Article Text

Statistics from Altmetric.com
Type 2 diabetes is by far the most common form of diabetes mellitus, and is estimated to reach epidemic proportions within the next 20 years. Diabetes is now considered an inflammatory, atherothrombotic, insulin resistance syndrome. Genetic predisposition may be important but the dominant factors seem to be the environmental triggers: diet, lifestyle, and ageing.
Atherosclerosis is the most persistent threat to the diabetic patient. Cardiovascular risk is particularly high, with ischaemic heart disease and stroke claiming the lives of 2–4 times as many people as in the non-diabetic population; also, more symptomatic forms of peripheral arterial disease are present in people with diabetes.
The optimal approach for diabetes management should be multifactorial and aggressive. It is just as important to achieve tight glycaemic control in order to limit microvascular disease, as it is to intervene against concomitant risk factors (hypertension, dyslipidaemia, obesity, smoking, etc) to stop atherosclerotic disease progression. Promotion of better patient lifestyle (exercise and diet) is also important.
Symptomatic and high risk cardiac patients may need revascularisation procedures, aimed at reducing ischaemic complications and improving quality of life, with an expected favourable impact on prognosis.
ATHEROSCLEROTIC BURDEN IN DIABETICS
Physicians facing the problem of selecting the revascularisation option in diabetics need to consider the global atherosclerotic burden, which may play the most important role in prognosis.
Activation of hyperglycaemia, excess free fatty acid release, and insulin resistance impair endothelial function in diabetes. By decreasing nitric oxide and increasing endothelin-1 and angiotensin II concentrations, both vascular tone and vascular smooth muscle cell growth and migration are increased. The activation of transcription factors induces inflammatory gene expression and increased production of inflammatory cytokines. Moreover, the increased production of tissue factor and plasminogen activator inhibitor-1 creates a prothrombotic milieu, while decreased endothelium derived nitric oxide and prostacyclin favours platelet activation. All these mechanisms lead to atherogenesis and accelerated atherosclerosis, with plaque rupture or erosion more susceptible to thrombotic occlusions.1
Particular clinical and angiographic features of the diabetic patient may point to a worse prognosis following revascularisation procedures. Older age, female sex, low body mass index, hypertension, peripheral arterial disease, and renal failure are some of the main clinical adverse features seen in diabetics. Smaller vessel size, more severe and diffuse pattern of disease, and increased coronary artery calcification have all been reported in diabetics.
It has been considered that patients with diabetes carry the same level of risk for subsequent acute coronary events as non-diabetic patients with previous myocardial infarction (MI). Diabetes worsens early and late outcomes in acute coronary syndromes, and long term outcomes after percutaneous or surgical revascularisations are probably worse for patients requiring insulin.
CORONARY REVASCULARISATION OPTIONS IN DIABETICS
Selection of the best myocardial revascularisation strategy for diabetics with multivessel coronary artery disease (CAD) has proven controversial. Data accumulated over the years are derived from subgroup, post-hoc analysis of diabetics included in randomised controlled trials (RCTs) or from single and multicentre registries.
Strict vessel and patient selection for RCTs do not resemble the complex diabetic population seen in daily practice. Moreover, constant progress is being made, not only in surgical techniques but also in interventional devices and pharmacological treatments, making it difficult to extrapolate previously reported data to the present day. Meta-analysis, with more statistical power, does not allow for a systematic evaluation of important biological confounders (diabetes control, lipid concentrations, blood pressure, or inflammatory markers) that may affect outcomes.
There has never been an RCT comparing coronary artery bypass surgery (CABG) and either balloon or stent percutaneous coronary intervention (PCI) conducted exclusively in diabetic patients.
CABG versus balloon PCI
Particular emphasis has been placed on the results of the BARI trial, where 353 diabetic patients were included between 1988 and 1991 and randomised between CABG and balloon PCI. The five year mortality was significantly lower with CABG (19.4% v 34.5%), which was attributed almost entirely to cardiac death (5.8% v 20.6%). The CABG benefit was more apparent among patients requiring insulin and was limited to patients who received left internal mammary artery (LIMA) grafts. The main explanations for better outcomes in surgical patients were the completeness of revascularisation, the use of LIMA grafts, and the protective effect among diabetics with MI caused by reocclusion of dilated arteries.
However, these results were not duplicated in the BARI Registry (patients eligible but not randomised by physician’s option), with similar outcomes in diabetics treated either by CABG or PCI; a meta-analysis combining data from all diabetic patients (n = 537) of three RCTs showed that the higher mortality observed after PCI at four years diminished over time and was not maintained at 6.5 years.
Data from 13 RCTs involving 7964 patients, comparing CABG to PCI, showed a risk difference in mortality of 2.0% favouring CABG, only observed at five years, but no differences in MI rates. There was, however, a higher risk difference for additional revascularisation procedures following PCI (38% to 24%), mainly in the first year.2
Restenosis was not only the main reason for the higher repeat revascularisation rates in diabetics, but also a major determinant of long term prognosis after balloon PCI, with occlusive restenosis in diabetics being a strong independent correlate of total and cardiac mortality.
Although with disputable long term benefit on mortality, no difference in MI rate, but a lower need for new revascularisations, CABG was considered, relative to balloon PCI, the preferred option for diabetics with multivessel CAD.
Stents versus balloon PCI
Stents made real progress in PCI techniques by improving immediate outcomes and controlling two recognisable factors responsible for restenosis—elastic recoil and negative remodelling.
A meta-analysis of 29 RCTs between stenting and balloon PCI, involving 9918 patients, showed a 48% reduction of angiographic restenosis and 41% of new PCIs, with no impact on the rates of death and MI or the need for CABG.3
Restenosis after stenting, caused by neointimal hyperplasia, remains the persistent limiting factor, which is particularly important for the diabetic population. In a meta-analysis of six studies, including 1166 diabetic patients with stent PCI, the average restenosis rates among patients with diabetes was 36.7%.4 In this study it was found that ageing alone could influence restenosis rates in diabetics. Many other predictors of restenosis in diabetics after stenting were described, such as smaller reference diameter, greater stented length, and reduced body mass index, with vessel calibre affecting the predicted risk of restenosis incrementally.
Overall, diabetes was found to be an independent predictor of one year mortality, MI, and target vessel revascularisations (TVR) after stent PCI, in one study due to the higher rate of new lesion formation, particularly in treated vessels.
CABG versus stent PCI
Of several published RCTs comparing CABG with stent PCI, the ARTS I trial seems particularly relevant. In this study, there were 208 diabetic patients recruited in 1997–98. The recently published five year outcome results in diabetics showed no significant differences in mortality, stroke, or MI rates. Only the overall major adverse cardiac and cerebrovascular event (MACCE) rate was significantly higher, a difference largely attributable to the need for further revascularisation, either by CABG or by PCI.5
Although the study was underpowered to detect differences in mortality between diabetics and non-diabetics, within the stent group diabetic patients had a significantly higher mortality (13.4% v 6.8%) and MACCE rate than non-diabetic patients, again with a higher rate of repeat revascularisation in diabetics (42.9% v 27.5%).5
In spite of the significant impact of stents in the reduction of restenosis and the need for subsequent revascularisations within the first year, diabetic patients continue to have high in-stent restenosis rates and diabetes continues to be an independent risk factor for adverse outcomes. Therefore, in the bare metal stent (BMS) era, surgery remained the preferred therapy for diabetic patients with multivessel CAD.
ADJUNCTIVE AND CONCOMITANT TREATMENTS IN DIABETICS
Protection against thrombotic complications is particularly important in diabetic patients undergoing PCI. Aspirin treatment is considered standard care before revascularisation and should be taken life long. Adding aspirin to adenosine diphosphate receptor antagonists (ticlopidine or clopidogrel) has a synergistic effect, leading to enhanced inhibition of platelet aggregation and improved prognosis following PCI with stents. Although no study has been performed specifically in diabetics, the dual antiplatelet regimen of aspirin and a thienopiridine, with clopidogrel being the thienopiridine of choice, has now been implemented.
Regarding the combination of stents with abciximab, a pooled analysis from three early trials (n = 1462) in diabetics showed a 2% absolute one year mortality reduction (from 4.5% to 2.5%) and an MI rate reduction (from 11.6% to 6.0%) that was more evident in patients receiving insulin.6 In the diabetic subgroup of the EPISTENT trial with 491 patients, significant benefits of stenting with abciximab were seen in TVR rates at one year.
More recently, the ISAR SWEET trial enrolled 701 diabetics (29% insulin treated) undergoing elective PCI (80% BMS, 10% balloon, and 10% drug eluting stents (DES)), following pre-treatment with 600 mg clopidogrel less than two hours before procedure, that were randomly assigned to abciximab or placebo. The combined end point of death and MI at one year was similar but angiographic restenosis was significantly lower in the abciximab group (28.9% v 37.8%) as well as the incidence of target lesion revascularisation (TLR) (23.2% v 30.4%).7
This study was underpowered to establish a mortality benefit with abciximab, but, as in EPISTENT, raised the question of its additional benefit on the restenotic process. Abciximab may have anti-inflammatory effects on leucocyte MAC-1 and antiproliferative effects on the vitronectin receptor on platelets and smooth muscle cells, which are particularly important for diabetics.
Many questions regarding the antiplatelet regimen remain to be answered, particularly in the DES era. The optimal dosing of clopidogrel, its timing of initiation, and the duration of treatment after PCI remains unknown. Because of resistance to clopidogrel in some patients, new and more potent agents are being tested (prasugrel). High risk diabetic patients are certainly the main candidates for intravenous abciximab to reduce the risks of acute events (ad hoc PCIs, when pre-treatment with clopidogrel is not possible, and for “high risk” procedures) and because of its potential benefits on restenosis and mortality.
Apart the adjunctive PCI antithrombotic treatments, other important concomitant medication should be considered in diabetic patients.
Firstly, glycaemic control might improve PCI outcomes and an optimal glycaemia (HbA1c ⩽ 7%) has been associated with a lower rate of TVR, cardiac rehospitalisation, and recurrent angina in diabetic patients undergoing elective PCI.8 Thiazolidinediones, a new class of insulin sensitising agents, have shown promise in reducing intimal hyperplasia and clinical restenosis rates in diabetics with stent PCI, an effect that may be independent of glycaemic control and related to the anti-inflammatory properties of the drug.9
For achieving long term benefits in diabetic patients, appropriate control of hyperlipidaemia and hypertension are mandatory. Angiotensin converting enzyme inhibitors and statins have been shown to improve vascular outcomes independently of their effect on blood pressure or lipid status.
DRUG ELUTING STENTS FOR PCI IN DIABETICS
The most recent advance in PCI has been the introduction of stents which elute antiproliferative agents to reduce neointimal hyperplasia. Theoretically they should be ideal for diabetic patients where the restenosis limitation of PCI is more acute. We are, however, in the initial clinical application phase and our knowledge of their real impact on mortality in diabetics is still limited.
Drugs
The first consideration is that DES have different stent platforms, different polymers to carry the drug, and different drugs. Most of the clinical experience with DES comes from the Cypher (sirolimus) and Taxus (paclitaxel) stents, introduced on to the market in 2002 and 2003, respectively.
Sirolimus or rapamycin, used in the Cypher stent, is a macrocyclic lactone with antiproliferative and anti-inflammatory properties. It is a pro-drug that binds to the immunophilin FK506-binding protein 12 and afterwards to a specific cell cycle regulatory protein, mTOR (mammalian target of rapamycin), inhibiting its activation. mTOR is involved in the transition between the G1 and S phase of the cell cycle, in which DNA replication occurs. Therefore, sirolimus has a cytostatic effect and induces cell cycle arrest in the late G1 phase (fig 1). Sirolimus has been shown to inhibit all phases of the restenosis cascade. Inflammation is notably reduced in parallel with the inhibition in neointimal hyperplasia formation, there is inhibition of total protein and collagen synthesis, and there is also inhibition of smooth muscle cell (SMC) migration, promoting a contractile rather than a proliferative phenotype. The stents use a non-erodable methacrylate co-polymer matrix for controlled drug delivery. Sirolimus is effective over a range of doses (18–1200 μg/18 mm stent) and the current dose applied on the stents of 140 μg/cm2 is well below toxic values. The controlled release of sirolimus lasts four weeks.
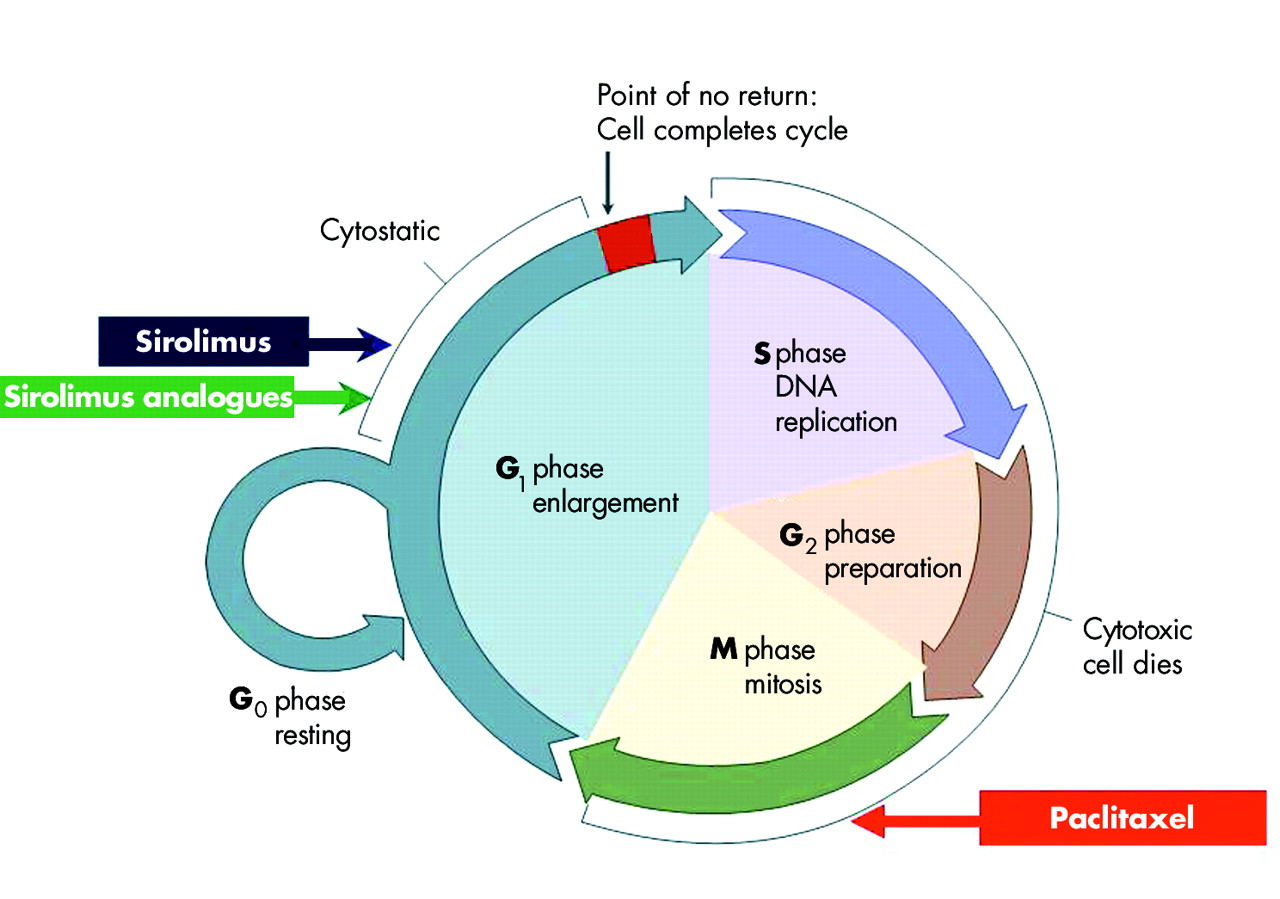
Diagram of the cell cycle, showing the different phases where sirolimus or its analogues (phase G1) and paclitaxel (phase M) exert their mechanisms of action.
Paclitaxel, used in the Taxus stent, is a naturally occurring compound isolated from the bark of the Pacific yew tree. Paclitaxel is highly lipophilic and hydrophobic, binds specifically to the β-tubulin subunit of microtubules rendering them non-functional, and by this mechanism interrupts various steps in the cell cycle, inhibiting cell replication and migration, and signal transduction. As an antimitotic, it acts on the G2/M phase of the cell cycle (fig 1), but cell killing is dependent on both drug concentrations and duration of cell exposure. The paclitaxel action on microtubules and the modulation of cell mitogenesis, independent of mTOR, may be particularly effective in the diabetic patient, inhibiting both insulin dependent and independent pathways specifically upregulated in the diabetic restenotic cascade. Stents eluting paclitaxel need a polymer delivery system to control drug release because of its narrow toxic therapeutic window and hydrophobic properties. Paclitaxel is loaded onto stents at a dose density of 1.0 μg/mm2 with total doses depending on stent length. There is an initial burst release in the first 48 hours followed by a sustained low level release (slow release formulation, only available for clinical use) for 10 days, but > 80% of the drug remains unreleased from the polymer coating.
Initial experiences with non-polymeric paclitaxel eluting stents evaluated in the ELUTES trial (V-Flex Plus, Cook) and the DELIVER trial (RX Achieve, Guidant) as well as with moderate release formulation of polymeric paclitaxel evaluated in the TAXUS II and VI trials have been published, but these stents have not been produce commercially.
The third DES recently approved in Europe is the Endeavor stent which uses zotarolimus (ABT-578). Zotarolimus is a tetrazole containing macrocyclic immunosuppressant and potent antiproliferative agent. It is the first new chemical entity specifically engineered to be delivered from stents. It is a sirolimus analogue, antiproliferative by G1/S blockade in the cell cycle (fig 1), is strongly lipophilic, and has extremely low water solubility. The stent is coated with a biocompatible non-thrombogenic phosphorylcholine polymer that does not initiate an inflammatory response. ABT-578 is loaded at a dose of 10 μg/mm of stent. Rabbit iliac models showed that 56% of total drug content was eluted within 24 hours, then gradually eluted to 97% by day 7, reaching 100% by day 14.
Other DES with sirolimus analogues—tacrolimus used in the Janus stent and tested in the JUPITER I and II trials, everolimus used in the Guidant XIENCE stent with an erodable polymer and tested in the SPIRIT I trial, and biolimus A9 used in the BioMatrix stent with a bioabsorbable polymer and tested in the STEALTH trial—are still at the pre-marketing phase.
All these drugs are partially similar to sirolimus, with changes in chemical structure to increase lipophilicity and to cause variable cell growth inhibition or toxicity.
Clinical results with DES
Several main pivotal trials comparing different DES with different BMS in selected populations undergoing PCI have been recently published or presented, with significant reductions in restenosis rates (fig 2), in TLR (fig 3), and in major adverse cardiac events (MACE) (fig 4).

Comparison of binary restenosis rates obtained in randomised clinical trials between drug eluting stents (DES) and bare metal stents (BMS). RAVEL, SIRIUS, C-SIRIUS, and E-SIRIUS with sirolimus; TAXUS I, II, and IV with slow released paclitaxel; ENDEAVOR with zotarolimus; and SPIRIT FIRST with everolimus.

Comparison of target lesion revascularisation (TLR) rates obtained in randomised clinical trials between drug eluting stents (DES) and bare metal stents (BMS). Trials as in fig 2.

Comparison of major adverse cardiac events (MACE) rates obtained in randomised controlled trials (RCTs) between drug eluting stents (DES) and bare metal stents (BMS). Trials as in fig 2.
A recent meta-analysis including 11 eligible trials (four with non-polymeric paclitaxel) and involving 5103 patients has shown remarkable risk reductions of 82% for restenosis rates (8.9% v 29.3%), 74% for TLR (4.2% v 13.2%), and 58% for MACE (7.8% v 16.4%) with DES compared to BMS at 6–12 month follow up.10 Pooled mortality (1% v 0.9%) and MI (2.7% v 2.9%) rates were low for both DES and BMS, with no differences between them.
Therefore, DES has entered into generalised routine use because of the improvement in the rate of restenosis and repeat revascularisations, both influencing the overall MACE rate.
Six RCTs including 3669 patients have also been performed comparing sirolimus with paclitaxel eluting stents. In a recent meta-analysis of these trials, restenosis (9.3% v 13.1%) and TLR (5.1% v 7.8%) rates were significantly lower with sirolimus eluting stents. No differences were found in regards to death (1.4% v 1.6%) and death and MI (4.9% v 5.8%).11
It is important to remember that the patients included in these initial trials were low risk, with single de novo lesions, and only a small proportion were diabetics (11–25%). The trials were, however, important for establishing the efficacy of the DES.
Safety concerns (DES thrombosis)
The possibility of increased rates of stent thrombosis after DES has been a matter of concern and can be particularly pertinent to diabetic patients.
Several factors related to stents (drug kinetics, delayed endothelisation, hypersensitivity to polymer, etc), procedure (underexpansion, residual stenosis/dissections, small, multiple and stent length, bifurcations, overlapping, etc), patients (primary PCI in cardiogenic shock, diabetes, renal failure, etc), and antiplatelet treatment (premature discontinuation, drug resistance, etc) can be implicated. In a meta-analysis of 10 randomised studies comparing DES with BMS published before June 2004, the incidence of stent thrombosis was not shown to be increased in patients receiving DES (0.58% v 0.54%), even late stent thrombosis (> 30 days) (0.23% v 0.25%), although there was a significant relation with stented length.12 The incidence of stent thrombosis was found to be similar in the meta-analysis of randomised head-to-head clinical trials between sirolimus and paclitaxel eluting stents (0.9% v 1.1%), with an overall proportion of diabetics of 31.6%, but with reduced power to draw any definitive conclusions about safety.11
Using registry data from Rotterdam, including all possible cases of stent thrombosis (with angiographic documentation or with sudden death and MI not clearly attributable to another coronary lesion), the incidence was similar among BMS (1.4%), sirolimus eluting stents, (1.5%) and paclitaxel eluting stents (1.6%).13 Diabetes was the only predictor of stent thrombosis by univariate analysis. In another important multicentre registry, the nine month cumulative stent thrombosis rate was 1.3% (0.8% with sirolimus and 1.7% with paclitaxel); diabetes was an independent predictor of subacute stent thrombosis (from procedure to 30 days), but not of late thrombosis, the main predictor being premature antiplatelet treatment discontinuation.14
Therefore, stent thrombosis does not seem to be increased with DES, but the clinical consequences can be dramatic. In the Rotterdam registry data, 30 day mortality was 15%, whereas another 60% of individuals suffered non-fatal MI.13 For the other multicentre registry, the case fatality rate at follow up was 45%, with presentation as death in 24%, as non-fatal MI in 69%, and as unstable angina in 7%.14
Because late stent thrombosis is still a real possibility and data on diabetics are limited, empirical clinical recommendations are for a longer use of dual antiplatelet treatment in diabetics, eventually for life.
Clinical results with DES in diabetics
The available information regarding the use of DES in diabetic patients is still scarce. Most of the data come from published subgroup analysis of RCTs between DES and BMS, and registry data from single or multiple centres.
In the SIRIUS trial15 there was a subgroup of 131 diabetic patients (26% of the total population) with sirolimus eluting stents, and the TAXUS IV trial16 included 155 diabetic patients (32% of the total population) with paclitaxel slow release stents (33% of the diabetics were insulin treated). Reference vessel diameters (2.75 mm and 2.72 mm) and lesion lengths (14.5 mm and 14.2 mm) were similar in the diabetics of these two trials. The clinical benefits of DES at 12 months were also confirmed in diabetics, with significant risk reduction regarding BMS and low rates of TLR (6.9% and 7.4%), TVR (9.9% and 11.3%), target vessel failure (TVF) (12.2% and 15%), and MACE (9.2% and 15.6%). Mortality and rates of MI were similar. There were no differences in clinical events comparing insulin treated (ITDM) with non-insulin treated diabetics (NITDM), although, unexpectedly, the TLR rates were lower in the ITDM patients of TAXUS IV trial. The results from these two trials may not be comparable, however, as the angiographic follow up was very different (67% in SIRIUS and 32% in TAXUS IV).
From the SIRIUS trial, a diabetic patient who was treated with a sirolimus eluting stent was at a lower risk of repeat revascularisation at nine months than a non-diabetic patient who was treated with a BMS but, by multivariate logistic regression model, diabetes continued to be an independent predictor of the need for repeat revascularisation.
This was also confirmed by the ARTS II study, a prospective multicentre registry of multivessel PCI patients with sirolimus eluting stents, matched to the randomised patients included in ARTS I to allow a comparison with the surgically treated diabetic patients. In the subgroup of 367 diabetic patients, the one year MACE rate was 15.7%, similar to the MACE rate in the CABG group (14.6%) of ARTS I. There were no differences in death (2.5% with sirolimus eluting stents in ARTS II v 2.1% with CABG in ARTS I), cerebrovascular accident (0% v 5.2%), or MI (0.6% v 2.1%), but the need for repeat revascularisation was still significantly higher (12.6% v 4.2%).17
Data from the single centre prospective Cypher (RESEARCH) and Taxus (T-SEARCH) Registries in Rotterdam for “real life” diabetic patients with de novo coronary lesions was recently published.18 There were 293 patients with diabetes (18% of the total population) treated with sirolimus (n = 145) or paclitaxel (n = 148) eluting stents. The two populations were relatively similar in clinical variables, but there was prolonged use of clopidogrel and significantly higher use of glycoprotein IIb/IIIa inhibitors in the paclitaxel eluting stent group compared with the sirolimus treated patients (28% v 18%, respectively). At one year, there were no differences between sirolimus and paclitaxel eluting stents in the clinical events of MACE, rate of death + MI, TLR, and TVR. Mortality was similar in ITDM (11.6%) and in NITDM (6.2%), and the MACE rate was only significantly higher in ITDM by univariate analysis (27.4% v 14.6%).
Only two randomised trials exclusively with diabetic patients have been published so far, with an angiographic primary end point at nine months.
The first, the DIABETES trial, was a prospective, randomised study comparing sirolimus eluting stents and BMS in four Spanish centres, and included 80 diabetic patients (26 insulin treated) with sirolimus eluting stents. Reference vessel diameter was smaller than in the subgroups previously reported (2.34 mm) but lesion length was similar (15.0 mm). Clopidogrel was given for one year and glycoprotein IIb/IIIa inhibitors were used in 59% of patients. At nine months, TLR (7.3%) and MACE (11.3%) rates were significantly reduced.19
The second was the ISAR-DIABETES, a prospective non-inferiority trial, in two German centres which included 250 diabetic patients randomised between June 2003 and March 2004 to receive sirolimus (n = 150) or paclitaxel (n = 150) eluting stents.20 Vessel size was similar (2.70 mm in sirolimus and 2.75 mm in paclitaxel) as well as lesion length (13.8 mm in sirolimus and 12.4 mm in paclitaxel). Clopidogrel was given at a loading dose of 600 mg and 75 mg/daily for at least six months and abciximab was used in 19.6% of patients. It was found that the use of the sirolimus eluting stent in diabetics was associated with a decrease in the extent of late loss, suggesting a reduced risk of restenosis, but the study was not sufficiently powered to assess the incidence of clinical restenosis. There were no significant differences in the rates of clinical end points between the two groups (TLR was 6.4% in the sirolimus group v 12.0% in the paclitaxel group, total death was 3.2% v 4.8%, and MI was 4.0% v 2.4%).
With limited information, particularly in patients with smaller vessels and longer lesions, it can be said that DES PCI for diabetics is associated with similar relative risk reduction of restenosis seen in non-diabetics, probably favouring sirolimus eluting stents; however, despite the use of DES, diabetes still remains an independent risk factor of restenosis, need for revascularisation, and MACE.
Long term results are also unknown, making speculative any assumptions on the potential benefit of DES on mortality and rate of MI in diabetic patients. However, in diabetics there may be a trend for improvement with PCI—for example, mortality at one year in the balloon PCI arm of BARI was 11.2%, in the stent PCI arm of ARTS I it was 6.3%, and with DES PCI in ARTS II it was 2.5%.
Several ongoing randomised trials will further evaluate the optimal revascularisation approach for patients with diabetes. The BARI 2D trial, sponsored by the National Heart, Lung, and Blood Institute (NHLBI), addresses the value of revascularisation versus no revascularisation in insulin requiring versus non-insulin requiring diabetic patients with mild to moderate coronary symptoms. The FREEDOM trial, also sponsored by the NHLBI, is comparing the efficacy of a sirolimus eluting stent with adjunctive glycoprotein IIb/IIIa inhibitor abciximab versus CABG, in patients with diabetes who require multivessel revascularisation. The CARDIa trial is assessing the outcomes of diabetic patients with multivessel or single vessel disease eligible for revascularisation and treated with either a drug eluting stent or CABG surgery.
Differences in late luminal loss and their relevance to diabetics
The efficacy of DES, as assessed by TLR rates (fig 5), reveals notable differences in in-stent late luminal loss (LL) among different stents (fig 6). Therefore, the value of LL as a clinically relevant end point has been questioned. A clarification of this problem may be important, as all DES may be perceived as interchangeable at present and in the future, if only TLR rates are considered.

Target lesion revascularisation (TLR) rates in 10 different RCTs with sirolimus (blue, from RAVEL to DIABETES), in eight RCTs with paclitaxel (green, from TAXUS I to ISAR-DIABETES-PES), and one with zotarolimus (red, ENDEAVOR).

In-stent late luminal loss (LL) in different RCTs with sirolimus, paclitaxel, and zotarolimus. Same trials as in fig 5.
LL can be calculated within the stent, at its edges, or across the entire analysis segment. The value of in-segment LL may be limited by multiple confounding factors that influence luminal dimensions such as elastic recoil, vessel spasm, and remodelling.21 This heterogeneity can also be caused by variations in drug distribution, degree of injury, and tissue composition along the target vessel, and could be amplified in small vessels and in diabetics in particular. In-stent LL, by isolating the neointimal hyperplasia component of the restenosis process, has been shown to retain a strong relation with restenosis and to be a sensitive indicator of the biological antiproliferative efficacy of a given DES.22,23
Based on analysis of TAXUS IV individual patient data, median thresholds for in-stent LL (0.75–1.0 mm) and for in-segment LL (0.5–0.65 mm) were suggested, that would accommodate the probability of TLR <5–10%. This would require homogeneity of response to DES as a function of vessel size, lesion length, diabetic status, and other parameters—hardly expected to be found in diabetics—and it was said that homogeneity would be more important to predict clinical benefit than the exact amount of LL.24 Regardless of the actual and currently unknown threshold of LL difference that is clinically relevant in diabetic patients, increasing values of LL have been shown to be associated with increasing risk of TLR.25 In the only trial exclusively with diabetics, LL with a sirolimus eluting stent was 0.19 mm and with a paclitaxel eluting stent was 0.46 mm, values similar to the ones found in other trials with these DES (fig 6). Although not significant, the benefit with sirolimus eluting stents was translated in this trial into clinical benefit with reduction of TLR (6.4% v 12.0%) at nine months.20 There may be a difference between these DES, suggested in the correlation between LL and TLR in the published trials (fig 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between in-stent late loss and target lesion revascularisation (TLR) rates in the different RCTs with sirolimus and paclitaxel eluting stents. Same trials as in fig 5.
Our understanding of the complete mechanisms of restenosis after DES is still limited. The magnitude of the biological effect of DES on neointimal proliferation may unmask the contribution of other mechanical or technique related factors. Antiproliferative agents may delay the biological response to injury, prolonging endothelium denudation and limiting endothelial cell regrowth, as has been suggested with paclitaxel.21
Small differences in restenotic risk and TLR seen in current trials are likely to be amplified in practice, where the magnitude of clinical benefit is expected to increase with the risk profile of the patient population.25
Therefore, diabetes continues to represent a greater challenge to PCI, even in the DES era. In-stent LL after DES is probably reduced in diabetics to the same degree as in other patient groups, although the underlying propensity for restenosis is higher and very small vessels have not yet been studied. But patients with diabetes are at a greater clinical risk and are more likely to suffer new revascularisations and MACE than those without diabetes. In these early phases of DES use, diabetes has still been found to be an independent predictor of MACE. As suggested by others, diabetes per se may not be an independent risk factor for revascularisation, but only a convenient aggregate marker for other causal factors.26 Local variables, such as small vessels and anatomical complexity, could be more important in predicting restenosis than simply diabetes.
Diabetes is probably too complex for it to be expected that a localised treatment would influence the rate of future revascularisations and overall patient prognosis. Abnormal coronary endothelial reactivity present in diabetes is associated with an increased rate of cardiovascular events.27 The coronary arteries of diabetics are less likely to undergo the favourable remodelling in response to atherosclerosis, are less able to adapt to significant obstructive lesions, and have larger amounts of lipid-rich plaques prone to rupture. Diabetics have an impaired ability to develop coronary collaterals, are more likely to develop new coronary lesions, particularly in instrumented vessels, and have higher rates of completely occlusive restenosis after PCI. Finally, coronary artery disease in diabetics is more frequently diffuse, occurs in multiple small vessels with smaller luminal diameters in segments adjacent to obstructive coronary lesions, the lesions are longer, and there are more completely occluded segments at diagnostic coronary angiography.28
PCI with drug eluting stents in diabetics: key points
-
Diabetes is a complex inflammatory, atherothrombotic, insulin resistance syndrome, which may reach epidemic proportions in the next two decades
-
The global atherosclerotic burden in diabetes, particularly endothelial dysfunction, inflammation, and the prothrombotic state, may have a major impact on prognosis
-
Medical management of the diabetic patient should include adequate selection of pharmacological agents with vascular effects beyond glycaemic control, lowering of blood pressure or lipids, and should promote better lifestyles
-
When needed, selection of the best coronary revascularisation strategy for diabetics should be individualised, taking into account the patient’s angiographic profile, tolerability to long term dual antiplatelet treatment, and preferences and current progress with percutaneous coronary intervention (PCI) techniques and coronary artery bypass graft surgery (CABG)
-
Until now, there has never been a randomised clinical trial comparing CABG to PCI, exclusively in diabetic patients
-
With PCI, diabetics are known to have higher restenosis rates, a greater need for new interventions, and a worse prognosis than non-diabetic patients
-
The most recent advance in PCI routine clinical practice is the introduction of drug eluting stents (DES), with remarkable reductions in restenosis and need for further revascularisations of the target lesions
-
DES may be particularly suitable for diabetics, mainly those with lower in-stent late luminal loss, but the available information is still limited. Long term dual antiplatelet treatment with aspirin and clopidogrel is strongly advised
-
It should not be expected that a local treatment, aimed at relieving symptoms or ischaemia, could be solely responsible for a more favourable prognosis in diabetics
For the time being and for practical purposes, it seems sensible for in-stent LL to be the true measure of efficacy of DES, representing the best angiographic surrogate of neointimal proliferation, with the unique ability of separating it from other procedural and intrinsic vessel variables, and able to predict reliably their long term restenosis propensity. Although restenosis is not abolished with current DES, these stents should be used in all diabetics, in the hope that future research will produce better stents and drugs to make PCI the definite first option for the great majority of patients.
CONCLUSIONS
The diabetic population is particularly challenging for percutaneous coronary revascularisation because of specific high risk clinical and angiographic features. Long term events are related not only to revascularisation failures but also to progression of coronary disease and overall risk of diabetics. DES represent a real advance in PCI for diabetics, and should be used as the first choice. Compared with BMS, they have achieved highly significant suppression of neointimal hyperplasia (as measured by LL), resulting in reduction of angiographic restenosis and improved clinical outcomes. There is no evidence as yet that they will improve survival.
There are still some concerns over the use of DES for PCI in diabetics related to possible late stent thrombosis that, in “real life”, may be higher than in other subgroups of patients. Doses and duration of dual antiplatelet treatment and routine use of glycoprotein IIb/IIIa inhibitors, outside the setting of acute coronary syndromes, have not been clearly established.
Diabetes, either in itself or as a result of the complexity of the coronary anatomy, continues to be a predictor of restenosis and worse outcomes. Differences in LL observed with different DES may prove to be important in the long term, particularly in high risk populations such as diabetics.
Until results of ongoing RCTs comparing DES with CABG are available, CABG is still a valid option for a progressively smaller diabetic population with multivessel disease. Both therapeutic alternatives are acceptable and the choice between them must be made depending on individual patient and angiographic profile. When considering PCI, we should make sure that patients can tolerate long term dual antiplatelet treatment and that they are aware of the possible need for repeat interventions, mainly caused by disease progression.
Although evidence and good clinical judgment should continue to guide revascularisation choices, it cannot be expected that a local treatment will affect the metabolic abnormalities and systemic derangements seen in diabetes. Therefore, irrespective of the first coronary revascularisation strategy selected, diabetic patients do require a continuous and multidisciplinary approach to manage adequately the underlying disease and all concomitant risk factors.
MULTIPLE CHOICE QUESTIONS
Education in Heart Interactive (www.heartjnl.com/misc/education.shtml)
There are six multiple choice questions associated with each Education in Heart article (these questions have been written by the authors of the articles). Each article is submitted to EBAC (European Board for Accreditation in Cardiology; www.ebac-cme.org) for 1 hour of external CPD credit.
How to find the MCQs: Click on the Online Learning: [Take interactive course] link on the table of contents for the issue online or on the Education in Heart collection (www.heartjnl.com/cgi/collection/heart_education).
Free access: This link will take you to the BMJ Publishing Group’s online learning website. Your Heart Online user name and password will be recognised by this website. As a Heart subscriber you have free access to these MCQs but you must register on the site so you can track your learning activity and receive credit for completed courses.
How to get access: If you have not yet activated your Heart Online access, please do so by visiting http://www.bmjjournals.com/cgi/activate/basic and entering your six digit (all numeric) customer number (found above your address label with your print copy). If you have any trouble activating or using the site please contact subscriptions{at}bmjgroup.com
Case based Heart: You might also be interested in the interactive cases published in association with Heart (http://cpd.bmjjournals.com/cgi/hierarchy/cpd_node;CBH)
REFERENCES
Footnotes
-
In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article