Article Text

Statistics from Altmetric.com
Most patients with infective endocarditis respond to appropriate antibiotic treatment within 72 hours, with a definitive loss of fever and improvement in general well being. Patients who show such prompt improvement will usually do well, but those who remain febrile and septic despite optimal antibiotics usually need surgery.1Late recurrence of fever is frequently the result of antibiotic sensitivity or an infected central line, and is less often caused by the development of bacterial resistance, infection by multiple organisms or a second infection by fungus or staphylococcus. Lack of success in treating endocarditis frequently comes from failure to observe recognised guidelines,2 ,3 and from lack of a team approach involving both the clinical microbiologist and the cardiac surgeon from an early stage.
Persistent or recurrent fever
Microbiological issues
From the outset the clinical microbiologist needs to be involved closely. The treatment regimen needs to be matched to both the clinical and microbiological circumstances. When there is a continuing clinical problem, despite appropriate initial treatment, then the microbiologist must be consulted again.
Infection elsewhere
The possibility of infection occurring elsewhere—intracardiac or extracardiac—must be the first thought of the clinician faced with this situation.
Line infection
A common cause of recurrence of fever is the central line. This should be removed and the tip sent for culture. Often the culture is sterile but the fever resolves rapidly after removal of the line. Recolonisation of the infected valve by staphylococcus or fungus derived from the line is rare but can occur. It is usually caused by poor sterile technique and line care. Such additional infection is a serious problem. It needs appropriate antibiotic treatment and frequently requires urgent surgery.
Paravalvar/intracardiac abscess
The patient not doing well despite being infected by an antibiotic sensitive organism probably has a paravalvar abscess until proved otherwise. This must be sought vigorously and usually requires surgery to effect a cure.4 Most patients with paravalvar abscesses also have severe valvar regurgitation and heart failure with evidence of uncontrolled infection.5 Therefore there is usually little or no difficulty in arriving at the decision to advise urgent surgery both to remove the infected tissue and to replace the leaking valve.
If there is a proven abscess plus evidence of persistent sepsis but without severe valvar regurgitation, the clinician is often slow to recommend surgery because he or she believes that the antibiotics will eventually produce a cure. This is nearly always a mistaken belief and surgery should be carried out sooner rather than later. Occasionally abscesses will discharge into the heart leaving a cavity with a wide entrance that the antibiotics can sterilise, but this is rare. It is not an event which should be anticipated thereby delaying the needed surgical cure.
In a small percentage of patients the infection appears to be under control and there is no haemodynamic requirement for surgery, but abscess is detected on echocardiography (usually transoesophageal echocardiography (TOE)) (fig 1). On cessation of the antibiotics the infection nearly always returns unless the very rare occurrence of internal discharge of the abscess has occurred. In this respect some abscesses appear to be functionally inaccessible to circulating antibiotics, and in such circumstances patients will usually need to undergo surgery.6
Fatal outcome in endocarditis
Late diagnosis
Inadequate treatment
Failure to seek advice

Aortic (Ao) root abscess (arrowed) shown in short axis of transoesophageal study. Figure reproduced courtesy of Dr Petros Nihoyannopoulos.
Coxiella produces an indolent illness but often with extensive local abscess formation.7 Diagnosis depends on a high index of suspicion in patients in whom no infecting organism has been found immediately. Such patients should routinely have serology for Q fever even if there is no known contact with animals. These patients often have only intermittent fever. Constitutional symptoms also are sometimes intermittent and clinical examination can be unrevealing in the early stages. Later on hepatosplenomegaly may dominate the clinical scene, deflecting attention away from the heart.8
Although echocardiography via the transoesophageal route, particularly with a multiplane transducer, has greatly improved the detection of abscesses, not all are visible. Most abscesses are para-aortic. In a French study nearly 90% of aortic abscesses subsequently confirmed at surgery had been seen by transoesophageal study compared with less than 50% via the transthoracic route.5 They may be missed if they are in the aortic wall. Mitral ring abscesses were less common, were only rarely detected by the transthoracic route, and more than half had still been missed by TOE in this study.5 Echocardiography can only detect abscesses which show a difference in acoustic properties compared to the surrounding tissue or when there is Doppler evidence of flow through a defect or communication caused by the abscess. If no such difference or abnormal flow exists, echocardiography will miss the diagnosis—no technique is 100% sensitive. If the clinical picture points to an abscess but none is detected this is an unusual but a good reason to repeat the TOE in a few days.
Extracardiac
Metastatic infection or mycotic aneurysm may cause fever. Any remote pain or focal symptoms should raise suspicion. Headache, particularly if lateralised, may suggest cerebral abscess or a mycotic aneurysm of a cerebral vessel. Mycotic aneurysms can present during the course of treatment or even after a satisfactory microbiological cure has been achieved and the antibiotic treatment has been completed. Adjacent aseptic meningitis is common. Focal signs in the nervous system may be absent but a computed tomographic scan of the brain may bring surprises. Abscesses in the frontal lobes may cause no more than a change in personality or there may be multiple infarcts in relatively silent areas.
Acute low back pain may be caused by spinal abscess formation and vertebral osteomyelitis or discitis should be suspected, particularly when there is evidence of a radiculopathy.9
Antibiotic problems
The development of drug sensitivity may lead to recurrence of fever with or without a rash but usually with a blood eosinophilia and a rise in C reactive protein in a patient who had been previously doing well. The patient is often not clinically ill or septic, but occasionally such patients feel and look very unwell. This is usually a reaction to a penicillin, most often in the third week of treatment. Sometimes, it may be appropriate to stop antibiotic treatment or it may be considered wise to continue with a different combination chosen on the advice of the bacteriologist.
Wrong diagnosis or more than one diagnosis
It is possible that the patient being treated for infective endocarditis and not doing well may have been given a wrong or incomplete diagnosis. The patient may have been regarded as having culture negative infective endocarditis or the positive cultures may have been misleading or not have grown a typical organism. If vegetations are seen, they may not be caused by infective endocarditis and in reality may be sterile thrombotic vegetations in a patient with adenocarcinoma or systemic lupus. The fever and rise in acute phase reactants may be caused by lymphoma, tuberculosis, opportunistic infection in AIDS or active autoimmune disease or, rarely, the patient may have a fever producing portal of entry such as ulcerative colitis, or carcinoma or Hodgkin's disease in addition to infective endocarditis.
Surgical goals
Restoration of haemodynamic competence
Removal of all infected tissue
It is obvious that whereas patients with any of these conditions are not harmed by administration of unnecessary antibiotics, steroid treatment of a patient with infective endocarditis on a false diagnosis of polyarteritis may be lethal.
Major immune activation
Immune activation, particularly with progressive renal failure, may be another cause for a patient failing to improve despite antibiotic treatment. In these patients blood cultures may have been negative (even if there has been no previous antibiotic treatment) and negative serology and microbiology will have excluded infection by cell dependent organisms. There may be doubt about the diagnosis but flamboyant vegetations are usually seen on echocardiography and the patient may have had emboli. Changing the antibiotics fails to help. In these rare patients deterioration will continue until removal and replacement of the valve. No organisms may be grown from it or stain microscopically, but the rapid improvement that follows surgical intervention clearly shows that the bacterial antigen had persisted in the valve. There is a danger of such patients being falsely diagnosed as having Libmann-Sacks (in association with systemic lupus erythematosus) or marantic endocarditis but, unlike such patients, they have an erosive destructive endocarditis with positive rheumatoid factor but no lupus specific antibodies. Renal biopsy shows a focal crescentic glomerulitis and a “lumpy bumpy” deposit of polyclonal immunoglobulins on the basement membrane shown on immunofluorescence microscopy.10 ,11
Multiple organisms
Infection by multiple organisms is unusual and is most often seen in intravenous drug abusers. Again the advice of the microbiologist on appropriate treatment should be sought and consideration given to surgery.
Acute myocardial and valvar problems, disappearing murmur or insignificant murmurs
Myocardial problems
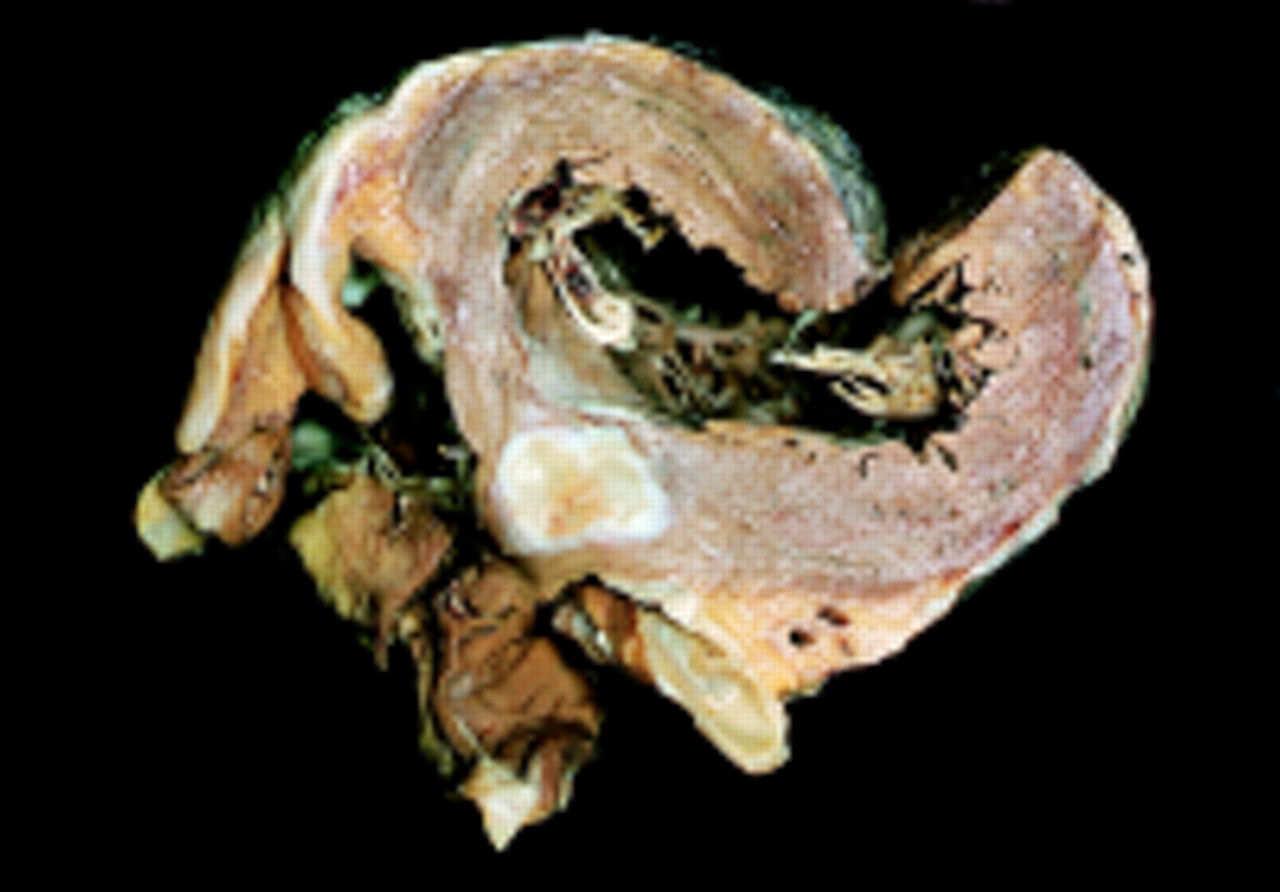
These are important although not very common. The patient may be unwell because of a low cardiac output which may be caused by coronary embolism with myocardial infarction or intramyocardial abscess formation (fig 2). Infectious myocardial infiltration or toxic myocardial depression may also be responsible, but this is rare.

Myocardial abscess. These are usually inoperable.
Valvar problems
A low cardiac output leading to cardiogenic shock and/or pulmonary oedema more commonly results from a sudden increase in mitral or aortic regurgitation. Chordal rupture and a flail, or perforated mitral valve or perforation/prolapse of an aortic cusp, may lead to free regurgitation. In both situations the very severe regurgitation alters the haemodynamics in such a way that the physical signs of the valve lesion and particularly the murmur may become insignificant and the clinical picture is dominated by the low cardiac output and a loud gallop rhythm.
Mitral valve
Reduction in gradient between a low left ventricular systolic pressure and a high left atrial systolic V wave in severe mitral regurgitation results in a softer or even disappearing murmur and a plummeting forward stroke output.
Aortic valve
Tachycardia and rapid diastolic equilibration of central aortic and left ventricular diastolic pressures in acute aortic regurgitation may obliterate the murmur and, by closing the mitral valve prematurely (an important sign on the M mode echocardiogram), severely limit forward flow.
In both situations urgent transthoracic echocardiography and Doppler usually confirm the cause of the clinical problem; if there is any doubt TOE should be done without delay. Such patients need immediate surgery, and cardiac catheterisation before surgery usually causes dangerous delay and a fluid load when time is of the essence.6 ,12-14
Role of surgery in the problem patient
When a patient is not doing well the possible benefits that might come from surgery should be considered. The goals of surgery are to remove all infected tissue and to restore haemodynamic competence. In the majority of patients who are not doing well while being treated for infective endocarditis, the problem is either uncontrolled infection, a haemodynamic problem, or a combination of both; surgery is therefore frequently essential. This is the most compelling reason for involving a surgeon at an early stage in the management of most patients with infective endocarditis. Surgeons are far happier to act quickly and appropriately when needed if they already know the patient or are at least familiar with the details through discussion.
The benefits of surgery are often enormous and usually almost immediate. It reverses a deteriorating haemodynamic situation, which uncorrected will often lead to death, and has the added advantage of removing infection which was “hidden” from the antibiotics—for example, in an abscess. Removal of infected tissue also leads to a rapid overall constitutional improvement as the infected burden is drastically reduced.
Indications for surgery
Haemodynamic
acute aortic or mitral regurgitation
Staphylococcal infection
often urgently
Infective endocarditis which is difficult to cure medically
fungus: always
coxiella: usually
chlamydia: usually
Staphylococcus epidermidis
Persistent fever
abscess: paravalvar or extracardiac
Major immune activation
persistent fever despite appropriate antibiotics
Emboli
remove very large vegetations (early or not at all )
Staphylococcal infection
Staphylococcal endocarditis may cause rapid tissue destruction and embolism, although vegetations may be difficult or impossible to detect. Surgical treatment is needed at once in patients who are toxic despite adequate antibiotics or who have evidence of abscess formation either on echocardiography or deduced from ECG conduction system delay (prolonged PR interval). Failure to act quickly in this situation often leads to a fatal outcome. Emergency surgery in these situations is the only treatment which provides any chance of averting a fatal outcome and preventing spread of infection despite full antibiotic treatment.
Nosocomial staphylococcal endocarditis (caused by coagulase negative staphylococci originating from the patient) carries a particularly high mortality because it is often not suspected in patients being treated for other diseases (particularly renal failure) and who are not known to have valve disease. It is diagnosed late and tends not to be operated on because of co-morbidity. The portal of entry is usually an indwelling intravenous line.15
Fungi and other organisms
Infection by certain organisms usually requires surgical excision because although they are technically sensitive to antimicrobial agents (albeit often very toxic in the case of fungi), they rarely if ever are cured without surgery. This always applies to fungus infection (fig 3), which usually occurs following antibiotic treatment or parenteral feeding in a patient who has had major abdominal surgery; alternatively the fungal infection may have gained entry at or just after cardiac surgery, especially in patients with wound infections or mediastinitis.

{kind=link}
{kind=link}
{kind=link}
Huge pedunculated vegetation (V) on the aortic valve caused by secondary candida infection in a young women with a variable course after treatment for enterococcal infection on a floppy mitral valve. Transoesophageal view—LA, left atrium; Ao, aorta. Figure reproduced courtesy of Dr Petros Nihoyannopoulos.
Similarly in patients with infective endocarditis caused by coxiella (Q fever) or chlamydia, the infection may appear to respond to antibiotics only to recur when they are stopped; in general, the patient needs either surgical excision of the infection or lifelong antibiotics, or sometimes both.14
Prevention of embolism
Surgery to prevent embolism is a contentious area. The patient may have had previous emboli or have large vegetations when first examined. Since the risk of embolism diminishes rapidly after the onset of antibiotic treatment, the decision for surgery to prevent embolism or further embolism in a patient with large vegetations when first seen should be made immediately and the surgery carried out urgently or not at all.16 Vegetations over 10 mm in diameter are associated with an increased risk of embolism but this risk has never been quantified accurately, nor has it been proved to be higher than risk posed by an operation to remove the vegetation. Often the decision is made easier because the large vegetation is associated with a degree of valve regurgitation that merits surgery in its own right, and the vegetation is removed with the valve. Vegetations, which are viewed anxiously day after day, will probably not become emboli.
In the past it was taught that anticoagulant treatment was contraindicated in infective endocarditis. However, since it will not influence the risk or result of rupture of a mycotic aneurysm the usual indications for anticoagulant treatment apply. Control of the international normalised ratio (INR) needs to be meticulous and is often difficult because of the interplay of other factors such as changes in diet, the influence of antibiotics on the INR, and pro-coagulant states induced by the infection. Patients who are sufficiently ill to be in bed should receive prophylactic heparin, but most patients should be encouraged to be up and about. There is some evidence that low dose aspirin may reduce the size of vegetations and lower the risk of embolism.17
Antibiotic treatment and surgery
The management of antibiotic treatment in the immediate preoperative period and following surgery needs careful planning. In general it is a serious mistake to delay urgently needed surgery in an attempt to give more antibiotics before surgery. This issue will be addressed in a separate article.
Results of surgery
Comparisons between the results of medical and surgical treatment have been made in many publications but are flawed from the scientific point of view mainly because of case selection. No randomised prospective trials of medical versus surgical treatment have ever been done or are ever likely to be done because they could include only patients suitable for medical treatment alone and thus would be neither ethical nor informative.
In certain circumstances, surgery may not be an option. For example, fig 2 shows an abscess in the wall of the left ventricle remote from an infected aortic valve. Sometimes detected by echocardiography, such abscesses are fortunately rare because they usually present the surgeon with an impossible task.
Because of the lack of an evidence base, decision making regarding surgery in infective endocarditis must be based on common sense and clinical experience. On this basis aggressive early surgery appears to reduce the mortality of this disease greatly. The threshold for surgical intervention is still too high in many centres, but despite this surgery must be reserved for patients with a definite indication.11 ,12 ,15 ,17 Early surgery is rarely regretted and very close observation with frequent clinical examination, and ECGs and echocardiograms repeated from time to time, will allow the timing to be decided appropriately. Undue delay is fraught with hazard, increasing the technical difficulties for the surgeon, extending the length of time spent in hospital, reducing the patient's chance of an uncomplicated recovery, and increasing future morbidity and the need for further surgery. It is of particular importance not to delay surgery in order to give more preoperative antibiotics in a patient with a strong indication for surgery
Failure to respond: summary
Abscess formation
paravalvar
metastatic
Low cardiac output
flail mitral valve or perforation
free aortic regurgitation
toxic myocardial depression or infectious infiltration
coronary embolism
Wrong diagnosis
lymphoma
sarcoidosis
autoimmune disease—for example, systemic lupus erythematosus
AIDS
tuberculosis
Major immune activation
progressive renal failure
vasculitis
emboli