Article Text

Statistics from Altmetric.com
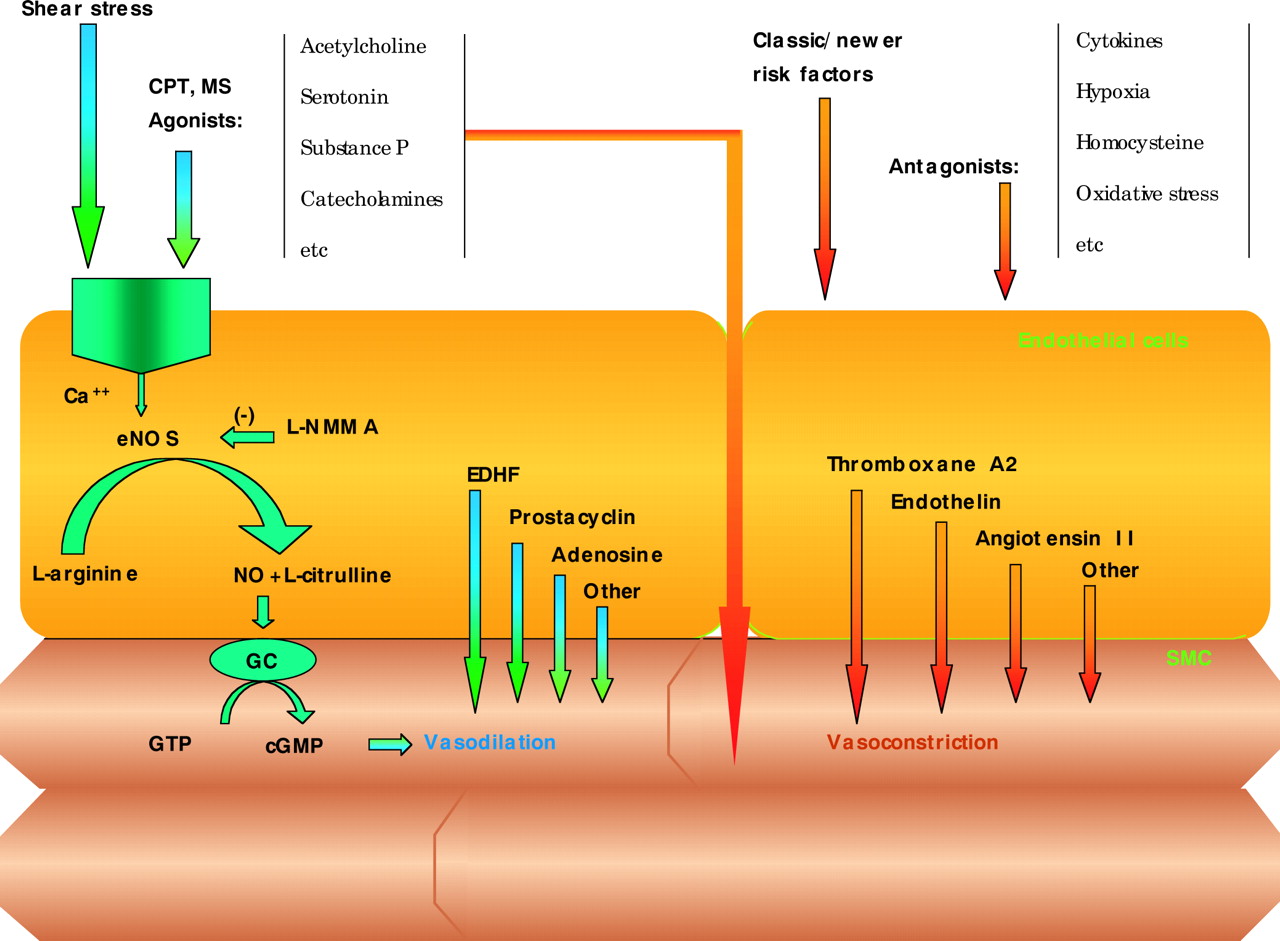
The endothelium regulates vascular homeostasis through the release of a variety of autocrine and paracrine substances, such as nitric oxide (NO), prostacyclin, and the endothelium derived hyperpolarising factor(s).1 Beyond its vasodilatory effects, NO has antiatherogenic properties, inhibits platelet aggregation and adhesion, smooth muscle cell proliferation, leucocyte adhesion, vascular permeability, and inflammatory mechanisms (fig 1).1

Effects of different stimuli (physical or chemical) on vascular endothelium. Stimuli leading to vasorelaxation in the presence of intact vascular endothelium (such as acetylcholine), produce vasoconstriction when acting directly on the underlying smooth muscle cells, in vascular areas with injured endothelium. CPT, cold pressor stress test; EDHF, endothelium derived hyperpolarising factor; eNOS, endothelial nitric oxide synthase; GC, guanyl cyclase; L-NMMA, NG-monomethyl-L-arginine; MS, mental stress; NO, nitric oxide; SMC, smooth muscle cell.
Several prospective and retrospective studies have shown that evaluation of endothelial function may be useful in identifying subjects at high risk for atherosclerosis, as well as for risk stratification of patients with already established coronary artery disease.2w1 Several invasive and non-invasive techniques have been developed during the last few years to evaluate endothelial function. Invasive techniques, which involve intracoronary or intrabrachial infusions of vasoacting agents, are still considered to be the gold standard for early detection of endothelial dysfunction. In addition, several non-invasive techniques have been developed, with comparable results and good reproducibility. In this article we describe and evaluate the different methods for assessing endothelial function in humans.
INVASIVE TECHNIQUES FOR ASSESSING ENDOTHELIAL FUNCTION
Intracoronary infusions of vasoactive agents
Intracoronary agonist infusion, combined with quantitative angiography, is the method of choice for direct quantification of endothelial function in the coronary arteries, since it allows both the evaluation of dose–response relations of endothelial agonists and antagonists, as well as assessing the basal endothelial function by the infusion of nitric oxide synthase (NOS) inhibitors.2 It is well known that intracoronary infusion of acetylcholine dilates normal coronary arteries in the presence of intact endothelium, through a receptor mediated stimulation of NO production by endothelial cells (fig 1).2w1 However, in the presence of endothelial dysfunction acetylcholine leads to vasoconstriction as a result of its direct effect on the underlying smooth muscle cells (fig 1).3w2 Briefly, a Doppler tipped guidewire is placed in the proximal segment of a coronary artery (usually at the proximal segment of the left anterior descending coronary artery), through a 6 French Judkins catheter, and the Doppler flow velocity is continuously recorded. Acetylcholine is infused in the coronary artery through the Judkins catheter at increasing rates (for example, 1, 3, 10, and 30 μg/min) while normal saline is co-infused with acetylcholine as a vehicle, and the total infusion rate is kept constant by the use of an arterial infusion pump.w3 Each dose is infused for 1–2 minutes. Coronary blood flow velocity is measured by an on-line spectral analyser and recorded on tape. Volumetric coronary blood flow is calculated with the formula validated by Doucette and colleagues.4 Endothelial function is finally evaluated by analysing the dose–response curves.
Coronary arteries with normal endothelium dilate in a dose dependent way, while in the presence of endothelial dysfunction, acetylcholine may lead to a decreased vasodilatory response or even vasoconstriction of the coronary artery. Co-infusion of NG-monomethyl-L-arginine (L-NMMA), an NOS inhibitor, blocks the vasodilatory effect of acetylcholine (fig 1).5,6
Instead of acetylcholine, intracoronary infusions of other vasoactive substances such as bradykinin, serotonin, or substance P have also been used as stimuli for NO production. The vasodilatory effect of acetylcholine or other vasodilators is usually compared with the response to glyceryl trinitrate, an exogenous source of NO leading to endothelium independent dilation of the vessel.5,6
Although intracoronary studies are considered to be the gold standard for early detection of endothelial dysfunction in the coronary arteries, they have the disadvantage of being invasive and expensive, with the risks of coronary catheterisation, and cannot be used as a screening test in the general population.2w4
Intrabrachial infusion of vasoactive agents
It has been shown previously that endothelial function in the coronary arteries is closely related to endothelial function in peripheral arteries such as the brachial artery.7 Therefore, the technique of intracoronary infusions of vasoactive agents can also be applied in the brachial artery, which is easily accessible and its cannulation has fewer potential dangers and complications.
A polyethylene cannula (usually 21 gauge) is inserted into the brachial artery under local anaesthesia (2% lidocaine) and it is connected through stopcocks to a pressure transducer for simultaneous monitoring of systemic mean blood pressure and heart rate. Forearm blood flow (FBF) is measured by gauge-strain plethysmography (preferably simultaneously in both experimental and contralateral forearms).8 During each FBF determination, the circulation of the hand is excluded for one minute before and during the measurements, by inflation of a paediatric cuff around the wrist at suprasystolic blood pressure.
After cannulation, the patient remains at constant room temperature (22–24°C), and usually normal saline is infused at a constant rate (usually 2 ml/min is sufficient for adults). After a 30 minute period of normal saline infusion, 10 subsequent measurements of FBF are performed and the mean baseline FBF is estimated. After the determination of baseline FBF, acetylcholine is infused in the brachial artery with a gradually increasing infusion rate (for example, 3, 12, 24, and 48 μg/min) by the normal saline displacement method, where the total pump infusion rate remains constant (for example, at 2 ml/min) with a simultaneous decrease of the normal saline infusion rate. Each infusion rate of acetylcholine remains constant for five minutes (three minutes before and during the two minutes of each FBF determination). FBF under acetylcholine infusion is measured as the average of at least three consecutive steady state measurements at the end of each infusion period.9 Each dosing is followed by a 30 minute resting period (with normal saline infusion at a constant rate) before the next dosing effect is evaluated, to allow the vascular endothelium to return to rest levels. The same protocol is usually repeated with nitroprusside infusion instead of acetylcholine, for evaluation of endothelium independent dilatation. The infusion rate of nitroprusside is selected to create a similar vasodilatory effect on the healthy vessels, to that of acetylcholine. The changes in FBF during acetylcholine or nitroprusside infusions represent indexes of endothelium dependent and endothelium independent dilation, respectively, while the respective graphs allow a more extensive evaluation of the response of the brachial artery to the two vasodilatory stimuli.10 To evaluate the NO availability, acetylcholine infusion is repeated under simultaneous constant intra-arterial infusion of L-NMMA, an NO synthase inhibitor.6,10
This method is highly reproducible, since previous studies have shown a variation of 5–8% in the short term evaluation (two hour intervals) as well as in the longer term (three week intervals).11 The method of intrabrachial vasodilator infusion, although reliable, reproducible, and easily applied, still remains an invasive method with potential side effects such as injuries of the median nerve or the brachial artery.2
NON-INVASIVE TECHNIQUES FOR ASSESSING ENDOTHELIAL FUNCTION
Recently, a number of non-invasive techniques have been developed to assess endothelial function in humans. These techniques are easily applied in humans, and can be used as screening tests for identification of early onset atherosclerosis. They are usually applied to the arm or forearm and evaluate endothelial function in the brachial artery or the resistance vessels of the upper arm.
High resolution ultrasound: assessment of endothelium dependent flow mediated vasodilation
Peripheral arteries, especially the brachial artery, respond to physical and chemical stimuli by adjusting vascular tone and regulating blood flow (fig 1).12 Increased blood flow in peripheral arteries leads to increased shear stress stimuli, increased NO production, and vasodilation.12 The vasodilatory response of the brachial artery to increased shear stress is called flow mediated dilation (FMD), and reflects the ability of vascular endothelium to produce NO.12 The role of NO in shear stress mediated vasodilation has been established by the administration of eNOS inhibitors such as L-NMMA.w5 L-NMMA infusion into the brachial artery decreases FMD by 85–95%, indicating that NO is the main mediator of this phenomenon.w5 FMD is almost completely blocked by L-NMMA when the ischaemia cuff is placed at the wrist, while the phenomenon is less NO specific when the ischaemia cuff is placed at the upper arm.w5 Other internal molecules such as endothelium derived prostanoids or endothelium derived hyperpolarising factor may also contribute to the degree of flow mediated vasodilation.13
Vasoactive drugs must be discontinued at least 12 hours before the study, and the patient must refrain from cigarette smoking for at least six hours.14 After a 12 hour fasting period, the subject is positioned in a supine position, in a quiet room under constant temperature, with the arm in a comfortable position for assessing the brachial artery, and must remain under constant conditions for at least 10 minutes. The brachial artery is imaged above the antecubital fossa in the longitudinal plane, by using a linear array transducer (with frequency 7–12 MHz) attached to a high quality mainframe ultrasound system (fig 2). The diameter of the brachial artery is initially determined at rest, and blood flow is estimated by time averaging the pulsed Doppler velocity signal obtained from a mid artery sample volume (fig 3). The diameter of the brachial artery is determined manually with electronic calipers or automatically using edge detection software. To decrease the variability of the measurements, the brachial artery diameter should be determined by the average derived from multiple diameter measurements along a segment of the vessel.
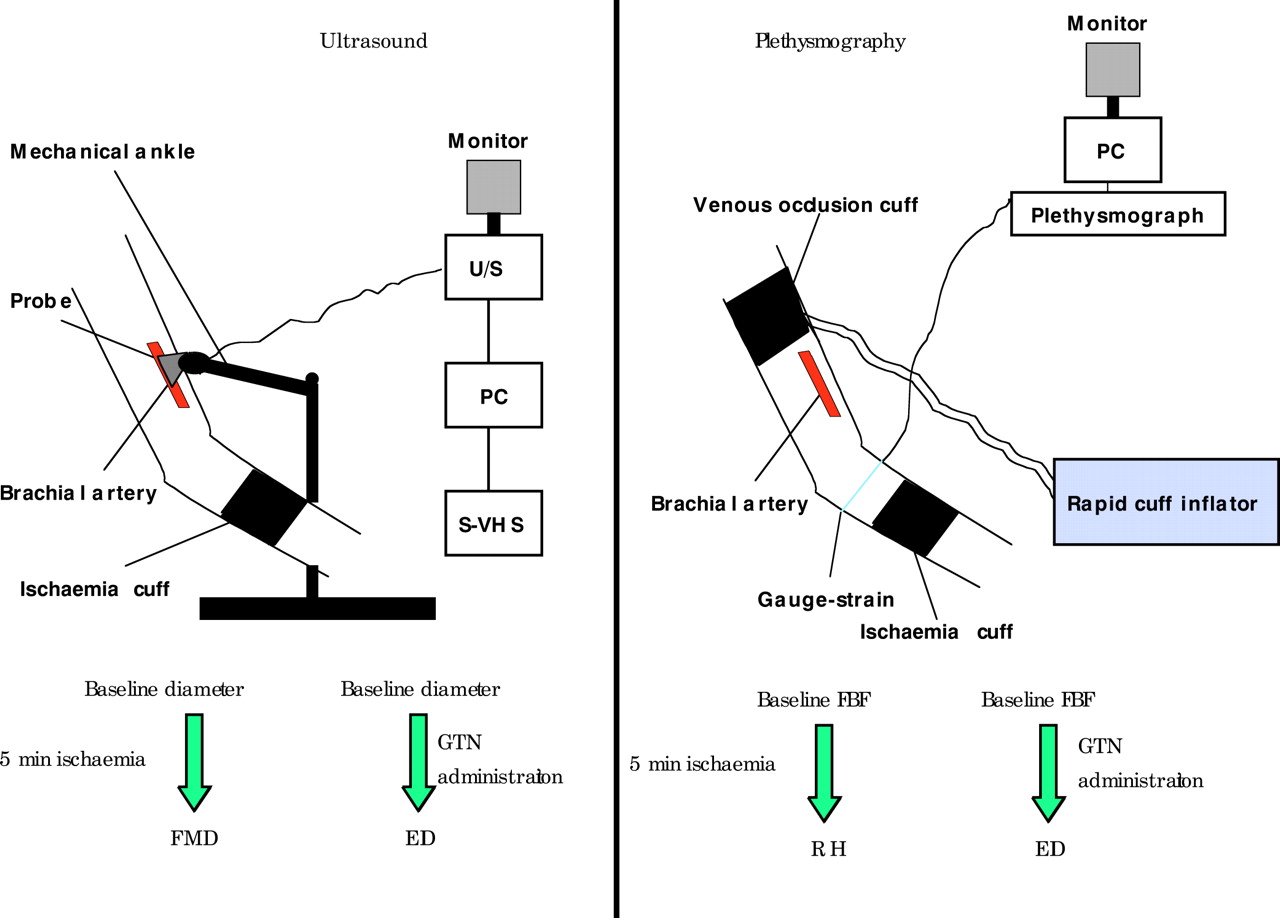
Technical aspects of the non-invasive methods for evaluating endothelial function. Flow mediated dilation is evaluated by the use of high resolution ultrasound (left panel), while gauge-strain plethysmography evaluates the changes in forearm blood flow during reactive hyperaemia. EID, endothelium independent dilation; FBF, forearm blood flow; FMD, flow mediated dilation; GTN, glyceryl trinitrate; PC, personal computer; RH, reactive hyperaemia; U/S, high resolution ultrasound.

{kind=link}
{kind=link}
{kind=link}
Timetable of flow mediated dilation (ultrasound technique, panel A) and gauge-strain plethysmography (panel B). FBF, forearm blood flow; FMD, flow mediated dilation.
After baseline brachial artery diameter determination, ischaemia is produced by inflating a cuff placed at the distal forearm, at a pressure 50 mm Hg greater than the systolic blood pressure. Alternatively the ischaemia cuff can be placed at the upper arm instead of the forearm, resulting in a greater hyperaemic flow and higher brachial artery vasodilation after its release. Although it is still unclear which is the most preferable position to place the ischaemia cuff, it seems that placing it at the upper arm results in less accurate data acquisition as the image is distorted by collapse of the brachial artery and a shift in soft tissue (fig 2).w5–7
The release of the ischaemia cuff after five minutes leads to an increase in FBF, resulting in a vasodilatory effect on the brachial artery. The maximum blood flow velocity is detected by analysing mid artery pulsed Doppler signal immediately after or up to 15 seconds after cuff release, while the maximum diameter of the brachial artery is determined approximately 60 seconds after release or 45–60 seconds after the peak hyperaemic flow (fig 3).w7 Additional information may be offered by the evaluation of the “area under the curve” of the diameter versus time from ischaemic cuff release.w8 It is important to measure the diameter of the brachial artery at the same period of the cardiac cycle, to avoid any effect of arterial compliance on the measurements.14 Therefore, simultaneous ECG recordings are essential to achieve the most reliable results. Most laboratories define FMD as the percentage change of the brachial artery diameter from rest to the diameter 60 seconds after ischaemia cuff release. All the determinations are carried out on tape by two independent observers, since the brachial artery is continuously monitored from 30 seconds before to 120 seconds after ischaemia cuff release.14w7 The comparison of FMD with endothelium dependent dilation in the brachial artery, produced after glyceryl trinitrate administration, often helps to elucidate changes in smooth muscle function or arterial compliance that may affect the observed changes in FMD.14w9
The method of FMD is reproducible, with a coefficient of variation for repeated measurements of brachial artery diameter in a good laboratory of about 3–4% in short term (two hour interval) as well as in longer term (three week interval) repeated measurements.11 It has the advantage of being non-invasive, safer, and faster than invasive methods, while its results are closely correlated with endothelial function in the coronary arteries. However, it seems to be highly operator dependent, requires excellent patient cooperation, and has relatively poor resolution relative to arterial size.
Gauge-strain plethysmography (evaluation of reactive hyperaemia)
Another index currently used for the non-invasive evaluation of endothelial function in the brachial artery is evaluation of the changes in FBF during reactive hyperaemia, by the use of gauge-strain plethysmography.15,16w10 This technique is non-invasive, simple, and reproducible since its results are less observer dependent than ultrasound. The technique evaluates the percentage change of flow from baseline to the maximum flow during reactive hyperaemia following a five minute ischaemia of the distal forearm.w10 Furthermore, the evaluation of the maximum hyperaemic flow and the overall time–flow curve during reactive hyperaemia may also offer significant information in evaluating endothelial function.16
Several studies suggest that endogenous NO plays only a minor role in vasodilation during reactive hyperaemia, and that reactive hyperaemia is largely caused by endothelium related mechanisms other than NO, such as adenosine, prostaglandins, and endothelium derived hyperpolarising factor.17w11 However, there are reports that NO may contribute significantly to the late phase of reactive hyperaemia,17w12 as well as to the peak hyperaemic flow.18 It was recently shown that inhibition of NO production by L-NMMA infusion significantly decreases maximum hyperaemic flow18 as well as the total hyperaemic flow in flow–time curves by 30–50%.16,18 Although this technique leads to less specific results than FMD, it is preferred by many centres because it is easily applied and does not require highly trained personnel, and its results are less observer dependent.
The technique
FBF is measured using a mercury filled silastic strain-gauge plethysmograph. The strain-gauge is attached to the upper forearm, at the position with the maximum diameter; it is supported above the level of the right atrium and it is connected to a plethysmographic device. The upper arm congesting cuff is inflated to 40 mm Hg for seven seconds in each 15 second cycle to occlude venous outflow from the arm by using a rapid cuff inflator. The FBF output signal is transmitted to a recorder or to a personal computer, where the flow chart is plotted (fig 3). The FBF is estimated by the gradient of the tangent to the curve during the first cardiac cycles, and it is expressed in ml/100 ml of forearm tissue volume/minute. The final FBF is calculated by the mean of 10 subsequent measurements, and always by two independent observers. The intraobserver coefficient of variation must be < 4%.
A second wrist cuff is placed distal to the gauge-strain, and inflated at 50 mm Hg over the systolic blood pressure for five minutes, to produce ischaemia. The FBF is measured every 15 seconds after the release of the ischaemia cuff, and the time–flow curve is plotted (fig 2). Alternatively, ischaemia may be produced by inflating the upper arm cuff, while the wrist cuff is inflated to occlude the flow of peripheral forearm and hand during each FBF measurement. However, the use of a peripheral forearm ischaemia cuff is preferred, since it is less susceptible to errors caused by brachial artery collapse during the hyperaemic period.w5 An ischaemia period longer than four and a half minutes does not lead to a further increase in FBF.w13
With this technique, endothelial function is evaluated after the determination of the maximum blood flow during reactive hyperaemia, the percentage change of flow from rest to the maximum hyperaemic flow, as well as by the analysis of the time–flow curves during reactive hyperaemia.19 The area under the curve of the flow response during reactive hyperaemia represents the overall dilatory capacity of resistance arteries, and it is also considered to be an indirect index of endothelial function.16,19w10 w14
Beyond ischaemic occlusion of the forearm, other alternative vasodilator stimuli such as cold pressor stress (CPT) can also be used.w14 CPT leads to the release of catecholamines,20 stimulating endothelium dependent vasodilation in the brachial artery. Furthermore, blood flow velocity during CPT also plays a major role in the dilator response of peripheral arteries through the increased shear stress that enhances the release of the endothelium derived relaxing factor and/or probably endothelium derived hyperpolarising factor.w15 CPT is applied by immersing one hand in ice water for two minutes,20w16 and determination of coronary blood flow (invasive technique), FBF by gauge-strain plethysmography, or the diameter of the brachial artery by high resolution ultrasound by the end of the test. The percentage change of coronary blood flow or FBF from baseline to the maximum flow after CPT, as well as the percentage change of the diameter of the brachial artery from baseline to the diameter after the test, are also alternative indexes of endothelial function.
Evaluating endothelial function: key points
-
Endothelial dysfunction is considered to be a major step in atherogenesis
-
Early detection of endothelial dysfunction may identify subjects at high risk for atherosclerosis
-
Endothelial function can be evaluated with invasive or non-invasive techniques, applied directly into the coronary arteries or in peripheral conduit arteries
-
Endothelial dysfunction is an independent prognostic factor in patients with advanced atherosclerosis
-
Asymptomatic subjects with endothelial dysfunction require better control of risk factors
CLINICAL IMPLICATIONS
Recent data suggest that endothelial function is a useful prognostic marker in coronary artery disease patients.w17 In these patients, it has been reported that endothelial dysfunction is an independent prognostic factor and may predict future events irrespective of the angiographic severity of the disease.w17 Persisting severe endothelial dysfunction in patients with advanced atherosclerosis may require a more aggressive control of risk factors and probably modification of current medication.
Moreover, blunted endothelial function may reflect early atherosclerosis, and should lead to a detailed evaluation (and control) of all the conventional and newer (such as infection/inflammation, homocysteine, etc) risk factors. By screening with a non-invasive technique, evaluation of endothelial function may contribute to the early identification of atherosclerosis in the general population. Individuals with endothelial dysfunction require better control of their lipid profile, C reactive protein, serum glucose, blood pressure, and smoking, since it is well known that all these factors affect endothelial function significantly.
CONCLUSIONS
Assessment of endothelial function with both invasive and non-invasive techniques in the peripheral circulation is now believed to be a window to the coronary arteries. The improvement of non-invasive techniques and the training of personnel may contribute to the early detection of high risk subjects or vulnerable patients, leading to the prevention of coronary atherosclerosis or coronary events.
REFERENCES
Supplementary materials
Web-only References
The references are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement: