Article Text

Statistics from Altmetric.com
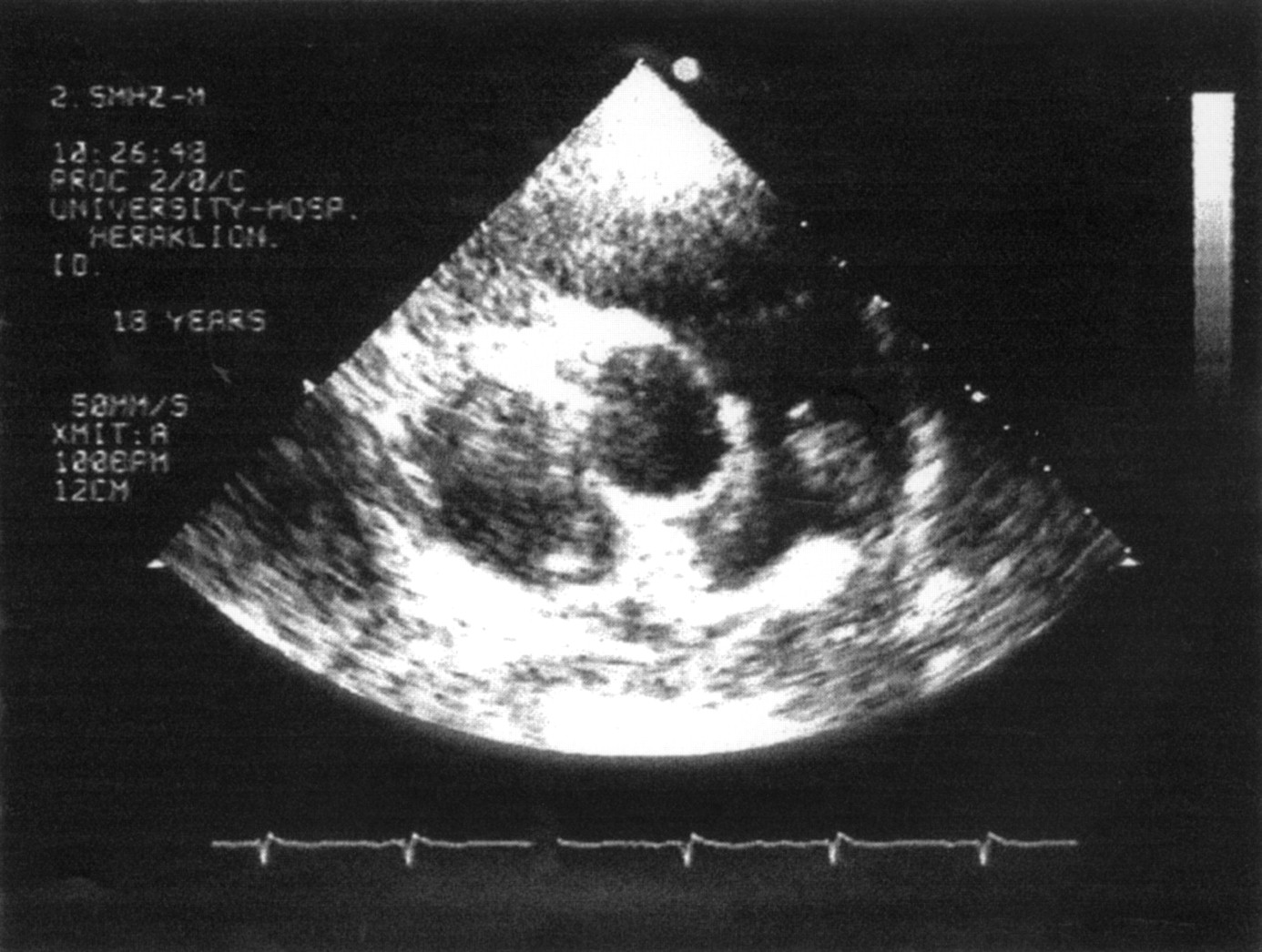
An 18 year old woman, without a previous history of cardiovascular disease, was referred for ultrasound examination because of pyrexia during the previous 40 days. Laboratory investigations produced three blood cultures with Streptococcus sanguis, while cardiac auscultation revealed only a soft systolic murmur at the second left intercostal space. Echocardiographic examination showed normal cardiac dimensions and function, normal valves with no vegetations, and no signs of pulmonary hypertension. In a modified short axis view at the level of the great arteries colour Doppler flow mapping revealed a tiny jet of retrograde flow in the main pulmonary area, indicative of patent ductus arteriosus (PDA). A large mobile mass was noted at the confluence of the left pulmonary artery, consistent with a vegetation at the entrance of the PDA (left). The discovery of this mass in a patient with streptococcus septicaemia led us to the diagnosis of PDA endarteritis. Following successful antibiotic treatment, surgery confirmed the presence of PDA; the ductus was closed and the mass was removed. Histological examination confirmed that the latter was vegetation. Estimation of the risk of infective endarteritis in patients with PDA is an important issue that affects clinical decision making. The classic continuous murmur is usually sufficient in itself for repair, in part to eliminate the risk of infective endarteritis. Although endarteritis may appear as a complication of clinically apparent PDA, it is not generally found in silent PDA, and its treatment with routine antibiotic prophylaxis and surgical closure is under discussion. However, as shown by our case, only the second such to be reported, the risk of infection still exists even in silent PDA.

{kind=link}