Article Text

Statistics from Altmetric.com
- acute coronary syndromes
- ST segment elevation acute coronary syndrome
- non-ST segment elevation acute coronary syndrome
- myocardial infarction
- reperfusion treatment
- percutaneous coronary intervention
Acute coronary syndrome (ACS) describes a spectrum of clinical conditions ranging from ST segment elevation myocardial infarction (MI) to non-ST segment elevation MI and unstable angina (ACS without enzyme or marker release) (fig 1).

Acute coronary syndrome (ACS) ranges from unstable angina without detectable myocyte necrosis to extensive myocardial infarction (MI). Unstable angina is characterised by the clinical syndrome, undetectable markers (troponin and CK-MB) but with ECG changes (typically ST depression or T wave inversion or transient ST elevation): the risk of death from hospitalisation to six months is approximately 5–8%. Markers are elevated in acute MI in proportion to the extent of myocyte necrosis. For those hospitalised alive, the risk of death is 12–15% in the following six months (GRACE registry data). A spectrum of left ventricular dysfunction exists across ACS ranging from no measurable dysfunction to remodelling, dilatation of the ventricle, and severe systolic dysfunction.
The syndrome is the consequence of disruption of a vulnerable coronary artery plaque, complicated by intraluminal thrombosis, embolisation, and varying degrees of obstruction to perfusion (figs 2 and 3). The severity of coronary arterial obstruction and the volume of affected myocardium determine the characteristics of clinical presentation. Patients with complete occlusion may manifest ST segment elevation infarction if the lesion occludes an artery supplying a substantial volume of myocardium, but the same occlusion in the presence of extensive collateralisation may manifest as infarction without ST segment elevation (non-ST elevation ACS). Similarly, incomplete occlusion at the site of a disrupted arterial plaque may produce ischaemia or microinfarction, depending on the volume of myocardium affected and the extent of distal embolisation. Sensitive and specific markers of myocyte injury (troponins) allow the detection of more subtle volumes of infarction than possible using conventional cardiac enzymes.1–3

High power image of the endothelial lining of a coronary artery with disruption of the endothelium revealing the subendothelial matrix. Platelets are attached to the disrupted endothelium and monocytes invade beneath it.

Low power image of a cross section of a coronary artery of a patient with extensive atheroma. A large lipid rich plaque has ruptured, resulting in an acute coronary syndrome (ACS). The ACS resolved and the plaque reorganised. Subsequent plaque growth encroached upon the lumen. After a further rupture the patient experienced myocardial infarction and sudden death caused by presumed embolisation and arrhythmia. The coronary artery is partially occluded at the time of postmortem examination.
The consequences of ACS are not benign. Among those who survive to reach hospital alive, approximately 12% of patients with ST segment elevation MI will die in the succeeding six months, 13% of those with non-ST segment elevation ACS and 8% with unstable angina (GRACE registry). The frequency of new stroke is between 1.5–3% and rehospitalisation for a further ACS, between 17–20% in the same time interval.
ESTABLISHING A WORKING DIAGNOSIS
Triage of patients into ST segment elevation ACS or non-ST segment elevation ACS is based upon the presence of a typical clinical syndrome plus electrocardiographic changes. Markers of myocyte injury may not be elevated on initial presentation if less than 4–6 hours have elapsed from the onset of ischaemia (due to the time course of release from cardiac myocytes).
Among those without ST elevation on the ECG, an ACS is diagnosed by the presence of a clinical syndrome of acute ischaemia with either rest pain or a crescendo pattern of ischaemic pain on minimal exertion, plus electrocardiographic and/or marker evidence of acute ischaemic injury. The predictive accuracy of ST elevation for a final diagnosis of MI is very high, but for non-ST elevation MI, less than 50% are suspected as infarction on initial presentation.
Within the spectrum of ACS, non-ST elevation MI presents the most difficult diagnostic challenge. In non-ST MI the ECG changes may consist of ST segment depression (or transient ST elevation) or T wave inversion. Separation of non-ST segment elevation MI from unstable angina is on the basis of marker or enzyme elevation in the former and the absence of detectable marker release in the latter (repeat assay at 12 hours after presentation is recommended). The management strategy of non-ST elevation ACS is determined by whether high risk features are present (fig 4). Imaging techniques (echocardiography, single photon emission computed tomography (SPECT) or magnetic resonance imaging (MRI)) can detect wall motion abnormalities in patients with recent or established infarction. The sensitivity of SPECT is sufficient to detect infarcts of at least 10 g, but MRI with gadolinium enhancement may detect infarcts as small as 1–5 g.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
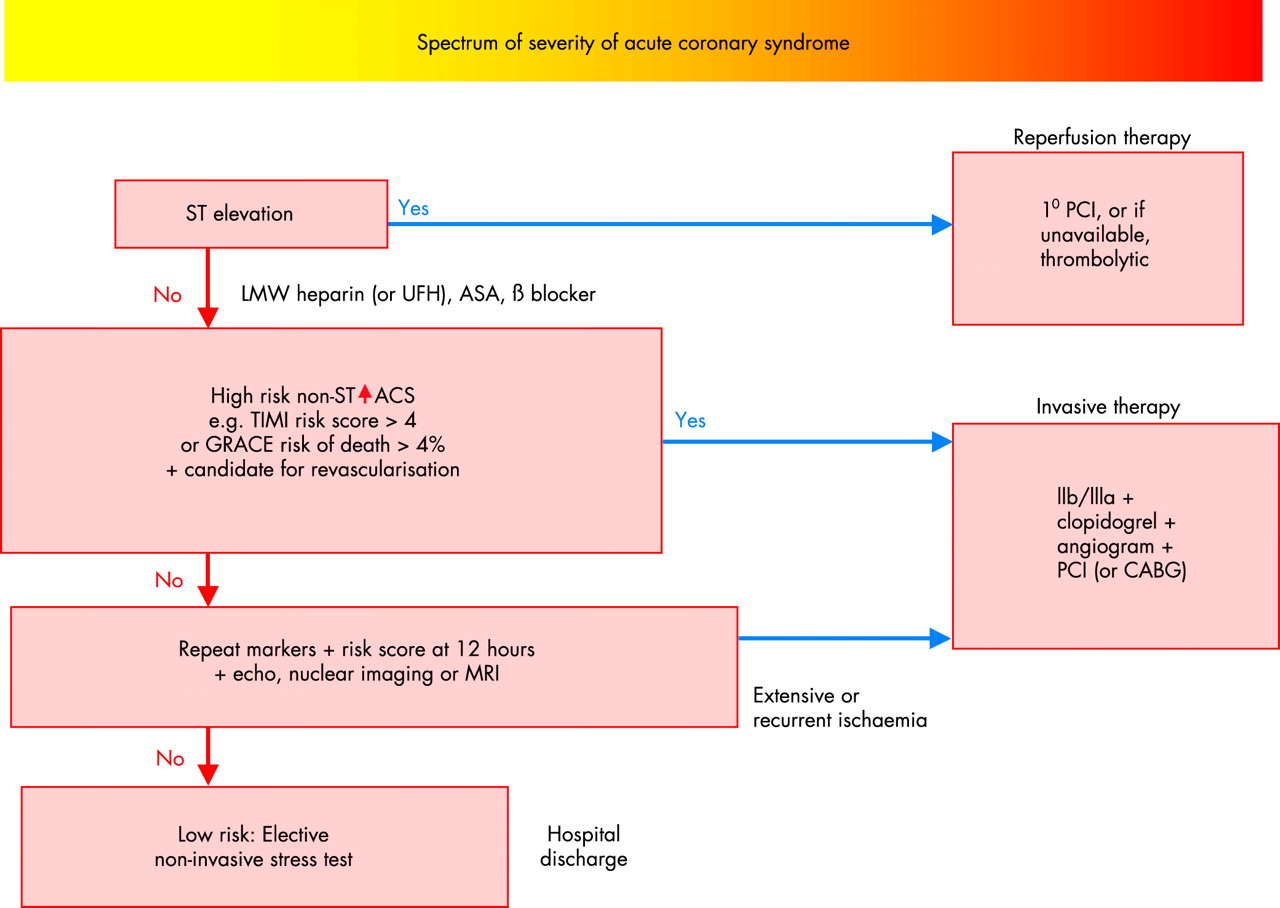
Schematic of the management of acute coronary syndrome (ACS) (see text for details). In the presence of a typical clinical syndrome and persistent ST elevation, a patient should proceed to reperfusion therapy with primary percutaneous coronary intervention (1° PCI) or, if unavailable, thrombolytic treatment. The remaining patients have non-ST elevation ACS. If high risk features are present, invasive treatment is indicated combined with a Gp IIb/IIIa inhibitor and clopidogrel. In the absence of high risk features repeat estimations of markers should be performed at 12 hours, and echocardiography, nuclear imaging or MRI may be used to detect evidence of ischaemia or necrosis. Low risk patients should undergo elective non-invasive stress testing to determine whether stable but obstructive coronary artery disease is present. Low risk patients are candidates for early hospital discharge.
THE REVISED DEFINITION OF ACUTE MYOCARDIAL INFARCTION
The more sensitive definition of MI proposed by the European Society of Cardiology (ESC), the American College of Cardiology (ACC), and the American Heart Association (AHA) requires a typical clinical syndrome plus a rise and fall in troponin (or creatine kinase-MB (CK-MB)) to values greater than 99% of a normal reference population (with less than 10% coefficient of variation of the assay).4 Troponin assays with more than 10% coefficient of variation at the decision limit will result in false negative and false positive results when the true result is close to this limit.
As a result of this more sensitive definition approximately 25% of those that would previously have been classified as unstable angina now fulfil the criteria for MI. This has important implications for patients, for interpreting outcome, and for planning future management.4
ACUTE MANAGEMENT AND EARLY RISK STRATIFICATION AS A GUIDE TO TREATMENT
Among industrialised communities suspected ACS constitutes the largest indication for acute medical hospitalisation. Separating ACS from the larger cohort of patients with non-specific or non-cardiac chest pain presents an urgent challenge. This is critical not only for those with ST segment elevation, but also to minimise the risk of fatal and non-fatal complications in non-ST elevation ACS.
A working diagnosis of ACS can be made on first presentation to medical care on the basis of a typical clinical syndrome accompanied by electrocardiographic changes of ischaemia (ST segment depression or T wave inversion). Biomarkers of myocyte injury may be elevated when ischaemia has been present for at least 4–6 hours or if preceding myocardial injury has taken place. An elevated biomarker of injury (at presentation) signifies increased risk of death in either ST elevation or non-ST elevation MI, but the absence of such elevation may simply reflect the lag before sufficient concentrations of the marker are detectable.5
A repeat assay is required following an initially negative measurement. However, urgent management should not be delayed awaiting the results of such assays. Thus, immediately after hospital presentation a sequence of decisions is required:
-
ACS or not, based on clinical and ECG (± echo) features
-
Candidate for emergency reperfusion or not—ST segment elevation or true posterior MI or left bundle branch block (LBBB)
-
Low or high risk non-ST elevation ACS (table 1, fig 4). This guides future treatment.
High risk features and markers of patients with non-ST elevation ACS
General measures
The underlying principles are to provide pain relief, adequate arterial oxygen concentration, and relief of ischaemia. In the presence of heart failure or shock, assisted ventilation with positive end expiratory pressures may be required. Reperfusion of critically ischaemic myocardium is crucial in those with acute ST elevation (or LBBB or posterior MI). Haemodynamic support may be necessary in patients with hypotension or cardiogenic shock (including intra-aortic balloon pumping to stabilise the patient for percutaneous coronary intervention (PCI)). Specific measures may be required to control hypertension to reduce myocardial wall stress, and to treat acute heart failure and mechanical complications.
Recent advances in anti-thrombotic and revascularisation treatments are described in the following sections but established therapies are only summarised briefly.
MANAGEMENT OF ST SEGMENT ELEVATION ACS
The aims of acute management are:
-
to establish rapidly a working diagnosis following presentation
-
to treat acute arrhythmic and haemodynamic complications including cardiac arrest
-
to provide prompt pain relief and adequate arterial oxygen concentrations
-
to initiate reperfusion therapy to limit the extent of infarction and minimise complications of pump failure and arrhythmias
-
to treat complications of acute MI
-
to provide risk assessment for longer term management and to initiate secondary prevention.
A working diagnosis of an acute evolving MI is made in the presence of clinical symptoms consistent with acute MI and specific ECG changes:
-
ST elevation of ⩾ 0.2 mV in leads VI–V3 or ⩾ 0.1 mV in other leads
-
ST segment depression consistent with posterior MI
-
Established MI (either old or recent) may be defined by the presence of Q waves of ⩾ 0.03 s in leads V1–V6 or II, aVL, aVF.
Haemodynamic compromise and cardiac arrest
Resuscitation may be required for ventricular fibrillation or for ventricular tachycardia with diminished cardiac output, and guidelines for such resuscitation are provided within the framework of Basic and Advanced Life Support. For the patient with extensive myocardial ischaemia and/or heart failure, additional circulatory support may be necessary, including the insertion of an intra-aortic balloon pump, as a bridge to revascularisation.
Reperfusion therapy
Prompt and effective reperfusion therapy is the cornerstone of treatment for acute ST elevation MI and is the only widely applicable acute treatment to diminish infarct size and major cardiac complications.
In trials of fibrinolysis versus control more that 150 000 patients have been randomised and the overall treatment benefit is approximately 50 lives saved per 1000 patients treated for the combination of thrombolytic agent and aspirin.6 Time delay is critically important, especially within the first four hours following symptom onset.7 Overall, there is a progressive decrease of about 1.6 deaths per hour of delay, per 1000 patients treated. However, within the first two hours the reduction in mortality is twice as large as beyond two hours (based on a meta-analysis of 22 trials). Hence, the European guidelines for the management of acute MI recommend that for those patients with clear cut changes of acute infarction, no more than 20 minutes should elapse between hospital arrival and the administration of thrombolytic therapy (or pre-hospital administration) or no more than 60 minutes between hospital arrival and balloon inflation for primary PCI.2 A second and critically important reason for minimising pre-hospital delay is to treat early ventricular fibrillation. At least as many deaths may be saved by prompt resuscitation therapy in early acute infarction as saved by reperfusion therapy.
Limitations and hazards of fibrinolysis
The major limitation of fibrinolytic drug treatment is that reperfusion is gradual, and incomplete or inadequate in a significant proportion of patients. This proportion may range from about 40% (failure to achieve TIMI 3 flow within the first three hours of reperfusion therapy) with streptokinase to 20–30% with tissue plasminogen activator (tPA) or tenecteplase (TNK). The principal hazard is intracranial haemorrhage: overall about four extra strokes occur per 1000 patients treated and, of these, two are fatal. These limitations have led to the testing of alternative fibrinolytic regimens and to the development of primary PCI. Overall, the use of accelerated tPA (alteplase) results in 10 fewer deaths per 1000 patients treated, but at the risk of three additional strokes compared with streptokinase treatment.8 Single bolus agents provide logistic advantages and both reteplase-PA or weight adjusted TNK have equivalent efficacy to accelerated tPA. TNK has a lower rate of non-cerebral bleeds and a lesser need for blood transfusion. Bolus agents are particularly advantageous in minimising time delay in the pre-hospital and emergency room settings.
Fibrinolysis combined with newer anti-thrombotic agents
The combination of glycoprotein (Gp) IIb/IIIa inhibitors and fibrinolysis has been tested in seven trials, including two large trials (ASSENT 3 and GUSTO V) involving more than 30 000 patients. There was no overall advantage for combining the lytic agent with a Gp IIb/IIIa inhibitor. In patients over 70 years of age the combination increased the risk of intracranial haemorrhage and extracranial bleeding (risk ratio 1.98, 95% confidence interval (CI) 1.65 to 2.38).8 Similarly, the combination of streptokinase with a specific anti-thrombin (bivalirudin) failed to improve survival in the HERO 2 trial.
Thus, the limits appear to have been reached in the balance of efficacy versus safety with more aggressive anti-thrombotic regimens for ST elevation MI.
Primary PCI
Individual trials comparing fibrinolytic therapy with primary PCI and the meta-analysis of such trials have demonstrated that, provided primary PCI can be administered promptly and by an experienced team, it is superior to the fibrinolytic therapy and it avoids the hazards of excess cerebral and systemic bleeding.9 Lower mortality rates have been reported among patients undergoing primary PCI in centres with a high volume of PCI procedures compared with low volume centres, demonstrating the need for an experienced team (interventional cardiologists and skilled supporting staff). For hospitals without on-site PCI facilities careful consideration needs to be given to the potential benefits of PCI following transfer to an intervention centre versus fibrinolysis. The DANAMI 2 study suggests that for transfer times of two hours or less from a community hospital to the start of PCI, a significant reduction in death, reinfarction, and stroke is observed compared with thrombolysis. In summary, a series of studies have demonstrated more effective restoration of patency with PCI compared to fibrinolysis, less reocclusion, improved left ventricular function, and better clinical outcome.9
Primary PCI is therefore the preferred strategy for patients with acute ST elevation MI if, with appropriate facilities, a skilled team can provide PCI within 60 minutes of hospital arrival.
PCI combined with fibrinolysis
Moderate sized studies with combined end points have investigated “facilitated PCI” where the fibrinolytic agent is administered followed by PCI. These strategies may offer advantages but larger scale trials are awaited. The recent BRAVE trial (American Heart Association hotline 2003) examined the impact of PCI with two boluses of 5 U reteplase plus abciximab, versus abciximab alone (12 hours). The infarct size was not improved after PCI with reteplase, and bleeding was more frequent.
PCI combined with Gp IIb/IIIa (abciximab)
The combination of Gp IIb/IIIa inhibitors and primary PCI has been tested in several studies (RAPPORT, ISAR 2, CADILLAC, ADMIRAL, and ACE trials, n = 3666). The pooled analysis suggests that Gp IIb/IIIa inhibition reduces adverse outcomes (death/MI or the combination with target vessel revascularisation) in primary PCI (without a lytic agent). Death or MI at 30 days was 3.2% (59/1843) with abciximab versus 4.8% (88/1823) without, based on the pooled analysis.10
In summary, although individual trials do not provide conclusive evidence for reducing death/MI, all do reduce target vessel revascularisation. The pooled analysis suggests a clear benefit in reducing MI when primary PCI is combined with abciximab.10 Thus, for primary PCI addition of Gp IIb/IIIa (abciximab) may be regarded as the modern reference standard. In contrast “upstream” use of a thrombolytic agent does not show clear evidence of benefit.
Rescue PCI
Rescue PCI refers to a PCI procedure performed in patients without evidence of a response to thrombolysis (< 50% ST segment resolution) and feasibility studies have demonstrated success of PCI in achieving coronary patency and flow. However, insufficient data are available to demonstrate whether there is improvement in mortality or further MI; such studies are still underway.
Shortfall in the provision of reperfusion therapy
Despite the clearly demonstrated survival and clinical advantages of prompt reperfusion therapy, approximately one third of patients fail to receive any form of reperfusion (despite presenting with ST segment elevation within 12 hours of symptom onset and without contraindications to reperfusion). A similar frequency occurs in the USA (33%), Europe (29%), Australia, New Zealand, and Canada (29%), and Argentina and Brazil (28%).11
Specific factors predict the failure to undergo reperfusion and these include previous coronary artery bypass graft (CABG) surgery, diabetes, a presentation with heart failure, a presentation without chest pain, and age greater than 75 years.11 The proportion of primary PCI varies widely across geographic regions but most reperfusion is still achieved with fibrinolysis.
An important shortfall in reperfusion therapy therefore exists and this is predominantly among patients with more complicated disease, with atypical presentation, and with advanced age.
The original fibrinolytic trials had limited power to demonstrate benefit or hazard among patients more than 75 years of age, but a re-analysis of the Fibrinolytic Trialist’s Collaboration in 3300 patients over 75 years, presenting within 12 hours of symptom onset, has demonstrated a significant reduction in mortality from 29.4% to 26%, (p = 0.03).
Symptoms of infarction but non-diagnostic ECG changes
During the early evolution of infarction the ECG may be abnormal without significant ST elevation. Typical changes may evolve over minutes or hours and it is critically important to institute continuous ST monitoring or perform repeat ECGs to ensure that such evolution is detected promptly.
In patients with symptoms suggestive of infarction, but without diagnostic ECG changes, alternative diagnoses must be considered (including aortic dissection, gastro-oesophageal disease, and musculoskeletal and mediastinal conditions). An echocardiogram demonstrating normal ventricular function in the presence of suspected cardiac pain should prompt the search for an alternative diagnosis. Similarly, myocardial perfusion scintigraphy or MRI may be used to detect the presence of ischaemia or infarction and a normal result effectively excludes significant MI.
ECG changes without typical symptoms
Certain groups of patients, including the elderly and those with diabetes, may present without typical symptoms of MI. They may present with or evolve ECG changes of MI and haemodynamic or mechanical complications. Their treatment should be similar to patients with typical painful infarction.
MANAGEMENT OF NON-ST SEGMENT ELEVATION ACS
General features
The patient with non-ST segment ACS (ranging from non-ST segment elevation MI to unstable angina without evidence of enzyme or marker release) is at risk of major cardiovascular complications and death, and the extent of this risk is dependent upon acute and pre-existing risk factors (fig 1, table 1). These risk factors not only predict the hazards of early cardiac events but also of future cerebrovascular and peripheral vascular complications.
Certain markers reflect an upregulation of the inflammatory/thrombotic systems (for example, high sensitivity C reactive protein (hsCRP), interleukin 6 (IL-6), CD40 ligand, and platelet–monocyte complexes). These inflammatory markers may be upregulated before the patient’s presentation with ACS, but acute phase reactant markers are also elevated as a consequence of myocyte injury. Elevation of both hsCRP and troponin signifies a substantially higher risk of death (approximately 14% at one year) than either marker alone, and in the absence of both markers the patient is at very low risk of future cardiac events (< 2%) based on FRISC 2 data.12 Importantly, whereas troponins predict the hazard of acute events (including acute MI and death), hsCRP on presentation does not independently predict the risk of death during hospitalisation but is a powerful predictor of death in the following 1–2 years.
The extent to which these biomarkers add to the predictive accuracy of established risk models (TIMI risk score, C index 0.65, or GRACE risk score, C index 0.84) remains to be tested.13 Nevertheless, the established risk scoring systems provide robust methods of categorising patients into low, mid, or high risk groups, as a basis for further treatment (table 2).
Independent predictors of death in patients presenting with the spectrum of ACS based upon widely available clinical and biological markers
Impairment of cardiac muscle function, as manifest by the presence of heart failure (Killip class) is a powerful and independent predictor of death; more recently, subtle evidence of myocardial dysfunction in ACS (as measured by brain type natriuretic peptide, or N terminal pro BNP) is a powerful predictor of death. Renal dysfunction may be the consequence of pre-existing atheromatous disease and may undergo further deterioration as a consequence of ACS. Although overt renal dysfunction has been recognised as an adverse marker, more subtle elevations of creatinine or creatinine clearance have recently been demonstrated to be independent predictors of death, even in the absence of previously recognised renal dysfunction.14
Markers of ischaemia and intravascular thrombosis
Recurrent ischaemia, at rest, is a powerful indicator of higher risk, especially when accompanied by dynamic ST changes. ST elevation and ST depression are well recognised electrocardiographic markers of risk; however, it has recently been demonstrated that ST deviation conveys the same risk for death whether this deviation is upwards or downwards (having controlled for the other elements of baseline risk).13
Extensive evidence supports the powerful and independent prediction of thrombotic complications, including MI and death, associated with troponin elevation.5 Furthermore, the evidence from trials of PCI revascularisation suggests that troponins can be used as part of the measures to identify higher risk (but not the sole arbiter of risk), and the potential for gain from the interventional procedures.15,16 Newer generation troponin assays have higher sensitivity and diagnostic accuracy. With newer generation assays very minor increases in troponins can detect myocyte necrosis in as little as 1 g of myocardium. These minor increases do predict a higher risk of cardiac complications and death. In all instances the risk predictors should inform rather than replace clinical judgement.
Antiplatelet treatment
The most recent update of the Anti-thrombotic Trialists’ Collaboration, based upon 287 studies in 135 000 patients, demonstrates a highly significant reduction in the risk of MI/stroke/vascular death as a result of antiplatelet treatment (principally aspirin) versus control.7 Overall, the event rates were 13.2% in control patients and 10.7% in those treated with antiplatelet therapy, a 22% relative risk reduction.7 In acute MI, and in other high risk patients, the absolute and relative risk reductions were greater: 23 per 1000 fewer vascular deaths and 13 per 1000 fewer MIs. Thus, abundant evidence supports the use of aspirin in patients with ACS. Additional antiplatelet treatment requires evidence of benefit on top of aspirin, rather than as an alternative to aspirin. Recent data suggest that bleeding risk doubles for aspirin doses above versus below 100 mg daily, with no improved efficacy.
Thienopyridines (ADP antagonists)
Thienopyridines inhibit ADP mediated platelet aggregation and, although initial studies were conducted with ticlopidine, this has been superseded by clopidogrel, on account of much superior safety. The CURE trial tested clopidogrel in 12 562 non-ST segment elevation ACS patients on top of background treatment and aspirin.17 A 2.1% absolute risk reduction (20% relative risk reduction, p < 0.0001) occurred in the frequency of non-fatal MI, stroke, or cardiovascular death.17 The treatment effect was evident within the first 24 hours of starting therapy and although the absolute benefits were greatest in the first three months of treatment, the relative risk reduction was the same beyond three months. Approximately 1% more patients experienced major bleeding, but there was no significant excess of life threatening bleeding nor haemorrhagic strokes.17 Nevertheless, in view of the irreversible nature of the ADP antagonism current guidelines suggest that clopidogrel should be withheld for five days before CABG surgery. In candidates for very urgent CABG a small molecule Gp IIb/IIIa inhibitor (eptifibatide or tirofiban) can be used before surgery.
In non-ST segment elevation ACS, the ESC and AHA/ACC guidelines recommend approximately nine months treatment with clopidogrel.1,3 Longer term treatment in higher vascular risk patients awaits the results of the large scale CHARISMA trial. As yet, there is no robust evidence for the use of clopidogrel in acute ST elevation MI treated with thrombolysis (other than to cover stent implantation).
Thienopyridines reduce the risk of stent thrombotic occlusion and are now part of standard treatment for at least four weeks in all patients undergoing elective PCI. With drug eluting stents, at least six months and perhaps 12 months of clopidogrel and aspirin are required. With PCI in ACS there is evidence for benefit for one year of treatment (PCI CURE and CREDO trials).
Glycoprotein IIb/IIIa receptors
Platelet aggregation involves the Gp IIb/IIIa receptor linked to fibrinogen or von Willebrand factor. Intravenous Gp IIb/IIIa receptor antagonists have been extensively tested in patients with ACS and in a meta-analysis of all the major randomised trials the absolute risk reduction for death or MI at 30 days was 1% (11.8% control v 10.8% with Gp IIb/IIIa).18 The absolute treatment benefit was largest in high risk patients—in particular, those with evidence of troponin release or those undergoing acute PCI.18 Among those without troponin elevation or without PCI no significant benefits were observed with Gp IIb/IIIa administration.
The CREDO trial has helped to resolve the question of whether clopidogrel plus Gp IIb/IIIa receptor antagonists may be required in patients undergoing PCI. Approximately half of the patients received Gp IIb/IIIa antagonists (a non-randomised subset) and two thirds had presented with an ACS. The frequency of MI, stroke, or death at one year was reduced with clopidogrel from 11.5% to 8.5% (p = 0.02), with similar risk ratios in the presence or absence of Gp IIb/IIIa inhibitors. However, in lower risk patients both of the platelet antagonists may not be required: the ISAR-REACT trial (n = 2100 patients) did not show additional benefits for abciximab in the presence of background treatment of aspirin and clopidogrel (loading dose 600 mg given more than two hours before PCI).
There is no evidence to support the use of oral Gp IIb/IIIa antagonists following ACS. Partial or transient inhibition of the IIb/IIIa receptor may upregulate platelet activation, and the composite of trials of oral Gp IIb/IIIa inhibitors suggests an increased risk of death.
In summary, aspirin remains the cornerstone of antiplatelet treatment in patients with ACS. Robust evidence supports the use of clopidogrel in patients presenting with non-ST elevation ACS (at least up to nine months) and extensive evidence supports the use of intravenous Gp IIb/IIIa inhibitors in high risk patients with ACS, especially those undergoing acute PCI.
Trial acronyms
-
ACE: Anticoagulation in Cardioversion using Enoxaparin
-
ADMIRAL: Abciximab before Direct angioplasty and stenting in Myocardial Infarction Regarding Acute and Long term follow up
-
ASSENT: ASsessment of the Safety and Efficacy of a New Thrombolytic
-
BRAVE: Bavarian Reperfusion Alternatives Evaluation
-
CADILLAC: Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications
-
CHARISMA: Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance
-
CREDO: Clopidogrel for the Reduction of Events During Observation
-
CURE: Clopidogrel in Unstable angina to prevent Recurrent Events
-
DANAMI: DANish Acute Myocardial Infarction
-
ESSENCE: Efficacy and Safety of Subcutaneous Enoxaparin in Non-Q-wave Coronary Events
-
FRISC: Fragmin and fast Revascularization during InStability in Coronary artery disease
-
GRACE: Global Registry of Acute Coronary Events
-
GUSTO: Global Use of Strategies To Open occluded coronary arteries
-
HERO: Hirulog and Early Reperfusion or Occlusion
-
INTERACT: INTegrilin and Enoxaparin Randomization assessment of Acute Coronary syndromes Treatment
-
ISAR: Intracoronary Stenting and Antithrombotic Regimen
-
NICE: National Investigators Collaborating on Enoxaparin
-
OASIS: Organization to Assess Ischemic Syndromes
-
PENTUA: PENTasaccharide in Unstable Angina
-
RAPPORT: ReoPro and Primary PTCA Organization and Randomized Trial
-
RITA: Randomized Intervention Trial of unstable Angina
-
SPORTIF: Stroke Prevention using ORal Thrombin Inhibitor in atrial Fibrillation
-
SYNERGY: Superior Yield of New strategy of Enoxaparin Revascularization and Glycoprotein IIb/IIIa Inhibitor
-
TACTICS: Treat angina with Aggrastat and determine Cost of Therapy with an Invasive or Conservative Strategy
-
TIMI: Thrombolysis In Myocardial Infarction
Anti-thrombin treatment
Thrombin is a highly potent stimulus not only of the generation of fibrin, but also platelet activation. In addition it leads to monocyte chemotaxis, to mitogenesis, to increased permeability of the vascular wall, and to secretion of cytokines and growth factors from smooth muscle cells. Effective anti-thrombotic treatment requires inhibition of platelet function and inhibition of thrombin.
Unfractionated heparin has been widely used but it suffers from practical difficulties in maintaining anti-thrombin activity within the therapeutic range (influenced by acute phase proteins and the binding to anti-thrombins). Nevertheless, there is clear evidence that a form of heparin, either unfractionated or low molecular weight heparin (LMWH), is superior to placebo in patients with ACS. The meta-analysis of trials demonstrates a reduction in absolute rates of death or MI from 7.4% to 4.5% (odds ratio 0.53, 95% CI 0.38 to 0.73). Although a meta-analysis of all the trials of LMWH versus unfractionated heparin has not demonstrated a significant advantage in death or MI (at 48 hours), biological and clinical heterogeneity exists among the LMHWs. A meta-analysis of the two trials of enoxaparin (ESSENCE and TIMI 11B) has demonstrated a significant reduction in death or MI (odds ratio 0.82, 95% CI 0.69 to 0.97). Both the European and North American guidelines on ACS suggest that enoxaparin is the preferred anti-thrombin.
Regarding safety, observational studies suggest a similar safety profile for LMWH and unfractionated heparin in the presence or absence of Gp IIb/IIIa inhibitors (NICE studies), and moderate sized randomised trials of enoxaparin versus unfractionated heparin suggest similar or superior safety and efficacy for enoxaparin in Gp IIb/IIIa treated patients (A to Z and INTERACT studies). Preliminary data from the large scale SYNERGY trial suggests that enoxaparin has similar efficacy to unfractionated heparin in patients undergoing PCI, but the bleeding risks appear slightly higher (American College of Cardiology hotline presentation 2004).
Direct anti-thrombins may provide significant advantages over the indirect inhibitors (unfractionated and LMWH). However, in ACS patients the GUSTO IIB trial failed to demonstrate a sustained benefit at 30 days, and in OASIS 2, although the early absolute benefits were maintained for hirudin versus unfractionated heparin, this difference was no longer significant during follow up. Nevertheless, combined analysis of the hirudin studies suggests a relative risk reduction compared to unfractionated heparin. Hirudin has only been approved for patients with heparin induced thrombocytopenia and none of the hirudins are licensed for ACS.
LMWHs partially inhibit factor Xa of the coagulation cascade, but newer specific inhibitors of Xa have been developed—for example, the pentasaccharide, fondaparinux. Such agents inhibit thrombin generation as distinct from thrombin activity. Direct comparisons with LMWH have shown advantages for fondaparinux over enoxaparin in the prevention of deep vein thrombosis (odds ratio 0.55, 95% CI 0.73 to 0.36), but the deep vein thrombosis prophylaxis dose of enoxaparin is lower than for ACS. In a dose ranging study of fondaparinux in ACS (PENTUA study) similar efficacy was seen with enoxaparin and similar rates of major and minor bleeding. The result of a phase III trial is awaited (OASIS 5).
An alternative approach involves an orally administered direct thrombin antagonist ximelagatran. It is converted to melagatran in the circulation and directly binds with the active site of the thrombin molecule. Ximelagatran does not require anticoagulation monitoring and is administered as a fixed dose. In a phase II trial it reduced the frequency of death, non-fatal MI, and severe recurrent ischaemia compared to placebo treatment (hazard ratio 0.76, 95% CI 0.59 to 0.98).19 Ximelagatran has also been used as an alternative to warfarin in the management of atrial fibrillation (SPORTIF trials) and demonstrates similar efficacy but less bleeding than warfarin. A potential hazard of ximelagatran involves alterations in liver enzymes: 6–10% of patients experience a rise in alanine aminotransferase to at least three times the upper limit of normal.19 This appears to resolve with or without cessation of drug treatment. Widespread application of ximelagatran as an alternative to other anti-thrombins in ACS requires large scale safety and efficacy studies.
Intervention in non-ST elevation ACS
Among patients presenting with ACS, but without persistent ST elevation, current guidelines recommend angiography and Gp IIb/IIIa inhibitors for those identified to be at higher risk. The current US guidelines (2002) suggest that either an interventional or a conservative strategy is appropriate in patients at moderate or low risk, but invasive strategies are recommended for those at higher risk.1
Based on a meta-analysis of all of the trials of intervention in ACS there is a reduction in death or MI with the interventional strategy (risk ratio 0.88, 95% CI 0.78 to 0.99).20 However, significant heterogeneity exists among the trials, and the older trials did not employ modern interventional techniques nor modern pharmacological therapy. The FRISC 2 trial independently demonstrated an impact on death or on death/MI (risk ratio 0.78, 95% CI 0.62 to 0.98). Similarly, the TACTICS TIMI 18 trial demonstrated a reduction in the composite of death, MI, and rehospitalisation for ACS as a result of the interventional strategy (in tirofiban treated patients).16
RITA 3 examined whether an interventional strategy was superior in moderate risk patients and demonstrated a significant reduction in the composite end point of death, MI, or refractory angina (from 14.5% to 9.6%, risk ratio 0.66, 95% CI 0.51 to 0.85).20 The major part of the benefit was a reduction in refractory angina but the curves for death/MI progressively separated in favour of the intervention strategy over prolonged follow up.20 Uncertainty remains about the benefits of an interventional strategy in women as both FRISC 2 and RITA 3 showed adverse trends in women (for death/MI) but clear benefits for men. The composite end point was improved in women in TACTICS but there was no independent effect on death/MI. This remains to be resolved.
Management of ACS: key points
-
Acute coronary syndrome (ACS) describes the clinical manifestations of disruption of coronary arterial plaque complicated by intraluminal thrombosis and distal embolisation
-
The severity of the syndrome is determined by the volume of myocardium affected and the extent of ischaemia and myocyte necrosis
-
Emergency primary percutaneous coronary intervention (PCI) is the preferred reperfusion strategy for ST elevation myocardial infarction (MI), but when unavailable thrombolysis substantially improves survival and outcome
-
The risks of non-ST elevation ACS have been underestimated: one in eight patients will die within six months and one in five will require emergency hospitalisation
-
Antiplatelet (aspirin and a thienopyridine) and anti-thrombin (low molecular weight heparin or unfractionated heparin) treatment improves outcome, and β blockers and nitrates reduce ischaemia
-
Death, MI, and refractory angina can be reduced with an interventional strategy (angiography followed by PCI or coronary artery bypass surgery) in higher risk patients
-
Glycoprotein IIb/IIIa inhibitors reduce cardiac complications, especially in those patients proceeding to intervention
-
Recent advances in anti-thrombotic and revascularisation treatments have been shown to reduce serious cardiac complications, rehospitalisations, and deaths in patients with ACS
-
However, these improvements in outcome require prompt and effective triage systems and consistent application of evidence based treatments: a substantial shortfall exists in clinical practice
The benefits of intervention are related to the risk status of the patient. The majority of benefit is seen in those with a TIMI risk score of > 3 points (each component contributes one point: prior coronary stenosis, ⩾ 2 anginal events in the preceding 24 hours, prior aspirin therapy within seven days, ST deviation on ECG, elevated cardiac markers, ⩾ 3 risk factors for coronary artery disease). FRISC 2 demonstrated that most of the benefits occur in those with ST segment depression, troponin elevation, or IL-6 elevation. Thus, it may be possible to resolve whether the patient is likely to benefit from an interventional strategy by applying either the TIMI risk score or the GRACE risk score (table 2, fig 4). In the future, biomarkers (including inflammatory markers) may add to the predictive accuracy of these risk scores.
AN INTEGRATED APPROACH TO THE MANAGEMENT OF ACS
Whereas the risks of ST segment elevation ACS are maximal in the minutes and hours after coronary occlusion, the risks in non-ST segment elevation ACS continue over time, as a result of further thrombotic events. For all patients with ACS the maximum risk of coronary events occurs in the first three months after presentation and treatments are designed to minimise this risk.
For those with suspected ST segment elevation MI, emergency management necessitates access to resuscitation facilities and prompt reperfusion. Current evidence suggests that primary PCI is superior to thrombolysis provided that it can be delivered promptly and in expert hands. The limited availability of interventional facilities in most countries suggests that a substantial proportion of patients will require reperfusion with thrombolytic treatment, at least over the next decade. This can be administered in the pre-hospital setting (provided that adequate diagnostic and resuscitation facilities are available at the point of first patient contact), or at the latest should be administered immediately after arrival in the emergency department. Most benefit is gained from reperfusion within the first 1–2 hours from symptom onset. Differences between lytic regimens are modest in comparison with the difference between failure to provide any reperfusion (in approximately one third of eligible patients) and the remainder. Thus, the urgent priority for ST segment elevation ACS is to provide prompt and effective reperfusion for all those eligible. Substantial evidence demonstrates that this approach will reduce acute complications, heart failure, and death.
In the remainder of patients without ST elevation, the first priority is to establish a working diagnosis based upon the clinical syndrome, ECG, and markers of necrosis (fig 4). These patients present a diagnostic challenge. Pharmacological treatment aims to reduce ischaemia, inhibit platelet aggregation, and inhibit thrombin generation. High risk patients require combination therapy with Gp IIb/IIIa administration and angiography with a view to PCI or surgical revascularisation. In lower risk patients repeat ECGs or ST segment monitoring will detect evolving infarction and subsequent measurements of troponin elevation will reveal those at increased risk. In the absence of clinical/ECG signs of recurrent ischaemia or troponin elevation, the patient is at low thrombotic risk but may have important underlying coronary disease. Elective stress testing is required to determine whether or not stable but obstructive coronary artery disease is present.
In summary, a rapid evolution of pharmacological and interventional strategies has improved acute and longer term outcome for patients presenting with ACS. Significant risks remain and strenuous efforts are required to reduce this risk without increasing the hazards of treatment.
REFERENCES
Linked Articles
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea
- Miscellanea