Article Text

Statistics from Altmetric.com
Valve surgery remains the treatment of choice for most significant valve lesions. Symptomatic improvement has been well demonstrated in a number of studies and is usually sustained into the late postoperative period, especially when valve replacement is undertaken for stenotic lesions. Invasive studies have shown that symptomatic relief is consistently accompanied by haemodynamic improvement, and the overall superiority of surgical intervention over conservative medical treatment for most patients with advanced valve disease has been firmly established.
Late results after valve surgery
The analysis of survival rates of patients following valve replacement relative to age and sex matched populations have shown an impaired prognosis in all but a minority.1 In patients older than 65 years undergoing aortic valve replacement for aortic stenosis, relative survival is “normalised” after the first postoperative year, but in all other indications an excess late mortality has been observed in surgical patients. Long term follow up studies consistently report better survival rates in patients undergoing aortic rather than mitral valve replacement, with 10 year actuarial survival rates of approximately 65% for aortic valve replacement, 55% for mitral valve replacement, and 55% for double (aortic and mitral) valve replacement. Late mortality is greater when surgery is undertaken for regurgitant as opposed to stenotic lesions, while long term survival is better in the context of degenerative as opposed to ischaemic or rheumatic valve pathologies. These observations illustrate the fact that long term mortality following valve replacement is most reflective of the nature of the original disease process, the pre- and postoperative state of the myocardium and coronary circulation, as well as the general wellbeing of the patient with valve related deaths being relatively infrequent. Approximately 60% of late mortality is attributable to cardiac causes that are independent of the valve surgery (namely, cardiac failure, myocardial infarction, arrhythmia or sudden death), approximately 20% is caused by valve related complications, and 20% is from non-cardiac causes. Independent predictors for death in the late postoperative period include advanced age (> 65 years), left ventricular impairment, New York Heart Association functional class IV symptoms at the time of surgery, coincident coronary artery disease, and documented ventricular arrhythmias.2 The presence or absence of these negative factors at the time of aortic valve replacement, for example, gives rise to a predicted 10 year survival rate varying between 16–90%.3 In the presence of three vessel or left main stem coronary artery disease nine year survival is as low as 29%4 and the negative influence of coronary disease is not completely ameliorated by grafting at the time of initial surgery. Favourable and rather similar survival rates have been reported with a variety of mechanical and bioprostheses. While the specific selection of a mechanical or bioprosthesis is usually dependent on factors such as age, valve position, risk of anticoagulation, and patient preference, the presence or absence of these negative predictors of clinical outcome should also be considered in order to minimise valve related complications and maximise quality of life within the life span expected. While attention to the medical treatment of additional cardiac comorbidities is important, improvements in long term survival after valve surgery will most likely be achieved through the earlier recognition and correction of significant valve lesions.
Late complications after valve surgery
Left ventricular failure
Following the successful surgical correction of left sided valve defects, residual left ventricular impairment may be present in some patients, exposing them to the risks of progressive cardiac failure and sudden death. Left ventricular dysfunction is usually the consequence of longstanding pathological changes that are secondary to sustained preoperative pressure and/or volume overload, but may also be related to the influence of other cardiac diseases including coronary artery disease, poorly controlled hypertension, and coincident cardiomyopathy.
The pathophysiology of late left ventricular dysfunction is greatly dependent on the preoperative left ventricular load, and therefore the specific valve lesion corrected. When aortic valve replacement is undertaken for aortic stenosis, postoperative improvement in systolic and diastolic left ventricular function may occur over a period of years but is by no means inevitable. In aortic stenosis, severe left ventricular systolic dysfunction may be caused by “afterload mismatch” with an increase in left ventricular systolic pressure and wall stress leading to a reduction in stroke volume and ejection fraction. Under these circumstances, systolic function improves once left ventricular pressure is normalised. Alternatively, systolic dysfunction may be caused by reduced contractility as a result of hypertrophy and fibrosis or by the additional insult of scarring following myocardial infarction. When this is the case, postoperative improvement in left ventricular systolic function often does not occur and long term clinical outcome may be severely compromised. Factors associated with residual postoperative left ventricular systolic impairment following the correction of aortic stenosis include low preoperative ejection fraction and aortic valve gradient, presence of coronary artery disease, and previous myocardial infarction. The combination of severe preoperative left ventricular dysfunction and previous myocardial infarction is particularly ominous, with a high operative risk and only 30% of patients alive two years after surgery.
Improvement in left ventricular diastolic function following aortic valve replacement for aortic stenosis is equally important in determining clinical outcome and is critically dependent on regression of left ventricular hypertrophy.5 While this occurs predictably in most patients over a period of years6 it rarely does so to normal ventricular mass; it may also be impaired by the presence of irreversible myocardial disease, and if only partial may be accompanied by persistent diastolic dysfunction and associated with excess mortality.
The long term results of surgery to correct mitral and aortic regurgitation are not as good as when aortic stenosis is the dominant lesion. The main reason for this is the more commonly encountered problem of postoperative left ventricular dysfunction and the impact that this has on clinical outcome. Impaired left ventricular function following successful correction of valvar regurgitation is thought to be attributable to a variable degree of irreversible damage to the dilating left ventricle, which is often subtle and difficult to identify preoperatively. Symptoms are delayed in chronic aortic and mitral regurgitation so that surgery is often offered too late. Once present, symptoms may indicate the presence of an irremediable degree of left ventricular dysfunction and are associated with an unfavourable long term prognosis. In mitral regurgitation, a deterioration in postoperative left ventricular function is to be expected anyway, with the presence of a competent valve leading to an increase in afterload and decrease in preload; thus in the presence of already depressed contractile function, left ventricular failure is likely to hinder long term recovery. In order to minimise the degree of postoperative left ventricular impairment following surgery for mitral and aortic regurgitation, surgery should be considered at an early stage and often before symptoms develop. Careful surveillance of left ventricular function in asymptomatic patients is essential. A reduced ejection fraction is predictive of a postoperative left ventricular impairment and in itself is an indication for early surgical intervention.7 In mitral regurgitation, measurement of left ventricular end systolic volume is useful, being independent of preload, correlating well with measurements of myocardial contractility, and when elevated (> 50 ml/m2) being predictive of postoperative left ventricular impairment.8In aortic regurgitation, subtle degrees of left ventricular dysfunction may only be apparent during haemodynamic stress, but once discovered may serve as an indication for surgical intervention.
When surgery is undertaken, surgical technique is an important factor in determining postoperative left ventricular function and therefore early and late clinical outcome. For pure mitral regurgitation, the benefits of mitral repair and reconstruction as opposed to replacement are well established.9 There is a lower rate of perioperative mortality and improved long term survival. Left ventricular function is better preserved, thromboembolic complications and the risk of future infective endocarditis are reduced, while the need for long term anticoagulation is obviated in most patients. These advantages in anatomically suitable patients and with appropriate surgical expertise are achieved at lower cost both in the short and long term10 such that the weight of medical and economic evidence in favour of valve repair is compelling. When patients with mitral regurgitation are unsuitable for valve repair and replacement is undertaken, evidence suggests that overall left ventricular function may be best preserved through the retention of the subvalvar apparatus.
Right ventricular failure and tricuspid regurgitation
The late appearance of tricuspid regurgitation accompanied by symptoms and signs of right heart failure is an important cause of late morbidity and mortality in patients undergoing mitral and aortic valve surgery. Recent studies have shown that significant tricuspid regurgitation is detectable by echocardiography in up to two thirds of patients late after mitral valve replacement, and that it is clinically apparent in more than one third.11 These patients have a pronounced reduction in exercise capacity and a poor functional outcome attributable to an impaired cardiac output response to exercise.12 The pathophysiology of this interesting clinical syndrome is variable and complex. In patients with rheumatic valve disease, the development of progressive organic tricuspid valve pathology may occur and accounts for about 25% of patients presenting with late tricuspid regurgitation. The persistence or late development of left heart pathology and the presence of unresolved pulmonary hypertension (see below) are important causes of increased afterload on the right ventricle which predisposes to progressive right ventricular dilatation. In many patients, however, persistent right ventricular and tricuspid annular dilatation may be present despite a postoperative reduction in pulmonary artery pressure. In some, this may reflect longstanding preoperative pressure overload since it is often apparent in those in whom mitral surgery was delayed for many years, while in others, right ventricular impairment may be caused by perioperative ischaemia. In many patients, however, the presence of uncorrected tricuspid regurgitation at the time of initial surgery is likely to be important since this may lead to a vicious cycle developing over subsequent years comprising right ventricular enlargement, further annular dilatation, and gradual worsening of tricuspid regurgitation and right ventricular function.
A number of studies have shown that correcting the mitral lesion without intervening on the tricuspid valve is associated in many patients with persistence and often worsening in the severity of tricuspid regurgitation postoperatively. Since reoperation to correct severe tricuspid regurgitation at a later stage is associated with a high mortality,13 an emphasis should be placed on prevention rather than cure. In this regard, a strategy of earlier surgical intervention combined with the accurate detection and liberal correction of tricuspid regurgitation at the time of the initial operation seems prudent. Pre- and intraoperative echocardiography allows for the assessment of the severity of tricuspid regurgitation and its relation to abnormalities of right ventricular and tricuspid annular function before and after correction of the left heart lesion. Tricuspid annuloplasty should be contemplated when tricuspid regurgitation is moderate or severe and accompanied by tricuspid annular dilatation (> 21 mm/m2) since spontaneous regression of tricuspid regurgitation postoperatively is rare under these circumstances.
Pulmonary hypertension
Pulmonary hypertension is commonly present in patients with left sided valve disease and is usually most pronounced in those with longstanding rheumatic mitral valve involvement. Pulmonary hypertension reflects not only passive transmitted back pressure from left atrial hypertension but also an active increase in pulmonary vascular resistance caused by a combination of pulmonary vasoconstriction and obliterative changes in the pulmonary vascular bed. Following the correction of left sided valve defects, an early fall in pulmonary artery pressure is expected and reflects normalisation of left atrial pressure as well as vasomotor changes including relief of vasoconstriction. The most dramatic haemodynamic changes in the pulmonary circulation therefore occur within the first few days after surgery and certainly within the first six months. Thereafter, any further fall in pulmonary vascular resistance is unpredictable and dependent upon structural changes within the hypertrophied pulmonary arteries, arterioles, and veins, a process which is slow, variable, and often incomplete. While a dramatic early reduction in pulmonary pressure is expected in most patients with even extreme pulmonary hypertension undergoing mitral or aortic valve surgery, full normalisation is rarely if ever achieved. Even when pulmonary pressures are apparently normal at rest, a hypertensive pulmonary response to exercise is often seen, with a rapid rise in pulmonary artery pressure at relatively low workload.14 This irreversible component of increased pulmonary vascular resistance probably reflects residual morphological changes within the pulmonary vasculature and leads to a continued and chronic increase in afterload on the right heart. The more complete the correction of the left sided lesion the more likely it is that pulmonary vascular resistance will fall, while conversely the late emergence of pulmonary hypertension and right heart failure may sometimes reflect left sided prosthetic dysfunction or new left heart pathology. While a temporary reduction in pulmonary pressures has been described with the use of nitrates or inhaled nitric oxide in the early postoperative period following mitral valve replacement, no specific treatment is available for persistent pulmonary hypertension; however, earlier diagnosis and surgical intervention may prevent the development of irreversible structural changes in the pulmonary circulation.
Sudden death, arrhythmias, and conduction abnormalities
Overall rates of sudden death in patients with prosthetic valves vary considerably and generally range from 15–30% with an estimated annual risk of 0.2–0.9%. Sudden death is defined as death within one hour of an event of abrupt onset and accounts for approximately 25% of all late deaths following valve replacement. Broadly speaking, sudden deaths may be stratified into three categories: those caused by natural disease processes, those relating to the prosthesis itself, and those resulting from management failure. Necropsy studies15 have shown that the majority of sudden deaths fall into the first category with the most common cause being ventricular arrhythmias, which are seen more often after aortic than mitral valve replacement and are sometimes a manifestation of coincident underlying ischaemic heart disease. Although the rate of sudden death decreases after aortic valve replacement, it is still a common cause of death with an incidence of 10–40%. Relating to this, the incidence of ventricular arrhythmia remains relatively high especially in those with cardiomegaly, residual cardiac hypertrophy, and left ventricular impairment. Causes of valve related sudden death include valve thrombosis, thromboembolism, endocarditis, paravalvar leak, and mechanical failure (see below), while sudden deaths relating to management failure include those caused by intracerebral haemorrhage occurring as a complication of anticoagulation treatment.
Because of the close anatomical relation between the aortic valve and conducting tissue, conduction defects are commonly found in association with aortic valve disease and are frequently encountered in the early postoperative period following aortic valve replacement. In those who develop complete atrioventricular (AV) block immediately after aortic valve replacement and who require pacing for more than six hours, permanent pacemaker implantation is usually required before discharge, while even when spontaneous recovery of AV conduction occurs, pacemaker implantation is required at a later date in 50% of cases. Patients with no change in the perioperative ECG after aortic valve replacement are also at risk, with an incidence of almost 14% of progressive conducting tissue disease emerging over the first six postoperative years.16 Although late pacemaker implantation rates are relatively low, this natural progression in conducting tissue disease combined with the known association between sudden death and the development of left bundle branch block (LBBB) after aortic valve replacement means that careful outpatient surveillance is critical and a low threshold for permanent pacemaker implantation should be set, especially in patients with a history of syncope or presyncope.
Thrombosis, thromboembolism, and complications from anticoagulation
Thrombotic and haemorrhagic complications are a major cause of morbidity and mortality and therefore are important determinants of long term outcome following valve surgery. Thrombosis on prosthetic valves (fig 1) can give rise to local mechanical problems including valve obstruction, but can also lead to thromboembolism and peripheral ischaemic complications including stroke. Overall, the risk of bleeding is greater than that of thromboembolism.17 For every 100 patient-years, the risk of valve thrombosis is reported to be 1 to 3, of thromboembolism 0.71, and of bleeding 2.68. Mortality is greater with haemorrhagic than with thromboembolic complications, being 0.3 versus 0.03 per 100 patient-years, reflecting the likelihood of death associated with intracranial bleeding. The development of these complications, however, cannot always be attributed to previous valve surgery and it is easy to forget that there is a background risk of stroke, transient cerebral ischaemia, and intracranial bleed that rises with age to approximately 2% per year by the age of 75 years.

Transoesophageal echocardiographic image showing multiple mobile thrombi (arrows) on the left atrial (LA) aspect of a prosthetic mitral valve (MV) in a patient who presented with transient cerebral ischaemia.
Numerous factors may influence the rate of valve thrombosis and thromboembolism, many of which are not specifically related to the surgical intervention. For valve thrombosis, the most important risk factors are periods of under-anticoagulation, low cardiac output, and the presence of hypercoagulable states including pregnancy.18 The lowest thrombosis rates have been reported with unstented homografts and pericardial heterografts in the aortic position. Comparison between mechanical prostheses is difficult since a fair assessment would have to assume equivalent levels of anticoagulation during the time of surveillance. The large variation in valve thrombosis rates reported for mechanical prostheses in the literature is at least partly caused by the fact that anticoagulation levels have varied substantially in published studies. Patients are at particular risk of valve thrombosis when anticoagulation is interrupted, even temporarily, during non-cardiac surgery at a time when the thrombotic substrate is often increased as a result of systemic illness. For thromboembolism, the constellation of risk factors is more numerous and their interactions more complex, but the quality of anticoagulation control and cardiac rhythm are by far the most important.19 Increasing age (> 50 years), ethnicity, associated hypertension, diabetes, and cigarette smoking are important, while the presence of chronic disease and intercurrent illness, especially infection, intermittently and substantially increases thromboembolic risk. During the advancement of chronic valve disease, many of the adaptive changes to pressure and volume overload will expose patients to chronic and irreversible changes in cardiac anatomy and physiology despite corrective surgery. Thus, atrial and ventricular dilatation, impaired ventricular function, chronic atrial fibrillation, atrial thrombus, and previous systemic embolisation increase the risk of thromboembolism. Valve type and position are also important. The incidence of events with ball and cage, tilting disc, and bileaflet valves is estimated at 2.5, 0.7, and 0.5 per 100 patient-years, respectively, with valves in the mitral position or more than one valve replacement being associated with double the risk of aortic valves.
Increased risk of bleeding is associated with age (> 70 years), erratic anticoagulation control, and recent initiation of warfarin. The latter is probably related both to fluctuations that often occur in the early stages of anticoagulation but also to the ability of this form of treatment to unmask underlying pathology. Even though clinical events do occur during periods of apparently excellent anticoagulation control, bleeding complications can be minimised through a combination of patient education and careful monitoring of anticoagulation with appropriate dose adjustment. Studies in anticoagulation clinics have shown that only approximately 50% of patients will be within their target range at any given moment of time so that improvements can be made by aiming to achieve narrower and more specific target INRs (international normalised ratios) with a greater proportion of time spent “in range”.
Research continues to improve surgical technique and to reduce the thrombogenicity of replacement heart valves, but the risk of thrombosis, thromboembolism, and bleeding will never be abolished. Improved patient safety will be achieved by the careful selection of the most appropriate and least thrombogenic replacement valve in each patient, through the careful achievement of tight anticoagulation control, and through the close surveillance of patients in the outpatient clinic looking for symptoms and signs of impending valve thrombosis and degeneration, especially during systemic illness or at the time of non-cardiac surgery.
A previous article in this series provides a detailed review of the role of anticoagulation in valvar heart disease.20
Infective endocarditis
Infective endocarditis is a dreaded late complication following valve surgery, with infection usually located on the replacement device (prosthetic valve endocarditis; PVE) but sometimes developing on other diseased valves. PVE is traditionally classified as either “early”, when it develops within 60 days of initial surgery, or “late” when it presents at a later stage. Early PVE is caused by contamination of the valve during or immediately after implantation, with the culprit organisms therefore reflecting those likely to be acquired in a hospital setting, including resistant strains ofStaphylococcal epidermidis, Gram-negative bacilli, and fungi. The likelihood of early PVE is less with porcine than with mechanical valves and is least with homografts.21 Late PVE results from the infection of a previously sterile implant so that the spectrum of bacteria and their portal of entry is more analogous to that of native valve endocarditis, with the streptococci most common. There are conflicting reports regarding the relative likelihood of late PVE with bioprostheses and mechanical prostheses, but the lower risk of PVE seen in the early postoperative period with homografts seems to be largely nullified at later time points.
PVE is a grave condition, being associated with a reported mortality of 25–60% which is highest for early infections when the degree of valve destruction tends to be greatest. With mechanical prostheses, the infection tends to colonise the sewing ring of the valve while in bioprostheses the infection can, in addition, involve the valve cusps. Vegetations may develop around the valve and give rise to systemic embolisation, while local periannular tissue destruction may lead to paravalvar leak, abscess, and fistula formation (fig 2). Clinical presentation is similar to that of native infective endocarditis but there should be a higher level of suspicion in patients with prosthetic valves in whom the presence of fever or a new or changing murmur should be regarded as PVE until proven otherwise. Diagnostic criteria are also similar but transoesophageal echocardiography is of particular importance in PVE, with a diagnostic sensitivity rate of up to 95% as compared with up to 65% for transthoracic echocardiography, reflecting the superior clarity and breadth of unimpeded visualisation of both the prosthetic valve and the perivalvar complications.

Transoesophageal echocardiographic image showing systolic (right panel) and diastolic (left panel) frames of a peri-aortic cavity (arrow) in a patient with infective endocarditis on a prosthetic aortic valve. The systolic expansion of the cavity is caused by its communication with the left ventricular outflow tract.
Prompt treatment with broad spectrum antibiotics is critical once the diagnosis is suspected. It is advisable to begin treatment before culture results are available because the incidence of systemic embolisation diminishes rapidly once effective treatment is commenced.22 Treatment strategies for PVE usually combine prolonged appropriate antibiotic treatment (at least six weeks after reoperation) with timely surgical intervention. Medical treatment alone may occasionally be successful—for example, when late PVE develops because of infection with a highly sensitive streptococcus or when there is localised colonisation of the leaflets of a bioprosthesis—but reoperation is usually required. Indications for surgery include prosthetic valve dysfunction, abscess or fistula formation, systemic embolisation, persistent bacteraemia despite appropriate antibiotic treatment, cardiac failure, and progressive multiorgan dysfunction. Operative mortality rates are high (up to 50%) but improving with the primary aim being to excise and remove all infected tissue before replacing the culprit valve.
For detailed reviews of endocarditis in valvar heart disease see earlier articles in this series.23 24
Mechanical complications
Paravalvar leak may occur with both mechanical and biological valves and, in the absence of infection, usually reflects a technical problem relating to suture failure. Subclinical levels of haemolysis can be biochemically detectable with all types of mechanical prosthesis, but clinically significant levels of haemolysis are rarely found in the absence of paravalvar leak.
In mechanical valves, sudden failure of the components of the valve is exceedingly rare but usually fatal. More common is a gradual deterioration in valve performance that is seen with the slow in-growth of fibrous tissue (pannus) over the sewing ring, a phenomenon also observed with bioprostheses. This over-exuberant fibrous reaction usually develops over years and is likely to be multifactorial in aetiology, relating to local flow conditions, periods of under-anticoagulation, foreign body reaction, and fibroblast activity as well as sewing ring damage and implantation technique. In-growth of fibrous tissue narrows the valve orifice (fig 3), may interfere with occluder movement, and act as a platform for thromboembolism. Reoperation is the only effective treatment.
{kind=link}
{kind=link}
{kind=link}
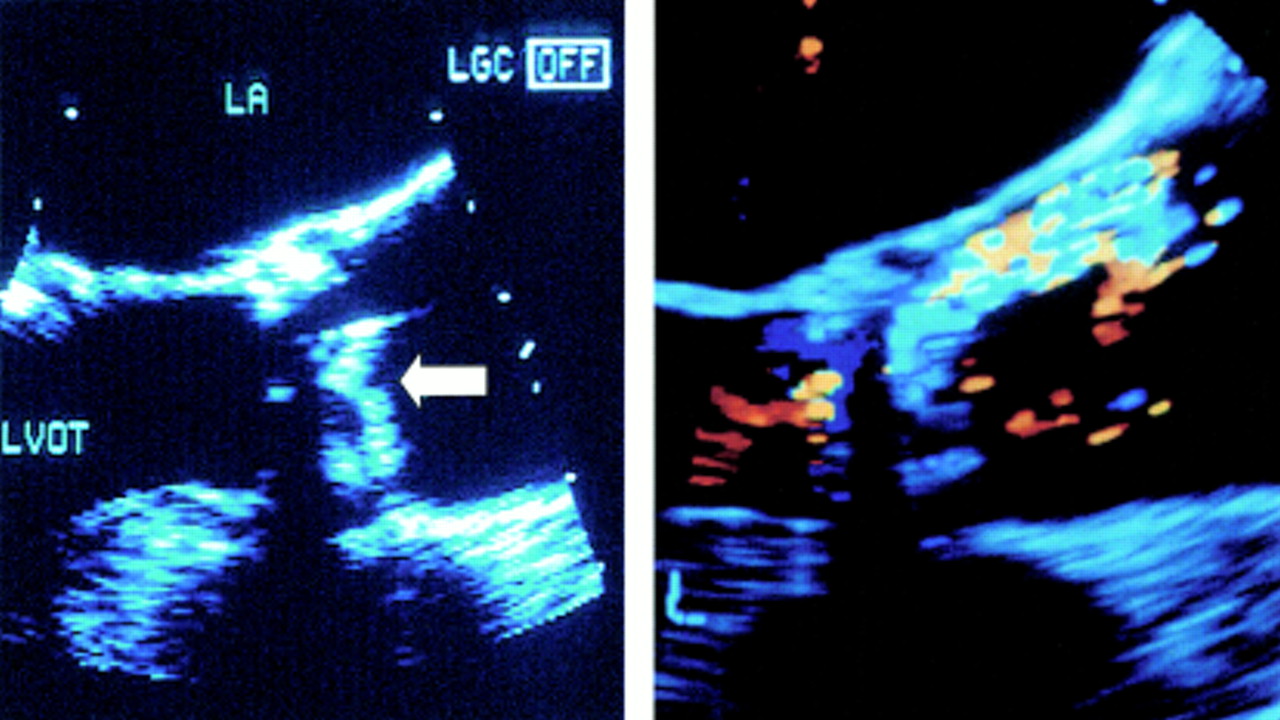
Transoesophageal echocardiographic image of an aortic prosthetic valve partly obstructed by pannus. Grey scale (left) and colour flow (right) images show that the movement of the occluder is limited in systole (arrow). LA, left atrium; LVOT, left ventricular outflow tract.
In biological valves, late degeneration is the major late complication. Pathological changes range from thinning, atrophy, and perforation seen particularly in allografts, through to leaflet calcification, thickening, and tearing seen with porcine and pericardial bioprostheses. Age is the most important determinant of failure with valve degeneration accelerated by youth. Rates of aortic valve failure of 42% are reported at 10 years after implantation of a porcine bioprosthesis in patients aged 21–30 years as compared with 0% in those aged 61–70 years.25 Careful outpatient surveillance is important since presentation is usually gradual, with progressive symptomatic limitation and development of new murmurs.
Follow up after valve surgery
There is an absence of consensus over optimal patient follow up after valve surgery, and the paucity of published clinical studies mandates that clinical practice is usually determined by physician preference and experience. The American Heart Association/American College of Cardiology guidelines26 suggest that a detailed first follow up visit should be undertaken with clinical assessment, ECG, and chest x ray in all patients. Echocardiography is helpful at this stage to document the presence or absence of satisfactory early prosthetic function, to detect residual ventricular dysfunction or pulmonary hypertension, and to serve as a baseline for future examinations should complications or deterioration develop at a later stage. Thereafter, controversy exists as to the necessity, frequency, and optimal location for further outpatient visits in patients who have enjoyed a good result from surgery and who are free of complications. For patients with prosthetic valves, annual hospital follow up has been proposed by some to enable a review of anticoagulation control, to screen for mechanical or haemodynamic problems, and to reinforce advice concerning endocarditis prophylaxis.26 On the other hand, complications from prosthetic valves are rare and usually catastrophic with no definitive evidence existing to suggest that routine screening enhances their detection over and above a strategy of dealing with problems when symptoms develop. Mahy and colleagues27 found routine hospital follow up of limited benefit in detecting or averting complications in asymptomatic patients with prosthetic valves, and reasonably concluded that in the present era of well developed primary care and effective community based anticoagulation clinics, such care could be safely devolved away from the surgical centre provided rapid access was offered to patients with new symptoms. The situation is somewhat different in patients with bioprosthetic valves since valve degeneration is often more insidious, with the development of new murmurs that may be detected and investigated by echocardiography during routine outpatient surveillance.