk stratification include non-invasive evaluation of left ventricular function, tests for ongoing myocardial ischaemia (silent or stress induced), and tests for electrical instability.
Left ventricular function
Left ventricular function is one of the major determinants of long term risk. There is now clear evidence that specific treatment with angiotensin converting enzyme (ACE) inhibitors (probably also β blockers) can reduce that risk, and coronary bypass surgery may be particularly beneficial when left ventricular dysfunction is associated with multivessel coronary artery disease. For many patients clinical criteria are sufficient to exclude significant left ventricular dysfunction, and an analysis of data from the GUSTO 1 trial confirmed that in patients presenting with a first infarct, absence of anterior infarction, left bundle branch block, or acute phase pulmonary oedema accurately identified 94% of all patients with an ejection fraction ⩾ 40%.9 For the remainder, non-invasive evaluation of left ventricular function by echocardiography or radionuclide angiography is recommended in order to determine appropriate risk management.
Clinical criteria associated with an ejection fraction ⩾ 40% in acute myocardial infarction
First myocardial infarction in the absence of:
- –
- anterior infarction
- –
- left bundle branch block
- –
- acute phase pulmonary oedema
Myocardial ischaemia
Stress testing
Patients with ongoing symptomatic ischaemia early after acute coronary syndromes are usually regarded as a high risk group requiring urgent angiographic investigation. However, many patients who make an uncomplicated early recovery have inducible ischaemia (with or without symptoms) that is variably predictive of recurrent ischaemic events. Thus stress testing has a time honoured role for predischarge risk stratification, particularly in uncomplicated myocardial infarction. A symptom limited test using the Bruce protocol is recommended for most patients although for some, particularly the elderly, modified protocols may be more suitable. An abnormal stress test with ST depression may be predictive of recurrent ischaemic events and provides grounds for coronary arteriography with a view to revascularisation. Other markers of risk include low exercise tolerance (< 7 mets), failure of the blood pressure to rise normally during exercise, and exertional arrhythmias. Unfortunately, recent meta-analysis has shown that inducible ischaemia during treadmill testing has a low positive predictive value for death and myocardial infarction in the first year (fig 4), falling below 10% in patients who have received thrombolytic treatment.10 Nevertheless, when “non-ischaemic” risk criteria are considered, the treadmill may provide added clinical value, inability to perform a stress test and low exercise tolerance both being independently predictive of recurrent events.11 Moreover, the negative predictive accuracy of predischarge stress testing is high, those with a normal test usually having a good prognosis without the need for additional investigation. Finally, it should be noted that the diagnostic value of exertional ST depression and reversible thallium perfusion defects is equivalent, making the treadmill a more cost effective strategy for risk stratification after myocardial infarction than the gamma camera.10 Predischarge stress testing has also been recommended in unstable angina, but although an ischaemic response at low work load has been associated with an increased risk, the positive predictive value of an abnormal test is low.
Treadmill stress testing for predischarge risk stratification
Positive predictive accuracy of ST depression < 10% after thrombolytic treatment
Inability to perform a stress test and low exercise tolerance are most useful predictors of recurrent events
Negative predictive accuracy is high
Diagnostic value of exertional ST depression and thallium perfusion defects are equivalent, making the treadmill more cost effective than the gamma camera
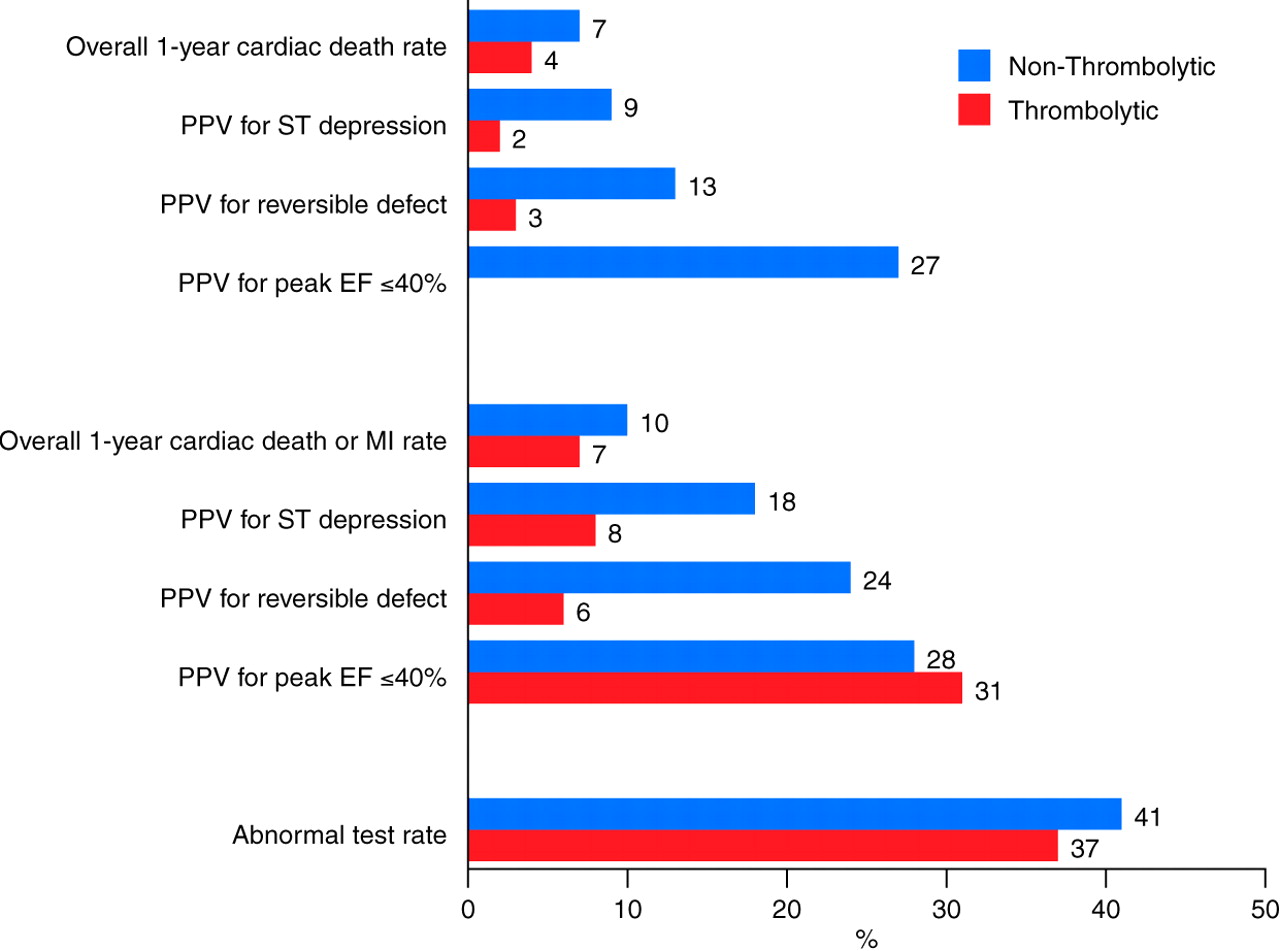
Positive predictive value (PPV) of non-invasive tests in non-thrombolytic and thrombolytic treated patients for cardiac death or reinfarction rates, and rates of abnormal tests. EF, ejection fraction. Reproduced from Shaw et al10 with permission.
Holter ST monitoring
Ambulatory ischaemia during predischarge Holter monitoring also identifies patients at risk of recurrent ischaemic events. In unstable angina its use is well documented; although it provides prognostic information additional to that available from the admission ECG, its incremental value relative to stress testing is not clear. In myocardial infarction ischaemic ST shift during predischarge Holter monitoring has a positive predictive value for recurrent infarction and death of 20%, and provides prognostic information that is additional to and independent of that obtained from stress testing and clinical assessment.12 Preliminary evidence suggests therefore that ambulatory ischaemia during Holter monitoring may be more useful than stress testing for risk stratification in acute coronary syndromes. It can certainly be applied earlier after admission when risk is greatest, but it is unlikely to become more widely used until further studies are available defining its role.
Electrical instability
Patients at greatest risk of arrhythmic death in the first year are those with extensive myocardial injury evidenced by Q waves, anterior infarction, left bundle branch block, or heart failure. Risk is further increased if late ventricular arrhythmias (frequent ectopy, ventricular tachyarrhythmia, ventricular fibrillation) occur before discharge.13 Because there are no well defined strategies for reducing the risk of arrhythmic death, routine electrocardiographic monitoring (Holter, telemetry) before discharge is not recommended although patients who declare themselves clinically with sustained ventricular arrhythmias require investigation to identify provocative factors (ischaemia, hypoxaemia, metabolic derangement). Where possible β blockers should be prescribed, based on evidence of efficacy in protecting against sudden death, but resistant life threatening arrhythmias require cardiac catheterisation to examine the potential for revascularisation. Electrophysiological investigation using programmed stimulation, though recommended by certain investigators, has proved unreliable for guiding treatment and predicting mortality.
Heart rate variability analysis
Holter monitoring after myocardial infarction permits analysis of autonomic function by measurement of heart rate variability. Sympathovagal balance is usually reduced in the postinfarction period, and the severity of the derangement is predictive of outcome, particularly arrhythmic and sudden death, but also all cause mortality.14 At present, however, it is not clear if heart rate variability analysis provides incremental data for risk stratification, or what the therapeutic implications of reduced heart rate variability should be. Similar considerations apply to unstable angina.
Signal averaged ECG
Ventricular late potentials detected by signal averaging are predictive of arrhythmic events late after myocardial infarction. Again, however, the therapeutic implications of ventricular late potentials are not well defined and the role, if any, in unstable angina is unknown.
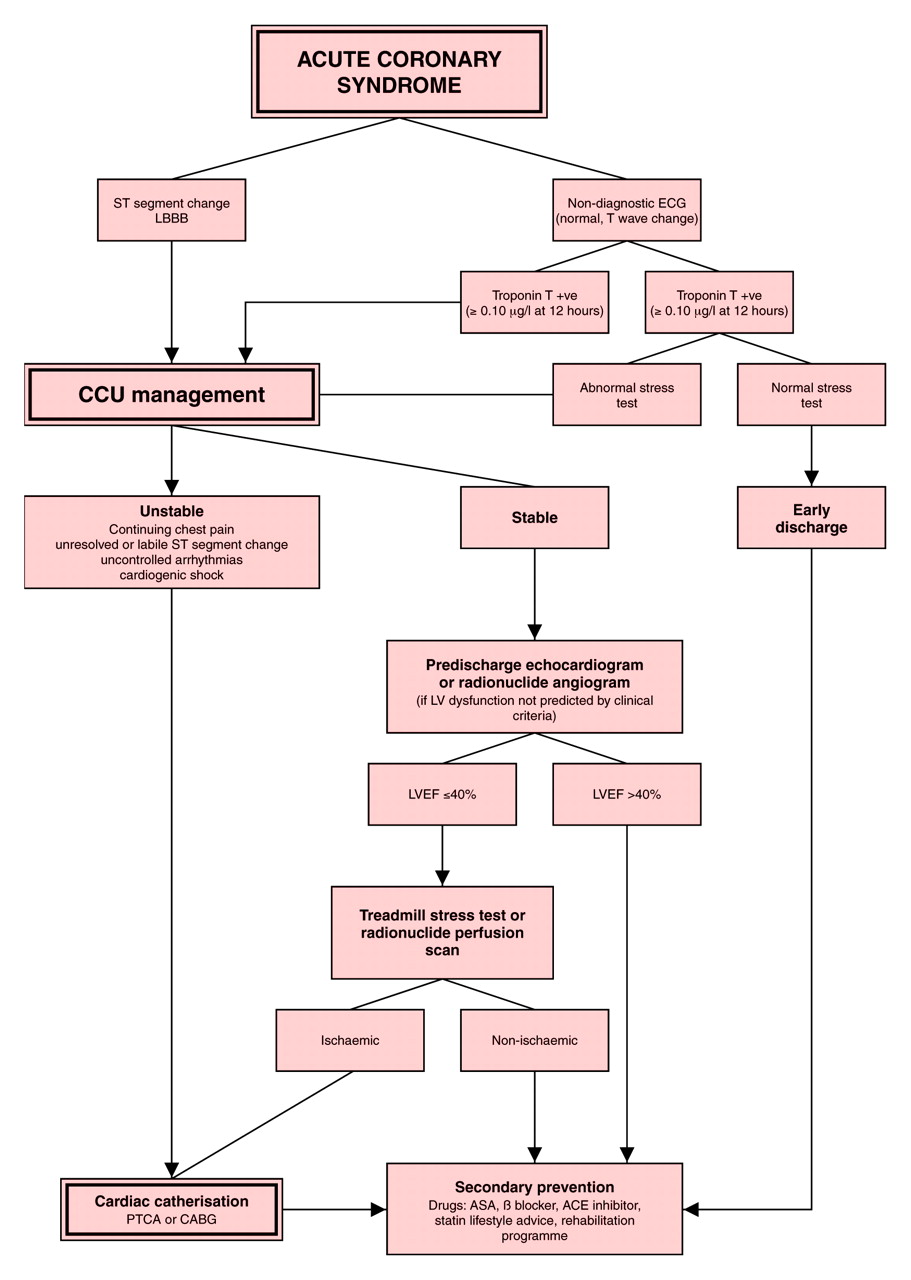
Practical recommendations
In patients with acute coronary syndromes, management should be risk based from the time of arrival in the emergency room (fig 5). An ECG and troponin assay should be obtained immediately with repeat troponin assay at 12 hours.15 Patients with regional ST change (elevation or depression) or left bundle branch block are a high risk group requiring admission to the coronary care unit and appropriate antithrombotic treatment. Patients with an ECG that is normal, or shows non-diagnostic T wave changes, should be treated similarly if troponin assay is positive, but if troponins are negative at 12 hours further management should be guided by the results of a stress test. An abnormal stress test requires further cardiac investigation and treatment, but if the stress test is normal then risk is very low, permitting early discharge pending review of the diagnosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for risk management in acute coronary syndromes. CCU, coronary care unit; LBBB, left bundle branch block; LVEF, left ventricular ejection fraction; PTCA, percutaneous transluminal coronary angioplasty; CABG, coronary artery bypass grafting; ASA, acetylsalicylic acid (aspirin); ACE, angiotensin converting enzyme.
If ST elevation or depression fails to respond promptly to treatment or recurs after early resolution, the risk of ongoing myocardial injury is considerable and urgent cardiac catheterisation is recommended with a view to revascularisation. Similar considerations apply to patients with unrelieved or recurrent cardiac chest pain. Invasive management may also be required for heart failure and late ventricular arrhythmias, particularly if responses to initial treatment are unsatisfactory or there is evidence of residual ischaemia or stunning.
For patients in whom the hospital course is uncomplicated, discharge at five days is usually possible. If clinical criteria are insufficient to exclude significant left ventricular dysfunction, a predischarge echocardiogram should be obtained, those with an ejection fraction ⩽ 40% representing a high risk group requiring ACE inhibition and also cardiac catheterisation if there is residual ischaemia on stress testing. Those with well preserved left ventricular function are a low risk group in whom stress testing is not usually helpful for risk assessment. Nevertheless, for troponin positive patients with unstable angina or non-Q wave infarction, risk is high and a predischarge stress test is recommended.
Regardless of the hospital course, all patients should receive secondary prevention with aspirin and, when possible, β blockers. Aggressive management of diabetes and dyslipidaemia is essential and ACE inhibitors should be given to patients who have had clinical evidence of heart failure. A cardiac rehabilitation course should be available for all patients recovering from acute coronary syndromes.
References
Supplementary materials
- Additional references for: Acute coronary syndromes: risk stratification. Timmis A.
Heart 2000;83:241�6.Bayes de Luna A, Coumel P, Leclercq JF. Ambulatory sudden cardiac death: mechanisms of protection of fatal arrhythmia on the basis of data from 157 cases. Am Heart J 1989;117:151�9.
Epstein SE, Palmari ST, Patterson RE. Evaluation of patients after acute myocardial infarction: indications for cardiac catheterisation and surgical intervention. N Engl J Med 1982;307:1487�92.
DeBusk RF, Glomqvist CG, Kouchoukos NT, et al. Identification and treatment of low-risk patients after acute myocardial infarction and coronary artery bypass graftsurgery. N Engl J Med 1986;314:161�6.
Cannon CP, Thompson B, McCabe CH, et al. Predictors of non-Q-wave acute myocardial infarction in patients with acute ischemic syndromes: an analysis from the thrombolysis in myocardial ischemia (TIMI) trials. Am J Cardiol 1995;75:977�81.
Timmis AD. Probability analysis in the diagnosis of coronary artery disease. BMJ 1985;291:1443�4.
ISIS-1 Collaborative Group. Randomised trial of intravenous atenolol among 16027 cases of suspected acute myocardial infarction: ISIS-1. Lancet 1986;ii:57�65.
ISIS-1 Collaborative Group. Mechanisms for the early mortality reduction produced by beta-blockade started early in acute myocardial infarction: ISIS-1. Lancet 1988;i:921�3.
Pfeffer MA, Braunwald E, Moye LA, et al, on behalf of the SAVE Investigators. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction: results of the survival and ventricular enlargement trial. N Engl J Med 1992;327:669�77.
Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. Lancet 1993;342:821�8.
CIBIS-II Investigators and Committees. The cardiac insufficiency bisoprolol study ii (CIBIS-II): a randomised trial. Lancet 1999;353:9�13.
Holmes DR Jr, Bates ER, Kleiman NS, et al. Contemporary reperfusion therapy for cardiogenic shock: the GUSTO-I trial experience. J Am Coll Cardiol 1995;26:668�74.
Hochman JS, Sleeper LA, Webb JG, et al, for the SHOCK Investigators. Early revascularisation in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med 1999;341:625�34.
FRagmin and Fast Revascularisation during InStability in Coronary artery disease (FRISCII) Investigators. Invasive compared with non-invasive treatment in unstable coronary artery disease:FRISC II prospective randomised multicentre study. Lancet 1999;354:708�15.
Laji K, Wilkinson P, Ranjadayalan K, et al. Prognosis in acute myocardial infarction: comparison of patients with diagnostic and nondiagnostic electrocardiograms. Am Heart J 1995;130:705�10.
Braunwald E. Unstable angina: a classification. Circulation 1989;80:410�14.
Clemmensen P, Ohman EM, Sevilla DC, et al. Changes in standard electrocardiographic ST-segment elevation predictive of successful reperfusion in acute myocardial infarction. Am J Cardiol 1990;66:1407�11.
Schroder R, Dissmann R, Bruggemann T, et al. Extent of early ST segment elevation resolution: a simple but strong predictor of outcome in patients with acute myocardial infarction. J Am Coll Cardiol 1994;24:384�91.
Hogg KJ, Hornung RS, Howie CA, et al. Electrocardiographic prediction of coronary artery patency after thrombolytic treatment in acute myocardial infarction: use of ST segment as a noninvasive marker. Br Heart J 1988;60:275�80.
GUSTO Angiographic Investigators. The effects of tissue plasminogen activator, streptokinase or both on coronary-artery patency, ventricular function, and survival after acute myocardial infarction. N Engl J Med 1993;329:1615�22.
TIMI Study Group. The thrombolysis in myocardial infarction trial. Phase 1 findings. N Engl J Med 1985;312:932�6.
Ellis SG, da Silva ER, Heyndrickx G, et al. Randomized comparison of rescue angioplasty with conservative management of patients with early failure of thrombolysis for acute anterior myocardial infarction. Circulation 1994;90:2280�4.
Archbold RA, Sayer JW, Suliman A, et al. Frequency and prognostic implications of conduction defects in acute myocardial infarction since the introduction of thrombolytic therapy. Eur Heart J 1998;19:893�8.
Bigger JT Jr, Fleiss JL, Kleiger R, et al. The relationship among ventricular arrhythmias, left ventricular dysfunction, and mortality in the two years after myocardial infarction. Circulation 1984;69:250�8.
Jacoby RM, Nesto RW. Acute myocardial infarction in the diabetic patient: pathophysiology, clinical course and prognosis. J Am Coll Cardiol 1992;20:736�44.
Malmberg K, Ryden L, Efendic S, et al. Randomized trial of insulin-glucose infusion followed by subcutaneous insulin treatment in diabetic patients with acute myocardial infarction (DIGAMI study): effects on mortality at 1 year. J Am Coll Cardiol 1995;26:57�65.
The 4S Study Group. Randomised trial of cholesterol in 4444 patients with coronary heart disease: the Scandinavian simvastatin study. Lancet 1994;344:1382�9.
Sacks F, Pfeffer M, Moye L, et al. The effects of pravastatin on coronary events after myocardial infarction in patients with average cholesterol. N Engl J Med 1996;335:l00l-9.
Wood D, Durrington P, McInnes G, et al, for British Cardiac Society, British Hyperlipidaemia Association, British Hypertension Society, endorsed by British Diabetic Association. Joint British recommendations on prevention of coronary heart disease in clinical practice. Heart 1998;80(suppl 2):S6�12.
Ravkilde J, Nissen H, Horder M, et al. Independent prognostic value of serum creatine kinase isoenzyme MB mass, cardiac troponin T and myosin light chain levels in suspected acute myocardial infarction. J Am Coll Cardiol 1995;25:574�81.
Holmvang L, Luscher MS, Clemmensen P, et al, and the TRIM Study Group. Very early risk stratification using combined ECG and biochemical assessment in patients with unstable coronary artery disease. Circulation 1998;98:2004�9.
Woo J, Lacbawan F, Sunheimer R, et al. Is myoglobin useful in the diagnosis of acute myocardial infarction in the emergency department setting. Am J Clin Pathol 1995;103:725�9.
Mair J, Artner-Dworzak E, Lechleitner, et al. Cardiac troponin T in diagnosis of acute myocardial infarction. Clin Chem 1991;37:845�52.
Adams JE, Bodor GS, Davila-Roman VG, et al. Cardiac troponin I: a marker with high specificity for cardiac injury. Circulation 1993;88:101�6.
Antman EM, Tanasijevic MJ, Thompson B, et al. Cardiac specific troponin I levels predict the risk of mortality in patients with acute coronary syndromes. N Engl J Med 1996;335:1342�9.
Newby LK, Christenson RH, Ohman EM, et al. Value of serial troponin T measures for early and late risk stratification in patients with acute coronary syndromes. The GUSTO-IIa investigators. Circulation 1998;98:1853�9.
Stubbs P, Collinson P, Moseley D, et al. Prognostic significance of admission troponin T concentrations in patients with myocardial infarction. Circulation 1996;94:1291�7.
CAPTURE Study Investigators. Benefit of abciximab in patients with refractory unstable angina in relation to serum troponin T levels. N Engl J Med 1999;340:1623�9.
Multicenter Post-Infarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med 1983;309;321�6.
Sanz G, Castaner A, Betriu A, et al. Determinants of prognosis in survivors of myocardial infarction: a prospective clinical angiographic study. N Engl J Med 1982;306:1065�70.
Greenberg H, McMaster P, Dwyer EM Jr. Left ventricular dysfunction after acute myocardial infarction: results of a prospective multicenter study. J Am Coll Cardiol 1984;4:867�74.
Holmes DR Jr, Davis KB, Mock MB, et al. The effect of medical and surgical treatment on subsequent sudden cardiac death in patients with coronary artery disease: a report from the coronary artery surgery study. Circulation 1986;73:1254�63.
Stevenson R, Umachandran V, Ranjadayalan K, et al. Reassessment of treadmill stress testing for risk stratification in patients with acute myocardial infarction treated by thrombolysis. Br Heart J 1993;70:415�20.
Wilcox I, Freedman SB, Allman KC, et al. Prognostic significance of a predischarge exercise test in risk stratification after unstable angina pectoris. J Am Coll Cardiol 1991;18:677�83.
Gill JB, Cairns JA, Roberts RS, et al. Prognostic importance of myocardial ischemia detected by ambulatory monitoring early after acute myocardial infarction. N Engl J Med 1996;334:65�70.
McComb JM, Gold HK, Leinbach RC, et al. Electrically induced ventricular arrhythmias in acute myocardial infarction treated with thrombolytic agents. Am J Cardiol 1988;62:186�91.
Willems AR, Tijssen JG, van Capelle FJ, et al. Determinants of prognosis in symptomatic ventricular tachycardia or ventricular fibrillation late after myocardial infarction. The Dutch ventricular tachycardia study group of the Interuniversity Cardiology Institute of The Netherlands. J Am Coll Cardiol 1990;16:521�30.
Pedretti R, Etro MD, Laporta A, et al. Prediction of late arrhythmic events after acute myocardial infarction from combined use of noninvasive prognostic variables and inducibility of sustained monomorphic ventricular tachycardia. Am J Cardiol 1993;71:1131�41.
Bigger JT Jr, Fleiss JL, Rolnitzky LM. Prevalence, characteristics and significance of ventricular tachycardia detected by 24-hour continuous electrocardiographic recordings in the late hospital phase of acute myocardial infarction. Am J Cardiol 1986;58:1151�60.
Yusuf S, Lessem J, Jha P, et al. Primary and secondary prevention of myocardial infarction and strokes: an update of randomly allocated controlled trials. J Hypertens 1993;11(suppl 4):S61�73.
Beta-Blocker Heart Attack Trial Research Group. A randomized trial of propranolol in patients with acute myocardial infarction. I. Mortality results. JAMA 1982;247:1707�14.
Echt DS, Liebson PR, Mitchell LB, et al. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The cardiac arrhythmia suppression trial. N Engl J Med 1991;324:781�8.
Waldo AL, Camm AJ, deRuyter H, et al. Effect of d-sotalol on mortality in patients with left ventricular dysfunction after recent and remote myocardial infarction. The SWORD investigators: survival with oral d-sotalol. Lancet 1996;348:7�12.
Breithardt G, Borggrefe M, Quantius B, et al. Ventricular vulnerability assessed by programmed ventricular stimulation in patients with and without late potentials. Circulation 1983;68:275�81.
Breithardt G, Borggrefe M, Haerten K. Ventricular late potentials and inducible ventricular tachyarrhythmias as a marker for ventricular tachycardia after myocardial infarction. Eur Heart J 1986;7:127�34.
Nalos PC, Gang ES, Mandel WJ, et al. The signal-averaged electrocardiogram as a screening test for inducibility of sustained ventricular tachycardia in high risk patients: a prospective study. J Am Coll Cardiol 1987;9:539�48.
Greenspan AM. Can electrophysiologic testing predict mortality after myocardial infarction? J Am Coll Cardiol 1986;7:124�34.
Santarelli P, Bellocci F, Loperfido F, et al. Identification of patients at risk of sudden death after myocardial infarction: is there a role for programmed ventricular stimulation? Clin Prog Electrophysiol Pacing 1985;3:115�23.
Appel ML, Berger RD, Saul JP, et al. Beat to beat variability in cardiovascular variables: noise or music? J Am Coll Cardiol 1989;14:1139�48.
Vaishnav S, Stevenson R, Marchant B, et al. The relation between heart rate variability early after acute myocardial infarction and long-term mortality. Am J Cardiol 1994;73:653�7.
Kuchar DL, Thorburn CW, Sammel NL. Late potentials detected after myocardial infarction: natural history and prognostic significance. Circulation 1986;74:1280�9.
Seino Y, Tomita Y, Takano T, et al. Early identification of cardiac events with serum troponin T in patients with unstable angina. Lancet 1993;342:1236�7.