Article Text

Statistics from Altmetric.com
In 180, several reports appeared almost simultaneously of the identification of normal cardiac anatomy in fetal life. The recognition of several different forms of structural cardiac anomaly followed soon after. At this time, cardiac evaluation was confined to pregnancies at increased risk of congenital heart disease (CHD), such as those with a family history of CHD or where extracardiac malformations had been detected. However, up to 90% of CHD occurs in pregnancies where there are no known high risk features. For this reason, in 1985 a group based in Paris put forward the idea of teaching the obstetrician to assess the heart in a simplified form during routine obstetric scanning, which was well established at that time in France. As a result, four chamber view scanning became an integral part of the fetal anatomical survey in many countries by the end of the 1980s. In the early 1990s, some authors suggested extending the cardiac assessment to include great artery scanning in order to detect a higher proportion of cases of major congenital heart disease.1 If cardiac screening is confined to the four chamber view, about 2/1000 studies will be abnormal and would represent about 60% of the major heart disease seen in infants. If the great arteries are also examined, about 3/1000 cases would be abnormal, and over 90% of major heart disease would be detectable prenatally. Therefore, in ideal circumstances, the vast majority of serious heart malformations could be detected before 20 weeks' gestation. Unfortunately, the reality is far from this for several reasons:
differing policies for obstetric scanning
differing guidelines for scanning
differing skill at scanning.
About 2% of live births have fetal structural malformations, the majority of which can be detected by ultrasound. About 25% of these malformations are cardiac in nature and about half of these are serious or life threatening. Despite these facts, and the opportunity during pregnancy for comprehensive evaluation of the fetal anatomy in fine detail, there is no universal agreement as to either the necessity for or the technique of fetal anatomical scanning. Some countries, such as Norway, France, and Germany, have instituted a government sponsored policy for routine anatomical screening by ultrasound. In the UK, routine screening is generally well accepted but not uniformly adopted or standardised in all parts of the country. In the USA, routine scanning is not recommended but is allowed only for specific indications, although these are fairly all encompassing. In practice, this leads to later scanning in the US and “targeted” scanning rather than a comprehensive anatomical survey.
Where an anatomical survey is performed, the timing of the scan varies—for example, in France it is usually between 20–22 weeks, in Norway 18 weeks. In general, the later in the mid-trimester that scanning is performed the more successful will be the detection of abnormalities, partly because scanning becomes easier and partly because some lesions become more evident as pregnancy advances. However, later detection of malformations will limit the options for interrupting the pregnancy or make it much more difficult both emotionally for the parents and technically for the obstetrician. Thus, the ideal policy would be a universal anatomical scan at a compromise time of between 18–20 weeks' gestation.
Although there are recommended guidelines for the technique of fetal scanning provided by the Royal College of Obstetricians and the American Colleges of Obstetrics and of Radiology, none are enforced and there is no standardisation of practice. This would be much easier in the UK than in the US and could be universally computerised to a standard format, but to my knowledge this is still not happening.
The skill involved in scanning is extremely variable for several reasons. A sonographer, whether a technician, an obstetrician, or a radiologist, needs:
to train with a high volume of patients
to maintain skills continuously with sufficient numbers of patients
to be exposed continually to a critical number of abnormal fetuses
to be provided with constant feedback and retraining.
In order to achieve and maintain a high level of expertise in scanning, the practitioner should be doing this as a full time or nearly full time commitment. Where ultrasound is performed in small numbers, the requisite practice necessary is quite unattainable. Nearly all scanning in the UK is hospital based, with delivery numbers usually over 2000 per year. Therfore, the necessary volume of patients is less of a problem in the UK than in the US, where scanning often takes place in private offices in small numbers.
As a result of the differing policies and standards in obstetric ultrasound, the results of the detection of all malformations in the screening setting varies with the organ involved, but is particularly poor in reference to the heart. During screening, reported detection rates vary between 4.5% and 96% for major CHD, with the most papers giving a rate of 15–20%.2-6 This is consistent with recent experience in our referral centre for paediatric cardiology, when 18% of infants requiring cardiac surgery in the first year of life during 1998 were identified prenatally. The rate of detection of four chamber view anomalies prenatally is better, but averages only about 50%,7 ,8 despite the fact that universally nearly all pregnancies are scanned at least once (figs 1, 2, and 3). Thus, the technology and personnel are in place in obstetric care, but they are not used to their maximum capability.

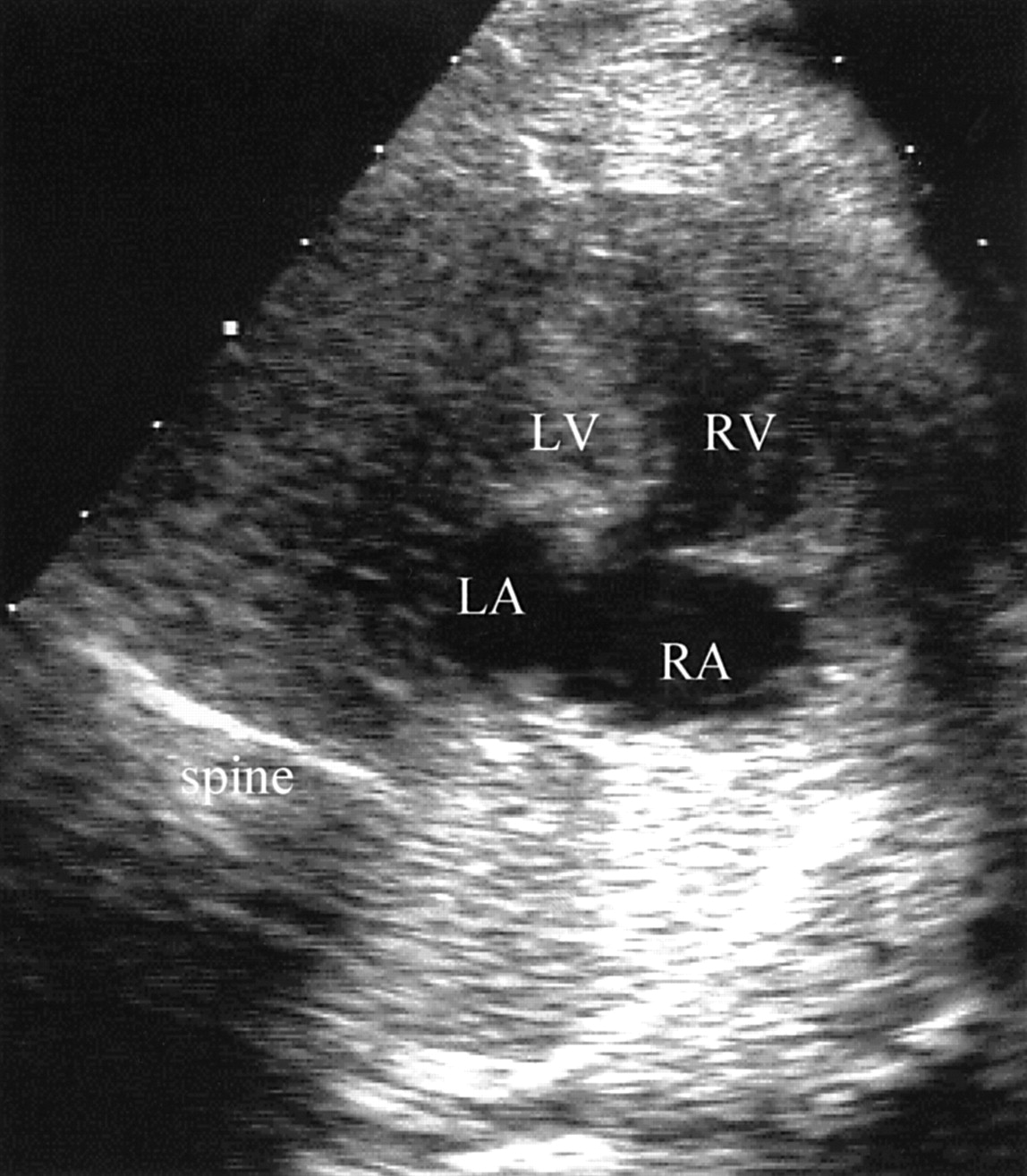
A normal four chamber view showing a heart of normal size (about one third of the thorax) in a normal position within the thorax (about 45° to the midline). There are two equally sized atria and two equally sized ventricles. In the moving image both atrioventricular valves would be seen to open equally. There is a “cross” at the crux of the heart, where the atrial and ventricular septum meet at the insertion of the two atrioventricular valves. LA, left atrium; RA, right atrium; LV, left ventricle; RV, right ventricle.

The fetal heart is oriented similarly to the normal example seen in fig 1. The most common anomaly detected prenatally is depicted. There is no “cross” appearance at the crux of the heart owing to a common atrioventricular junction and a complete atrioventricular septal defect. Despite the obvious difference between this and the four chamber view of the normal heart, only about 50% of cases are detected in fetal life.

{kind=link}
{kind=link}
{kind=link}
This fetal heart is oriented similarly to the normal example shown in fig 1. The second most common anomaly detected prenatally is depicted. The left atrium is small. The left ventricle is hypoplastic with the right heart forming the apex. The mitral valve is not patent. This is mitral atresia, in its most frequent setting of the hypoplastic left heart syndrome. Again, this defect is only detected prenatally in just over half of cases.
Cardiac evaluation at referral to paediatric cardiologists
A common misconception among paediatric cardiologists is that fetal cardiology is the same as paediatric echocardiography but a bit smaller. Therefore, nearly all paediatric echocardiographers in the US would not hesitate to offer fetal echocardiography as part of their practice. However, it is clear that quite a different spectrum of disease is seen prenatally,9 and fetal heart scanning is quite a different skill. Success in accurate diagnosis will be partly dependent on technical skills, which again require training and practice. In the US, there are recommended guidelines for training, and a minimum number of scans in order to maintain skills, but these are not commonly known and certainly are not adhered to. Experience of fetal malformations therefore is so diluted that few practitioners have sufficient numbers to maintain a high standard of expertise. In addition, most paediatric cardiologists know little of fetal medicine and obstetric pathology, which have an important influence on fetal cardiac evaluation.
Although the majority of paediatric cardiology centres in the UK now offer fetal echocardiography, this is usually confined to one or two cardiologists and, theoretically, there should be sufficient numbers in each regional centre to provide adequate experience. However, there is no system of independent review or systematic quality control in place anywhere, to my knowledge. Indeed, in the US, pathological correlation after termination of pregnancy is quite rare for various reasons, not least being the difficulty in obtaining remuneration for pathological services, despite their vital role in quality control.
Problems and limitations
Limitations of fetal echocardiography are related to:
image quality
subtle lesions, such as small ventricular septal defects
developing or progressive lesions
lesions which are undetectable before birth.
Image quality is dependent on the skill and experience of scanning in addition to local factors such as gestational age, fetal position, and the thickness of the maternal abdomen. Maternal obesity is an increasing problem everywhere but particularly in the US, especially in the poorer states. This is the most important limitation to image quality, which in turn will limit confidence in excluding malformations in the fetus in any anatomical system. Even though the resolution of ultrasound equipment has improved vastly since the early 1980s, a great deal more detail is also expected during fetal scanning, and there are a significant proportion of patients where detail is just not possible because of the way scanning is presently organised. As up to 10% of adult Americans are said to be morbidly obese, this group should probably be managed with a different strategy, perhaps with early transvaginal scanning instead of transabdominal scans; to date this problem has not been addressed by the ultrasound community.
In a small proportion of fetuses, CHD becomes evident or more evident as pregnancy progresses.3 Thus, the cardiac evaluation can be normal at 18 weeks although a significant malformation is found later or at birth. This is true of some cases of aortic or pulmonary stenosis, cardiac tumours, or cardiomyopathies. It is rare for a life threatening malformation to arise after 20 weeks' gestation, but it can occur. In addition, minor lesions can be overlooked because of the limits of ultrasound resolution, such as small ventricular septal defects; a persistent arterial duct and an atrial septal defect cannot be predicted prenatally as these communications are always present prenatally. Thus, there are confidence limits with even detailed fetal heart scanning. It is important to realise, however, that confidence limits may be much wider with poor image quality.
Latest technologies
By 14 weeks' gestation, the cardiac connections can be identified in many patients transabdominally. The connections can be seen in almost all patients at this stage transvaginally, however, and in much finer detail than on the transabdominal scan. Expertise with this technique is essential and the paediatric cardiologist should use the experienced gynaecological technician to display the fetal cardiac images, in a setting where transvaginal scanning is routine. At present, a cardiac scan at 14 weeks is confined to the high risk patient, such as those with a family history of CHD or those whose fetus has been found to have an increased nuchal fold.
The data concerning nuchal translucency in early pregnancy (10–12 weeks) are fascinating and intriguing.10 When the translucent region at the back of the neck is increased in size, there is a high incidence of associated chromosomal anomalies, cardiac malformations, or both, with the incidence of heart disease increasing with increasing nuchal thickness. Conversely, 50% of fetuses subsequently found to have CHD had an abnormal nuchal fold measurement. This may reflect the “insult” which has caused the fetal heart malformation. Extension of the nuchal translucency screening program, which has received little attention in the US so far, is likely to have important implications for the improved detection of both chromosomal and cardiac malformations. In addition, the earlier the diagnosis of fetal malformation is made in pregnancy, the more likely are parents to choose interruption. If a pregnancy with increased nuchal thickening is continuing, fetal echocardiography is recommended, ideally at 14 weeks, which is the earliest time a cardiac scan can be completely comprehensive.
Impact on paediatric cardiology
The impact on paediatric cardiology may include:
reduced prevalence of CHD, especially complex forms
improved morbidity after delivery and perioperatively
improved perioperative mortality.
Decisions about termination of pregnancy are influenced by many different factors, including gestational age at diagnosis, social circumstances, and socioeconomic group. Generally speaking, however, if complex heart disease is detected in a pregnancy at less than 20 weeks' gestation, over half the parents will choose to interrupt the pregnancy. This is true in the UK and the US. Thus, about half of the complex forms of CHD which the paediatric cardiologist would expect to see and treat postnatally may only be seen once in prenatal life. As fetal cardiology preferentially detects the complex forms of heart disease which require long term cardiac care and follow up, this is bound to have an impact on paediatric cardiology in the future. As an example of this, termination of pregnancy has been shown to have lowered the prevalence of pulmonary atresia in England and Wales, compared with Scotland and Ireland where either the diagnosis was not made in the fetus or termination was not chosen.11 The frequency of complex one ventricle type cardiac repairs may therefore become less common in the coming years.
Some forms of CHD are associated with early decompensation and even death of the infant before the malformation can be recognised and treated. This applies mainly to those where either the pulmonary or systemic circulation is dependent on the patency of the arterial duct, or the lesions which require “mixing” at an adequate atrial septal defect such as transposition of the great arteries or total anomalous pulmonary venous drainage. It appears intuitively obvious that if CHD is recognised prenatally and delivery takes place in or near a paediatric cardiology centre, thus avoiding delay in diagnosis and emergency transfer of a sick neonate, the morbidity for the infant will be minimised. This has been shown in several studies although improvement in mortality has been harder to prove, partly because fetal echocardiography preferentially detects more severe forms of CHD which have a higher mortality per se.12 ,13 However, a recent study of infants with transposition of the great arteries, where there were adequate numbers to answer this question, showed conclusively that there was a much lower mortality in those cases prenatally diagnosed.14 Thus, the impact on paediatric cardiology, if fetal heart scanning improved to the ideal level of expertise, would be a decrease in the number of complex malformations, but those patients with CHD who come to surgery would do so in optimum status without prior insult. This would have a potentially significant effect on saving of resources by reducing complex disease and improving both the cardiac and neurological outlook for the survivors of treatment.
Medico-legal aspects
Certainly in the US, and increasingly in the UK, one is continually aware of the fear of litigation. One would imagine that this would result in more rigid standards and codes of practice in the US, but in reality this does not appear to happen. Litigation is so sporadic, and frequently occurs in the most unexpected circumstances, that it does not seem to deter careless attention to training or practice guidelines. In the case of an obstetrician who misses a four chamber view anomaly on a prenatal scan, the parents can sue for wrongful life. To my knowledge there is no precedent for this in court, although out of court settlements have been made in such circumstances. However, the RADIUS study was a large multicentre scanning program based in the midwest and eastern US, where no cardiac malformation was detected outside tertiary centres, despite a supposedly uniform scanning format.15 This publication gives the obstetrician a reasonable defence that such malformations are not detectable by the present general “standard of care”. A little threat of litigation may be no bad thing if it encourages self regulation within the medical profession, uniform codes of practice, and quality control initiated by doctors themselves. However, an atmosphere of litigation, especially if the application and outcome of suits are extremely unpredictable, leads to bad clinical practice, with over investigation and over treatment.
Differences between the UK and the US
Some of the differences between the UK and the US in terms of the practice of fetal cardiology have been alluded to above. The most striking difference in medical practice is that in the UK there is, in general, an atmosphere of collective responsibility for the health service among doctors, and for the impact of care on society as a whole. Despite the dissatisfaction among the medical profession in the UK, which appears to have grown in the last 10 years, the organised nature of the UK National Health Service provides a unique opportunity for imposing and maintaining uniform standards of practice and for collecting data for quality control across the whole service. This would demand a willingness on the part of practitioners to be part of a drive to improve the quality of service and to confront the hazards of “audit”, but such an effort would be applicable to many aspects of obstetric and paediatric cardiology practice.