Article Text

Statistics from Altmetric.com
- CI, confidence interval
- IVUS, intravascular ultrasound
- LPS, lipopolysaccharide
- MI, myocardial infarction
- OR, odds ratio
- PBMC, peripheral blood mononuclear cells
- TNFα, tumour necrosis factor α
Recent studies have rekindled interest in the possibility that infection, particularly by Gram negative bacteria, may contribute to the inflammatory component of atherosclerosis, and that the activation of monocytes/macrophages may contribute to acute myocardial infarction (MI).1 Recently, several groups have studied the association between the (-260)T allele in the gene encoding the CD14 lipopolysaccharide receptor (CD14) and MI, with differing results.2–5 In the present study we examined the association between the CD14 C(-260)T gene polymorphism and the risk of MI with regard to the severity of the coronary artery stenosis at the culprit lesion site. We revealed one possible mechanism by which CD14 polymorphism could affect the degree of activation of peripheral blood mononuclear cells (PBMC) with small amounts of lipopolysaccharide (LPS).
METHODS
Study patients were recruited from 333 patients who underwent heart catheterisation (MI patients, 139; non-MI patients, 194) at Nagoya University Hospital and at Nagoya First Red Cross Hospital in Aichi Prefecture, Japan from January 2000 to August 2000. Non-MI patients included those with arrhythmia, valvar disease or congenital heart disease. MI patients were treated by mutant tissue plasminogen activator before coronary angiography. Coronary artery stenosis was defined as significant when the narrowing of the luminal diameter was > 50% after glyceryl trinitrate administration. Of the total of 139 MI patients, 67 had mild coronary artery stenosis of less than 50% of the adjacent normal coronary artery at the site of the culprit lesion, as determined by intravascular ultrasound (IVUS) study. Written informed consent was obtained from each patient before the study in the hospital. The study protocol adhered to the guidelines approved by the ethics committee of the Nagoya University School of Medicine.
The presence of the C (-260) T variant of the CD14 was determined by polymerase chain reaction-restriction fragment length polymorphism analysis as described previously.2 PBMC were isolated from venous blood of 28 healthy volunteers by centrifugation using Mono-Poly Resolving Medium (Dainippon Pharmaceutical Co, Osaka, Japan) and were stimulated by 10 pg/ml of LPS (Chlamydia trachomatis, Sigma Chemical Co). Tumour necrosis factor α (TNFα) released from PBMC was measured with a commercial assay kit (Quantikine Human TNFα, R and D System). The relative risks of MI associated with each genotype, with 95% confidence intervals (CI), were calculated by multivariate regression models.
RESULTS
In this study, the genotype frequencies were in agreement with those predicted by the Hardy-Weinberg equilibrium in non-MI patients. There was no significant difference in the allele and genotype distribution of the CD14 polymorphism between MIs and non-MIs.
However, when we investigated the association of the CD14 TT genotype among 67 patients, who had insignificant coronary artery stenosis at the site of the culprit lesion, the frequency of the TT genotype was three times higher in the MI patients with insignificant coronary artery stenosis at the culprit lesion (odds ratio (OR) 3.32, 95% CI 1.38 to 8.13).
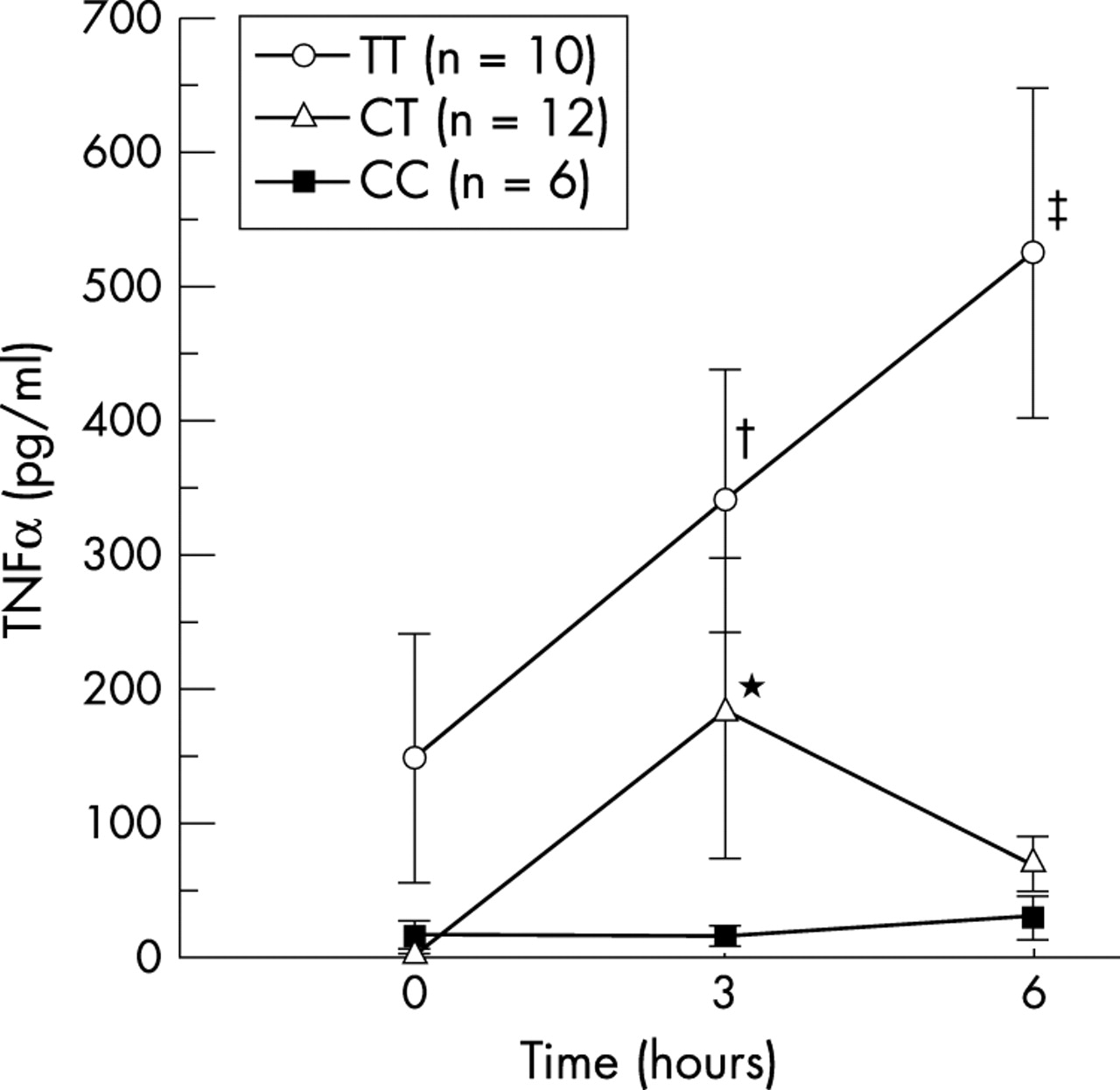
We then investigated whether different CD14 genotypes affected the degree of PMBC activation in response to challenge with a small amount of LPS (10 pg/ml), which mimics the situation of subclinical infection in vivo. We assessed the degree of PMBC activation by measuring the amount of TNFα released in the medium. The concentrations of TNFα were much higher at three and six hours after LPS stimulation in TT genotypes than in CT or CC genotypes (fig 1).

{kind=link}
Concentrations of tumour necrosis factor α (TNFα) released from peripheral blood mononuclear cells (PBMC) by lipopolysaccharide (LPS) challenge in three genotypes. All these experiments were done in triplicate. TNFα concentrations were determined by enzyme linked immunosorbent assay (ELISA). Data are expressed as mean (SE). Among CT genotype subjects, the peak TNFα concentration occurred at three hours and disappeared at six hours after low dose LPS (10 pg/ml) challenge. Among TT genotype subjects, TNFα concentration continued to rise for six hours after low dose LPS challenge. p < 0.05 by two way repeated measured analysis of variance (ANOVA) with Bonferroni post hoc correction. *p < 0.05, CT, 3 h v 0 h and 3 h v 6 h. †p < 0.05, TT, 3 h v 0 h. ‡p < 0.05, TT, 6 h v 3 h.
DISCUSSION
Several groups have reported the association of the CD14 polymorphism with MI, but the results have been inconsistent.2–5 All previous studies examined MI patients with different severity of coronary artery disease. In this study, we revealed that the TT genotype of the CD14 gene was prevalent among MI patients with insignificant coronary artery stenosis at the culprit lesion (OR 3.32). Furthermore, ex vivo investigation revealed that PMBCs derived from TT genotype patients are easily activated in the presence of a small amount of LPS.
Taking these facts into consideration, we may conclude that those with TT genotypes have activation prone macrophage/lymphocytes at their coronary artery plaque. Therefore, even if people with the TT genotype have only mild coronary plaques, this plaque is more likely to rupture, leading to acute MI. To the best of our knowledge, this is the first study to clarify the association of CD14 polymorphism and MI with regard to the culprit coronary artery characteristics. Recent findings suggest that infection and inflammation play a pivotal role in the process of MI, especially by Gram negative bacteria such as Chlamydia pneumoniae.1 As the density of CD14 was about 40% higher in blood monocytes from TT homozygotes than those from the other two genotypes,2 and as CD14 is the main receptor of LPS, monocytes/macrophages from TT homozygotes are thought to be easily activated by a small amount of LPS, after which they release many cytokines, matrix metalloproteinases, and tissue factor when challenged. Indeed, the present study revealed that PMBC from TT homozygotes release a large amount of TNFα when challenged with LPS.
Considering all these facts together, it is tempting to speculate that the coronary plaques of people carrying TT homozygotes have a tendency to rupture because of the existence of activation prone macrophages/lymphocytes, even when there is only a small amount of coronary atheroma.
In line with our data, there is evidence that MI and infection are associated, and that some antibiotic treatments are effective in the prevention of MI. While it may be premature to conclude that antibiotics for the treatment or prevention of MI are generally recommended, our results could provide a means to identify patients (namely TT genotypes) who would benefit from antibiotic treatment for the prevention of MI.
This study has several limitations. First, it is not a randomised case–control study. Moreover, we used a control population including those with arrhythmia, valvar heart disease, and congenital heart disease, which may cause some selection bias. The second limitation is the small study population. Third, we could only assess the results of coronary angiography after MI patients had received thrombolytic treatment. Therefore, we could not determine the exact characteristics of the coronary lesions before those patients had developed MI.