Article Text

Statistics from Altmetric.com
The aortic valve, and its supporting ventricular structures, form the centrepiece of the heart. All chambers of the heart are related directly to the valve, and its leaflets are incorporated directly into the cardiac skeleton. As such, the valve is the focus for the echocardiographer. Yet still the precise structure of its component parts remains controversial, with persisting disagreements relating largely to the enigmatic “annulus”. Indeed, it is difficult to find an unequivocal definition of the annulus, a structure appearing most frequently in the context of cardiac surgery.1
This review describes the arrangement of the aortic root in terms of the attachment of the aortic valvar leaflets, and their relations to the aorta and its ventricular support.2 Recognising that these parts will still be considered to represent an annulus, I will try to show that the ring like structure thus described has considerable length, encompassing the entirety of the semilunar attachments of the leaflets. It is the recognition of the relation of these attachments to the anatomic and haemodynamic ventriculo-arterial junctions which is the key to understanding.3
Location of the aortic root
Although forming the outlet from the left ventricle, when viewed in the context of the heart as it lies within the chest (“attitudinally correct orientation”4), the aortic root is positioned to the right and posterior relative to the subpulmonary infundibulum (fig 1). The subpulmonary infundibulum is a complete muscular funnel which supports in uniform fashion the leaflets of the pulmonary valve.5 In contrast, the leaflets of the aortic valve are attached only in part to the muscular walls of the left ventricle. This is because the aortic and mitral valvar orifices are fitted alongside each other within the circular short axis profile of the left ventricle, as compared to the tricuspid and pulmonary valves which occupy opposite ends of the banana shaped right ventricle (fig 2). When the posterior margins of the aortic root are examined, then the valvar leaflets are seen to be wedged between the orifices of the two atrioventricular valves (fig 3). Sections in long axis of the left ventricle then reveal the full extent of the root, which is from the proximal attachment of the valvar leaflets within the left ventricle to their distal attachments at the junction between the sinusal and tubular parts of the aorta (fig4).
In this normal human heart, viewed in attitudinally correct orientation, the subpulmonary infundibulum has been transected, and the pulmonary valve removed, showing the central position of the aortic root within the cardiac short axis.

The ventricular apexes have been amputated from this ventricular mass, and the base of the heart is shown from beneath in left anterior oblique orientation. Note the central location of the aortic valve, which is overlapped by the mitral valve within the short axis of the left ventricle. The tricuspid and pulmonary valves are separated by the supraventricular crest in the roof of the right ventricle. The dotted line shows the area of fibrous continuity between the leaflets of the aortic and mitral valves.

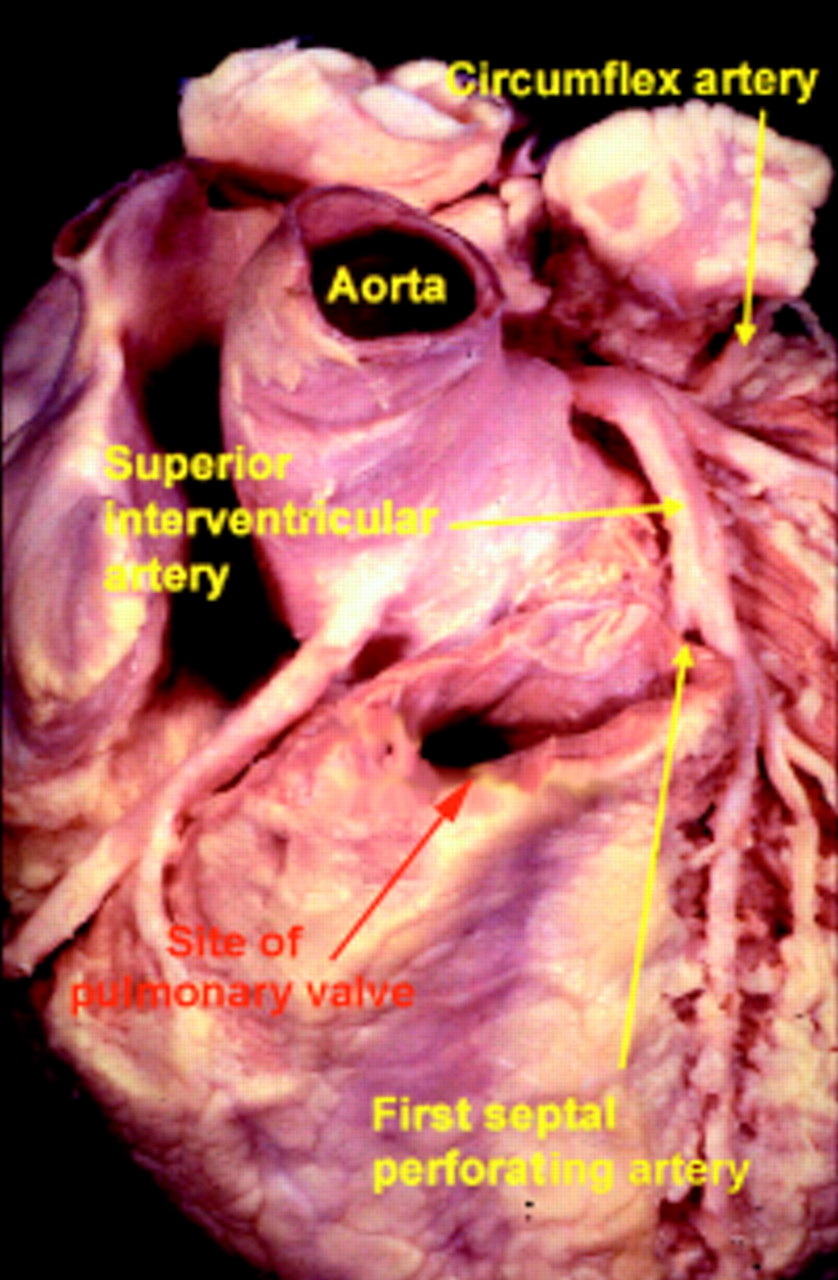
The short axis of the heart is photographed from above and from the right, producing a right posterior oblique orientation. Note that the aortic root is deeply wedged between the orifices of the mitral and tricuspid valves. Note also the origins of the coronary arteries from the sinuses of the aortic valve adjacent to the pulmonary trunk.

This is a close up of the aortic root, having sectioned the left ventricle along its own long axis. Note the length of the root between the basal attachments of the valvar leaflets and the sinutubular junction. Note also the thin areas of aortic wall which separate the left ventricular cavity from the pericardial space just below the level of the sinutubular junction.
How can we describe the aortic root?
Forming the outflow tract from the left ventricle, the aortic root functions as the supporting structure for the aortic valve. As such, it forms a bridge between the left ventricle and the ascending aorta. The anatomic boundary between the left ventricle and the aorta, however, is found at the point where the ventricular structures change to the fibroelastic wall of the arterial trunk. This locus is not coincident with the attachment of the leaflets of the aortic valve. As shown in fig 4, the leaflets are attached within a cylinder extending to the sinutubular junction of the aorta. The semilunar attachments of the leaflets themselves form the haemodynamic junction between left ventricle and aorta. All structures distal to these attachments are subject to arterial pressures, whereas all parts proximal to the attachments are subjected to ventricular pressures.
Opening out the aortic root shows the complexities of these relations (fig 5). The structures distal to the semilunar attachments are the valvar sinuses, into which the semilunar leaflets themselves open during ventricular systole. Two of these valvar sinuses give rise to the coronary arteries, usually at or below the level of the sinutubular junction (figs 3 and 4). The arrangement of the coronary arteries permits these two sinuses to be called the right and left coronary aortic sinuses. When their structure is examined, it can then be seen that, for the greater part, the sinuses are made up of the wall of the aorta. At the base of each of these coronary sinuses, however, a crescent of ventricular musculature is incorporated as part of the arterial segment (fig 6). This does not happen within the third, non-coronary, sinus. This is because the base of this sinus is exclusively fibrous in consequence of the continuity between the leaflets of the aortic and mitral valves (fig 5).

The aortic root has been opened through a longitudinal incision across the area of aortic-mitral valvar continuity, and spread open to show the semilunar attachments of the valvar leaflets. Note the interleaflet triangles extending to the sinutubular junction, and the crescents of myocardium at the base of the two coronary aortic sinuses.
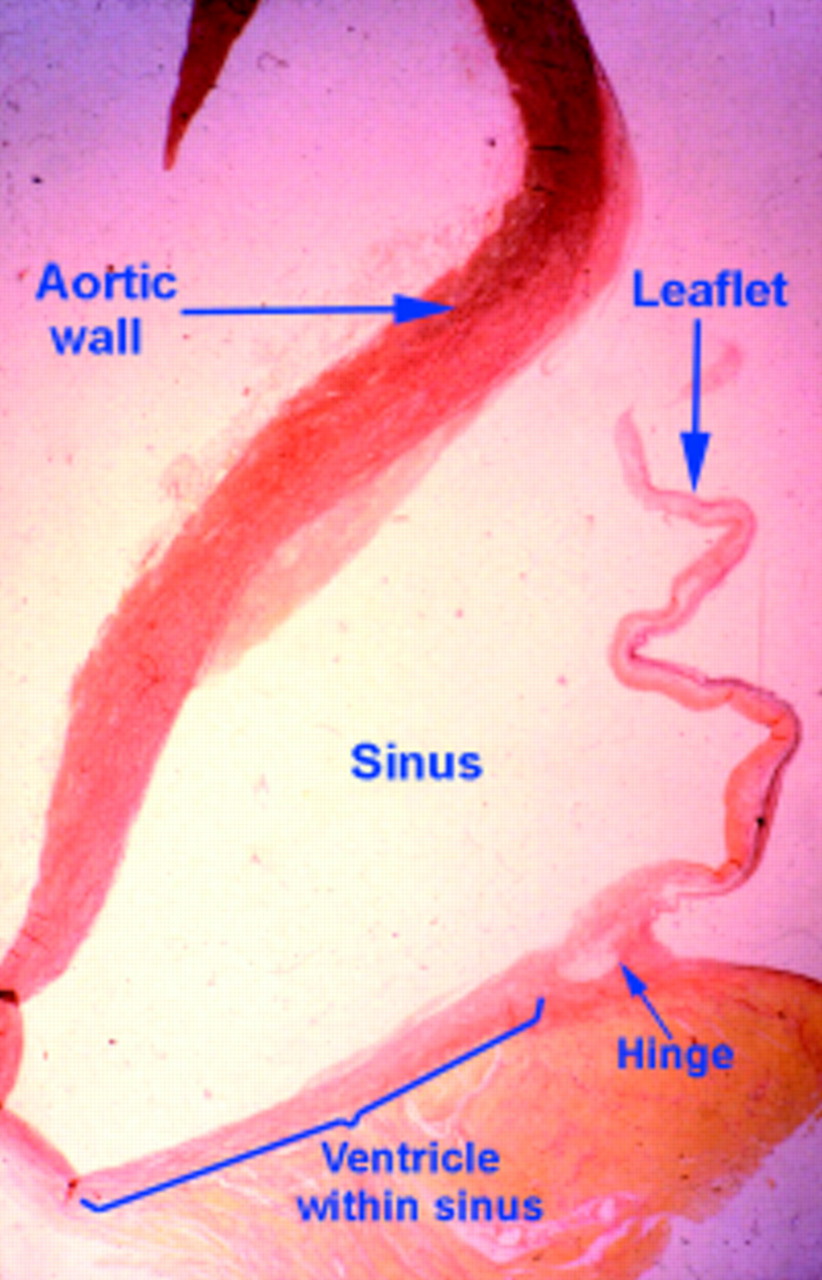
This section across one of the two coronary sinuses of the aortic valve shows how the hinge of the valvar leaflet is attached to the ventricular myocardium well proximal to the anatomic ventriculo-arterial junction (see fig 5 also).
Examination of the area of the root proximal to the attachment of the valvar leaflets also reveals unexpected findings. Because of the semilunar nature of the attachments, there are three triangular extensions of the left ventricular outflow tract which reach to the level of the sinutubular junction. These extensions, however, are bounded not by ventricular musculature, but by the thinned fibrous walls of the aorta between the expanded sinuses. Each of these triangular extensions places the most distal parts of the left ventricle in potential communication with the pericardial space or, in the case of the triangle between the two coronary aortic valvar sinuses, with the tissue plane between the back of the subpulmonary infundibulum and the front of the aorta (fig 4). The triangle between the left coronary and the non-coronary aortic valvar sinuses forms part of the aortic-mitral valvar curtain, with the apex of the triangle bounding the transverse pericardial sinus (fig 4). The triangle between the non-coronary and the right coronary aortic valvar sinuses incorporates within it the membranous part of the septum. This fibrous part of the septum is crossed on its right side by the hinge of the tricuspid valve, which divides the septum into atrioventricular and interventricular components. The apex of the triangle, however, continuous with the atrioventricular part of the septum, separates the left ventricular outflow tract from the right side of the transverse pericardial sinus, extending above the attachment of the supraventricular crest of the right ventricle.
When considered as a whole, therefore, the aortic root is divided by the semilunar attachment of the leaflets into supravalvar and subvalvar components.1 The supravalvar components, in essence, are the aortic sinuses, but they contain at their base structures of ventricular origin. The supporting subvalvar parts are primarily ventricular, but extend as three triangles to the level of the sinutubular junction. Stenosis at the level of the sinutubular junction is usually described as being “supravalvar”. In that the peripheral attachments of the leaflets are found at this level, the junction is also an integral part of the valvar mechanism.6 Indeed, stretching of the sinutubular junction is one of the cardinal causes of valvar incompetence.
Does the aortic valve have an annulus?
As with so many disputes, the answer to this ongoing conundrum resides in the definition of an “annulus”. In the strictest sense, an annulus is no more than a ring. In this respect, the entirety of the aortic root can be removed from the heart, and slipped on the finger in the form of a ring. Within the ring as thus removed, however, the leaflets themselves are not supported in ring-like, but rather in crown-like fashion. The answer regarding the presence or absence of an annulus, therefore, is very much in the eyes of the beholder. Some have argued that fibrous thickenings attach the leaflets within the root, and point to these supposed thickenings as the “annulus”.1 I find this confusing, since the purported thickenings are not universally present. Even when found, if removed they would constitute a crown-like circlet rather than a true ring. It is my own belief that the aortic root would be best understood if divorced from the concept of the “annulus”. This is unlikely to happen. Suffice it to say, therefore, that the “ring” takes the form of the cylindrical aortic root in which the valvar leaflets are supported in crown-like fashion (fig7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A diagrammatic representation of the aortic root shows its considerable length. The leaflets are attached within the cylinder of the root in the form of a coronet.
Clinical implications
There are several inferences from the complex interplay of ventricular and arterial structures which make up the aortic root which are important in the clinical context. When seen in long axis section, the diameter of the root varies greatly through its short length. The root is much wider at the midpoint of the sinuses than at either the sinutubular junction or at the basal attachment of the leaflets. This becomes of significance when considering measurements of the “annulus” since, as discussed, the hinges of the leaflets extend through all these three levels. Proper values can only be provided when measurements are made at the bottom of the valvar attachments, at the widest point of the sinuses, and at the sinutubular junction. Similarly, if measurements were taken from the basal attachment of one leaflet to the comparable point of an adjacent leaflet, as is frequently shown in diagrams, this would not measure the full diameter of the outflow tract, but rather a tangent across the root. These considerations are also important in a surgical context. The native valvar leaflets are obviously removed during the procedure of valvar replacement. The prostheses used for the purposes of replacement most usually have a truly circular sewing ring. Should the stitches used for securing this ring be placed within the semilunar remnants of the removed valvar leaflets, then there will be some distortion when the valve is “seated”, albeit that this does not usually compromise its subsequent function. When necropsied hearts are examined subsequent to valvar replacement, the circular sewing ring is usually found to be located at the anatomic ventriculo-arterial junction.2 It is the normal discrepancy between this junction and the haemodynamic junction which is the key to understanding the clinical anatomy of the aortic root.
Acknowledgments
I am indebted to Dr Siew Yen Ho for her help in the preparation of this review, and to Karen McCarthy and Vi Hue Tran for help in preparing the illustrations. The work itself was supported by the British Heart Foundation together with the Joseph Levy Foundation.